
From the 1Studio di Economia Sanitaria, Milan, 2Physical and Rehabilitation Medicine, Department of Health Sciences, Università del Piemonte Orientale, Novara, 3Neuromotor and Cognitive Rehabilitation Research Center, Department of Neurosciences, Biomedicine and Movement Sciences, University of Verona, Verona, 4Ipsen S.p.A, Medical Advisor, Assago, 5Ipsen S.p.A, Market Access, Assago, Italy and 6Spasticity and Movement disorders “ReSTaRt” Unit, Physical Medicine and Rehabilitation Section, “Riuniti Hospital”, University of Foggia, Foggia, Italy
*A provisional version of this research has been given as an oral presentation at the TOXINS 2019 conference, Copenhagen, Denmark, 17 January 2019 (speaker: Alessio Baricich, MD, PhD).
Objective: To investigate costs and quality-adjusted life years of rehabilitation combined with abobotulinumtoxinA (aboBoNT-A) (rehab/aboBoNT-A) vs rehabilitation alone (rehab) in post-stroke spasticity in Italy.
Design: Based on both Italian National Health Service and societal perspectives, a 2-year cost-utility analysis model was performed.
Subject/patients: The cost-utility analysis model considered hypothetical patients.
Methods: The cost-utility analysis model was populated with data concerning demographics, disease severity, healthcare and non-healthcare resource consumption. Data were collected via a questionnaire administered to 3 highly experienced Italian physiatrists (864 out of 930 post-stroke spasticity patients on rehab/aboBoNT-A in total). Costs are expressed in Euro (€) based on the year 2018.
Results: The cost to society (rounded to the nearest whole €) was €22,959 (rehab/aboBoNT-A) vs €11,866 (rehab). Italian National Health Service-funded cost was €7,593 (rehab/aboBoNT-A) vs €1,793 (rehab). Over a period of 2 years rehab/aboBoNT-A outperforms rehab in terms of quality-adjusted life years gained (1.620 vs 1.150). The incremental cost-utility ratio was €12,341 (Italian National Health Service viewpoint) and €23,601 (societal viewpoint). Sensitivity analyses confirmed the robustness of the baseline results.
Conclusion: Despite some limitations, the higher number of quality-adjusted life years gained vs rehab and the high probability of reaching a cost-utility ratio lower than the Italian informal acceptability range (€25,000–40,000) make rehab/aboBoNT-A a cost-effective healthcare programme for treating patients with post-stroke spasticity in Italy.
Key words: stroke; spasticity; abobotulinumtoxinA; rehabilitation; cost-utility analysis; Italy.
Accepted Nov 28, 2019; Epub ahead of print Dec 10, 2019
J Rehabil Med 2020; 52: jrm00016
Correspondence address: Carlo Lazzaro, Studio di Economia Sanitaria, Via Stefanardo da Vimercate, 19, Milan I -20128, Italy. E-mail address: carlo.lazzaro@tiscalinet.it
Using a tool named cost-utility analysis, this study investigated whether rehabilitation combined with a given drug (abobotulinumtoxinA) for post-stroke spasticity is cost-effective (i.e. affordable) vs rehabilitation alone for both the Italian National Health Service and society. Over a period of 2 years, this study shows that each additional year weighted for health-related quality of life (quality-adjusted life year; QALY) gained via rehabilitation combined with abobotulinumtoxinA vs rehabilitation alone for post-stroke spasticity costs the Italian National Health Service and society €12,341 and €23,601, respectively (2018 values). Given the Italian informal acceptability range (i.e. the maximum amount decision-makers are supposed to pay) for additional QALY gained (€25,000–40,000), these results support the conclusion that rehabilitation combined with abobotulinumtoxinA is a cost-effective (i.e. good value for money) healthcare programme for treating patients with post-stroke spasticity in Italy.
Post-stroke spasticity (PSS) is described as velocity-dependent increased muscle tone with exaggerated tendon jerks subsequent to stroke, resulting from hyperexcitability of the stretch reflex. Its prevalence ranges from 4% to 27% in the early post-stroke phase (1–4 weeks post-stroke), 19% to 26.7% in the post-acute phase (1–3 months post-stroke), and 17% to 42.6% in the chronic phase (>3 months post-stroke) (1).
Spasticity can vary from a mild neurological sign to a significant increase in muscle tone that might affect joint mobility. Notably, PSS can be associated with a negative impact on activities of daily living (ADL) (1).
Botulinum toxin type A (BoNT-A) is an effective treatment for focal spasticity in stroke survivors, and is approved by the US Food and Drug Administration and European regulatory agencies for this indication. BoNT-A is an enzyme that acts in the cytosol of nerve endings to cleave synaptosomal-associated protein (SNAP)-25, resulting in blocked acetylcholine release at neuromuscular junctions (2). Intramuscular injections of BoNT-A are currently considered the gold standard for treatment of PSS, due to its effectiveness in reducing spastic hypertonia with low prevalence of complications. In addition, BoNT-A might reduce disability in patients affected by PSS, improving patients’ participation in ADLs and health-related quality of life (HRQoL) (3).
AbobotulinumtoxinA injection (aboBoNT-A; Dysport®, Ipsen Pharma SAS, Paris) has been shown to be a safe and effective treatment for PSS (4), which improves rehabilitation outcomes (5, 6) and relieves pain (7).
In order to investigate the costs and QALYs of rehabilitation + BoNT-A (rehab/aboBoNT-A) vs rehabilitation (rehab) in Italy, a 2-year, model-based cost-utility analysis (CUA) was performed (8, 9).
Decision tree
All authors participated in a meeting aimed at exploring the feasibility of this research project. Hence, it was not possible to apply the approach used in other studies on the cost-effectiveness of BoNT-A (10, 11), the Delphi panel (12), since the methodological requirement of anonymity of the panellists was breached (12). Thus, as suggested in the literature for this situation (12), the qualified opinion of a sample of convenience (13) of 3 highly experienced Italian physiatrists (comprising 930 post-stroke patients with upper or lower limb spasticity treated in total; 864 on rehab/aboBoNT-A and 66 on rehab only) who co-authored this research (AB: 170 on rehab/aboBoNT-A and 30 on rehab only; AP: 456 on rehab/aboBoNT-A and 24 on rehab only; AS: 238 on rehab/aboBoNT-A and 12 on rehab only) was elicited to estimate, via an ad hoc questionnaire, most of the parameters that were used for populating the CUA model (see Supplementary Tables SM1–SM241).
To obtain the mean value for each parameter, these estimates were weighted for the proportion of 930 post-stroke patients with upper or lower limb spