
From the 1ACHIEVE Centre for Applied Research, Faculty of Health, Amsterdam University of Applied Sciences, 2Capri Cardiac Rehabilitation, Rotterdam, 3Amsterdam University Medical Center, Department of Cardiology, 4Cardiovitaal Cardiac Rehabilitation Centre, Amsterdam and 5Erasmus University Medical Centre, Department of Rehabilitation Medicine, Rotterdam, The Netherlands
Objectives: To determine the psychometric properties of a questionnaire to assess fear of movement (kinesiophobia): the Tampa Scale for Kinesiophobia (TSK-NL Heart), and to investigate the prevalence of kinesiophobia in patients attending cardiac rehabilitation.
Methods: A total of 152 patients were evaluated with the TSK-NL Heart during intake and 7 days later. Internal consistency, test-retest reliability and construct validity were assessed. For construct validity, the Cardiac Anxiety Questionnaire (CAQ) and the Hospital Anxiety and Depression Scale (HADS) were used. The factor structure of the TSK-NL Heart was determined by a principal component analysis (PCA).
Results: After removal of 4 items due to low internal consistency, the TSK-NL Heart showed substantial reliability (intraclass correlation coefficient; ICC: 0.80). A strong positive correlation was found between the TSK-NL Heart and the CAQ (rs: 0.61). Strong positive correlations were found between the TSK-NL Heart and de HADS (Anxiety) (rs: 0.60) and between the TSK-NL Heart and the CAQ (rs: 0.61). The PCA revealed a 3-factor structure as most suitable (fear of injury, avoidance of physical activity, perception of risk). High levels of kinesiophobia were found in 45.4% of patients.
Conclusion: The 13-item TSK-NL Heart has good psychometric properties, and we recommend using this version to assess kinesiophobia, which is present in a substantial proportion of patients referred for cardiac rehabilitation.
Key words: cardiovascular disease; Tampa Scale for Kinesiophobia; fear of movement; cardiac rehabilitation; physical activity; exercise.
Accepted Jan 28, 2020; Epub ahead of print Feb 7, 2020
J Rehabil Med 2020; 52: jrm00021
Correspondence address: Paul Keessen, Centre for Applied Research, Faculty of Health, Amsterdam University of Applied Sciences, Amsterdam, The Netherlands. E-mail: p.keessen@hva.nl
Fear of movement (kinesiophobia) in common is patients with cardiac diseases. As a consequence, these patients have lower levels of adherence to cardiac rehabilitation. It would be useful to gain more insight into kinesiophobia in cardiac patients. In order to effectively screen for kinesiophobia and to evaluate treatment for these patients, an objective measurement tool would be useful. Secondly, in order to effectively treat patients, it would be useful to determine which subgroups of cardiac patients experience kinesiophobia. The aim of this study was to determine the reliability and validity of a questionnaire to measure kinesiophobia, and to determine the level of kinesiophobia in subgroups of patients.
Physical activity (PA) is one of the cornerstones of secondary prevention of cardiovascular disease, and a core component of cardiac rehabilitation (CR) (1). Nevertheless, the percentage of cardiac patients performing the recommended amount of PA has been reported to be as low as 17% (2). A potential explanation for the low levels of PA might be the anxiety that is frequently reported after cardiac events (3). Specifically, fear of movement, also known as kinesiophobia, might be an important barrier for patients to achieve adequate levels of PA. Kinesiophobia is defined as “an excessive, irrational and debilitating fear of movement and activity, resulting from a feeling of vulnerability to painful injury or re-injury” (4). Bäck et al. reported that up to 20% of patients with coronary artery disease (CAD) develop kinesiophobia (5).
The setting of CR might be suitable, not only to identify patients with kinesiophobia, but also to develop and test interventions targeting patients with high levels of kinesiophobia. Since avoidance of PA is related to major adverse cardiac events (4), participation in CR is even more important for these patients.
Kinesiophobia can be measured using the Tampa Scale for Kinesiophobia (TSK), which is based on the fear avoidance model created by Kori et al. (6). The TSK is predominantly used in patients with musculoskeletal complaints and was adapted by Bäck et al. (7) for use in patients with CAD by replacing “fear of pain” with “fear of a heart incident” (TSK-Heart) (7). The TSK-Heart has been translated into several other languages (8, 9). However, a comprehensive external validation, including a rigorous factor analysis, and population prevalence of kinesiophobia in a large contemporary group of patients attending CR, is lacking.
The aim of this study was therefore to cross-culturally validate the TSK Heart (English to Dutch), to assess the psychometric properties of the TSK Heart, and to assess the prevalence of kinesiophobia in patients referred for CR.
Study design
A prospective study was performed with 2 time-points at Capri Cardiac Rehabilitation Rotterdam (CCRR) and Cardiovitaal Cardiac Rehabilitation Amsterdam (CCRA).
Ethical considerations
A waiver of approval was granted by the Medical Ethics Committee of the Erasmus University Medical Centre, Rotterdam (MEC-2017-1096).
Cross-cultural validation
A forward translation of the TSK-Heart was performed by NtH and IdU, and reviewed by a professional English teacher (academic level). All comments regarding the translation were independently processed by NtH and IdU. After consensus was reached, the questionnaire was reviewed by HvdBE. After the last comments were processed by NtH and IdU, the final version was reviewed in several rounds by an expert panel consisting of cardiac patients (n = 12) and CR healthcare professionals (n = 8). The panel of healthcare professionals consisted of 2 cardiologists, 2 physical therapists, 2 cardiac nurses and 2 psychologists. The expert panel was asked to respond to the relevance and formulation of the separate items on a standardized form. After each round a new version of the TSK-NL Heart was created until consensus was reached.
Patients
In order to adequately analyse all psychometric properties and to analyse differences in kinesiophobia between subgroups, this study aimed to include 150 participants.
For this study we used an “all-comers design”. All patients who were referred to CR, in CCRR or CCRA, between July 2018 and February 2019 were invited to participate in the study. Patients were eligible to participate if they were able to read and understand the Dutch language and had a valid e-mail address. Delayed participation in CR (>10 months post-event) was an exclusion criterion. All patients who agreed to participate gave written informed consent.
Procedures
Data were collected during the intake for CR (T0) and 5-7 days post-intake (T1). Patients started CR after T1. At T0 the following baseline data were collected: age, sex, cardiac diagnosis, cardiac disease history and co-morbidities. Furthermore, patients were asked to complete the following questionnaires at T0 and T1.
TSK-NL Heart. This questionnaire measures fear of movement. It consists of 17 questions with a 4-point answer scale. Minimum score is 17 and maximum score 68. A cut-off score of 37 points is used to define “low levels of kinesiophobia” (<37 points) and “high levels of kinesiophobia” (≥37 points) (7).
Cardiac Anxiety Questionnaire (CAQ). Cardiac anxiety is defined as anxiety symptoms that are triggered by specific cardiac-related stimuli and symptoms (10). The CAQ is 18-item questionnaire with a 5-point Likert scale (0–4) with a maximum score of 72. The CAQ reflects the subscales: fear, attention, avoidance of physical exercise and safety-seeking behaviour (10).
Hospital Anxiety and Depression Scale (HADS). The HADS consists of 7 items measuring anxiety (HADS-A) and 7 items measuring depression (HADS-D). A 4-point Likert scale (0–3) is used. For both subscales a score of 0–7 is defined as “no anxiety/depressive disorder”, a score of 8–10 is defined as “possible anxiety/depressive disorder”, and a score of 11–21 is defined as “likely anxiety/depression disorder”’. The HADS is a widely used tool to assess anxiety and depression in various patient groups (11). For this study we only used HADS-A.
Data were collected using a software package (Castor EDC at CCRA and GemsTracker at CCRR) for distribution of questionnaires between July 2018 and February 2019.
Statistical analysis
Descriptive statistics were used for demographic data. Continuous data were presented as mean and standard deviations (SD), if data were normally distributed. For categorical data median and range were used. All statistical analyses were performed using IBM® SPSS® v. 25.0 software.
Internal consistency
Homogeneity and the contribution of each item to the test were assessed by Cronbach’s α at T0. A Cronbach’s α value of 0.70 and a minimal corrected item correlation of 0.25 per item were classified as sufficient (12). Items with a corrected item correlation below 0.25 were excluded from the exploratory factor analysis.
Test-retest reliability
A test-retest procedure was performed on the sum score of the TSK-NL Heart and on all 17 items separately between T0–T1. If items were removed due to low internal consistency, the adjusted sum score was used. Test-retest reliability was assessed by computing the intraclass correlation coefficient (ICC) with a 2-way mixed model. The strength of reliability was classified as slight (0.00–0.20), fair (0.21–0.40), moderate (0.41–0.60), substantial (0.61–0.80), or excellent (0.81–1.00) (13).
Construct validity
External measure. Construct validity was assessed by investigating the correlation between the sum score of the TSK-NL Heart, and the sum score of the CAQ and of HADS-A at T0. The correlations were computed using the Spearman’s rank correlation. Strength of correlation was defined as small (0.00–0.29), moderate (0.30–0.49), or strong (0.50–1.00) (14).
Exploratory factor analysis. The factor structure of the TSK-NL Heart was assessed with a principal component analysis (PCA) at T0. To check whether the data were suitable for factor analysis, the “Kaiser-Meyer-Olkin Measure of sampling adequacy” (KMO) was used. A KMO value > 0.8 indicates good sample adequacy (15). Bartlett’s test of sphericity was performed to test whether the variables were unrelated and thus unsuitable for structure detection. Small values (< 0.05) reject the null hypothesis that the variables are unrelated, (15) and thus justify proceeding with the PCA. An Oblimin rotation was used to assess the data, since it was expected that the components were correlated (15). Kaiser’s criterion (eigenvalue > 1) was used to determine the number of components. Subsequently, the explained variance of the various components was assessed. A total explained variance of ≥ 60% was considered satisfactory (16).
Prevalence of kinesiophobia
The distribution of kinesiophobic scores at T0 was explored by creating amplitude probability distribution functions (APDF) for the study population as a whole. The distribution of scores in the following sub-groups was then assessed: (i) acute and elective hospitalization; (ii) interventional procedures, surgical procedures and medication only. Interventional procedures included: percutaneous cardiac intervention (PCI), transcatheter aortic valve implantation (TAVI), electro cardioversion (ECV), internal cardiac defibrillation procedure (ICD), and ablation. Surgical procedures included: aortic replacement, coronary artery bypass grafting (CABG) and CABG combined with mitral valve replacement (MVR) or aortic valve replacement (AVR). High kinesiophobic traits were defined as a TSK-NL Heart sum score ≥ 37 (9). If items were removed from the analysis due to low internal consistency, this cut-off point was proportionally re-scaled.
Cross-cultural validation
In the first round, 129 comments were made by the expert panel, mainly regarding formulation and interpretability of the items. The panel made 51 suggestions to improve formulation of the items. After the second round the number of comments decreased to 57, and 25 suggestions were made to improve the items. After the third round there were no further comments and suggestions. After consensus was reached, the final version of the TSK-NL Heart was developed.
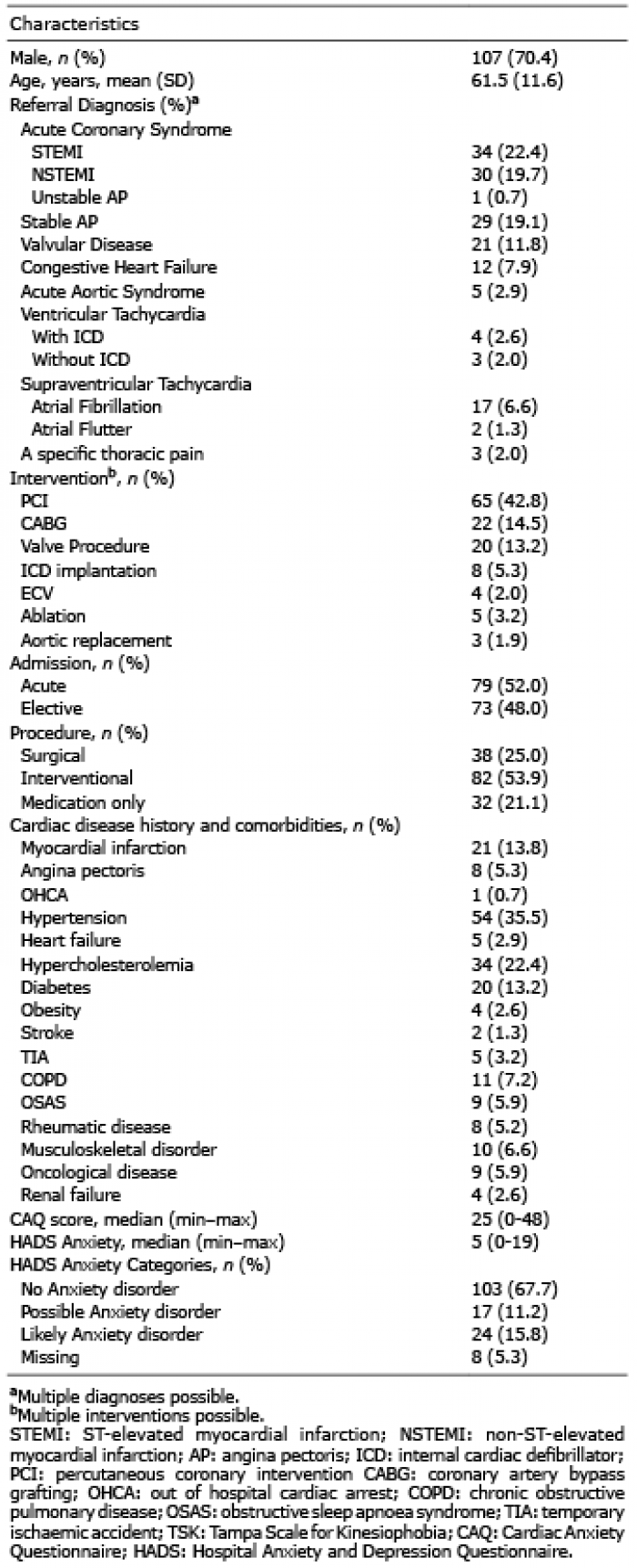
Table I. Population characteristics
Internal consistency
Cronbach’s α for the whole scale was 0.84. The corrected inter-item correlation of items 4, 8, 12, and 16 were below < 0.25 and were removed from the analysis. After removal of these items with low inter-item correlation, Cronbach’s alpha increased to 0.88. All values are shown in Table II.
Table II. Internal consistency and test-retest reliability
Test-retest reliability
Excellent reliability was found for the sum score of the TSK-NL Heart: ICC: 0.82 (95% CI 0.75–0.86). After removal of items 4, 8, 12 and 16, the ICC sum score was: 0.80 (95% CI 0.72–0.85), which is classified as substantial. All ICC values are shown in Table II.
Construct validity
Relationship between TSK-NL Heart and external measures. Since the data were not normally distributed, Spearman’s correlation coefficient (rs) was used. A strong positive correlation was found between TSK-NL Heart sum score (13-items) and the CAQ: rs = 0.61 (95% CI 0.51–0.71). A strong positive correlation was found between the TSK-NL Heart (13-items) and HADS-A: rs = 0.60 (95% CI: 0.48–0.70).
Exploratory factor analysis
After the removal of 4 items (4, 8, 12 and 16) an analysis was performed on the 13 remaining items. The KMO was 0.89, indicating good sample adequacy. Bartlett’s test of sphericity was significant (approximate χ2: 762.845, p = 0.0001), thereby rejecting the hypothesis that our matrix is an identity matrix and thus suitable for PCA. Three components were identified using Kaiser’s criterion (eigenvalue > 1). The explained variance of the 3 components together was 59.5%. Table III shows 3 components after rotation. After assessment 3 factors were defined: “Fear of injury”, “Avoidance of physical activity” and “Perception of risk”.
Table III. Pattern matrix
Prevalence of kinesiophobia
The distribution of kinesiophobia scores across the sample are determined by the 13-item TSK-NL Heart. The new cut-off score of the TSK-NL Heart with 13 items was calculated as 37 * = 28. Patients who score > 28 points are considered to have kinesiophobia. The median score of the total sample was 27.0 points. In this sample, 45.4% of patients scored above the cut-off score. Highest kinesiophobic scores were found in patients treated with medication only, 59.4% scored above the cut-off value vs 45.1% in patients treated with an interventional procedure and 34.2% of patients treated surgically. In acute patients, 46.8% scored above the cut-off value vs 43.8% in elective patients. All scores are shown in Fig. 1.
This study shows that the TSK-NL Heart is a reliable and valid tool to measure kinesiophobia in patients referred to CR with a variety of cardiovascular diseases. In addition, this study showed that kinesiophobia is present in a substantial proportion of participants referred for CR, especially in those treated with medication only and with interventional procedures.
After removal of ambiguous items (4, 8, 12 and 16) the internal consistency of the questionnaire improved. We therefore suggest using the 13-item version of the TSK-NL Heart to measure kinesiophobia in CR participants. Similar results have been reported by other studies (8, 17). The high test-retest reliability reported in this study shows that the TSK-NL Heart is a reliable instrument and indicates that kinesiophobia was stable over the chosen time period of one week. Although the individual items showed only “fair” to “moderate” test-retest reliability, the sum score of the TSK-NL Heart in this study is substantial. This indicates that the TSK-NL Heart is a reliable instrument and gives an indication that kinesiophobia was stable over the chosen time period of one week. Nevertheless, scores on individual items should be interpreted with caution. Similar results, with regard to internal consistency and test-retest reliability, have been reported in previous studies with a similar population (7, 8).
A strong negative correlation was found between the TSK-NL Heart and the HADS-A. A more detailed look at our data revealed that a substantial proportion of patients (62%) had high levels of general anxiety (HADS-A >11) without being fearful of movement, while general anxiety and kinesiophobia co-existed in only in a small proportion (38%). This explains the negative correlation between the HADS-A and the TSK-NL Heart. Theoretically it is unsurprising that almost all patients with kinesiophobia also have high levels of general anxiety, since anxiety is the primary factor in kinesiophobia (18). The HADS-A is commonly used in to assess the level of anxiety in patients in CR (19), but it appears unsuitable to determine the level of specific anxiety symptoms (19), such as kinesiophobia. Based on the current results, we conclude that the HADS-A and TSK-NL Heart measure different constructs (anxiety vs kinesiophobia) and recommend including the TSK-NL Heart in the psychological evaluation of patients referred to CR.
As opposed to the HADS-A, the correlation between the TSK-NL Heart and the CAQ was classified as strong and improved after removal of the ambiguous items. This high correlation was expected, since the factor structure of the external measurement tool (CAQ) was similar to the TSK-NL Heart. The CAQ measures behaviour and anxiety-related symptoms (10), where the TSK-NL Heart’s primary focus is measuring patient beliefs about their physical state. Secondly, the TSK-NL Heart measures “fear of injury”, which is an important aspect of fear avoidance behaviour in patients with cardiovascular disease (20). It is worth investigating the added value of the TSK-NL Heart in a study in which actual movement behaviour is measured, together with both TSK-NL Heart and CAQ, to determine whether the TSK-NL Heart is more specific than the CAQ.
Bäck et al. (7) reported, after performing a confirmatory factor analysis, that the original framework of the TSK with 17 items according to the framework of Kori et al. was the best fit for their data. Since the current study investigated a different patient population and adapted the questionnaire, we performed a new factor analysis. After removal of 4 items, our PCA revealed 3 components that explain the construct of kinesiophobia. Similar levels of explained variance were found by Acar et al. (8) who proposed an 11- item model with 4 components. Differences in factor structure might be explained by differences in study population. Bäck et al. included only those patients with CAD, and Acar et al. studied patients with heart failure and pulmonary hypertension. Our study population consisted of a more heterogeneous group of cardiac patients, since we wanted to generalize the findings to a broad group of CR patients.
High kinesiophobic scores (> 28) were found in patients referred to CR. In particular, high kinesiophobic scores were found in patients treated with medication only (59.4% scored above 28) and after an interventional procedure (45.1%) compared with those who received surgical treatment (34.2%). An explanation for these high kinesiophobic scores might be that patients are discharged shortly after their intervention and thus receive less information or guidance from a physiotherapist or registered nurse, which, in turn, might lead to psychological distress (21). Patients treated with medication alone did not receive an intervention that “repaired” their heart, and might feel less confident about their body and the risk of a secondary cardiac event. Patients who were treated surgically had a longer hospital stay, which might have led to lower levels of kinesiophobia, since these patients received more support from a healthcare professional than those treated with an interventional procedure. This study also shows that the difference between acute and elective admissions, in terms of kinesiophobic scores, was small, indicating that patients treated electively should also be assessed for kinesiophobia.
The high scores for kinesiophobia seen in this study emphasize the need for more attention for kinesiophobia during CR. The outcomes suggest that the TSK-NL is a reliable tool to measure kinesiophobia. We recommend the use of this questionnaire in future studies, to further investigate the presence of kinesiophobia in CR and to evaluate intervention effects, since reducing kinesiophobia is an important objective of CR (22). Furthermore, early screening for kinesiophobia might result in better CR outcomes in patients with kinesiophobia. The TSK-NL Heart could be used for screening patients in whom there is an indication of possible kinesiophobia.
Future research is needed into other psychometric properties of the TSK-NL Heart, such as responsiveness to change, in order to investigate whether this tool is suitable to evaluate outcomes of CR interventions targeting kinesiophobia.
Study limitations
This study has several limitations. Firstly, we chose to include patients who were already referred to CR. Research shows that only 39% of the eligible patients participate in CR (23). Kinesiophobia could result in unwillingness to participate in CR (24). This might have led to selection bias and resulted in a sample with relatively low kinesiophobic scores.
Secondly, in line with previous studies (7), the current study used a cut-off score of >28 to define “high kinesiophobic scores”, since, unfortunately, there is no gold standard for kinesiophobia. Nevertheless, a large variety of scores was found in our sample with a substantial number of scores above the cut-off point. Even when a more conservative cut-off point is used, high kinesiophobic traits are present in a substantial proportion of patients. We therefore consider it likely that high kinesiophobic scores exist in CR patients.
In a recent study, with a different population, in which a 13-item TSK-pain was used, the clinically meaningful severity levels of the TSK-pain were assessed in a sample of patients with musculoskeletal pain and divided as follows: subclinical: 13–22; mild: 23–32; moderate: 33–42; and severe: 43–52 (29). It is not known whether these cut-off scores can be generalized to our population. However, it might be useful to define several categories, since the presence of kinesiophobia is not dichotomous and might be of better use for the clinician (30). More research is needed, in studies with bigger sample sizes, to define clinically meaningful severity scores for the TSK-NL Heart.
Thirdly, the current study shows a 3-factor model to be the most suitable for the TSK-NL Heart. This version of the TSK-NL Heart excludes 4 questions due to low inter-item correlations. It should be investigated whether rephrasing these items is necessary to gain better construct validity, instead of removal. Lastly, the current study assessed the prevalence of kinesiophobia. There were high levels of kinesiophobia in this relatively small sample. These findings should be validated in future studies with larger sample sizes.
Conclusion
This study shows that the TSK-NL heart has good psychometric properties. We recommend using the 13-item TSK-NL Heart to measure kinesiophobia in CR patients.
This study indicates that high kinesiophobia scores are present, and also in a substantial proportion of patients referred to CR, emphasizing the need for more attention for kinesiophobia during these rehabilitation programmes.
Fig. 1. Distribution of kinesiophobia presented as amplitude probability distribution functions.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize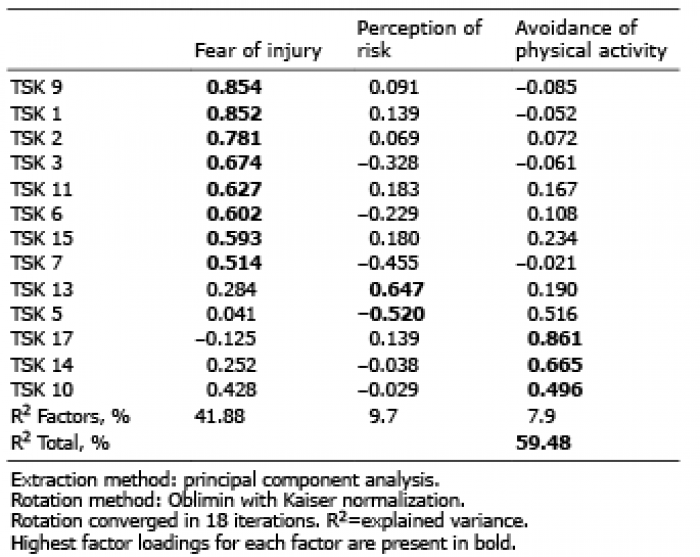 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize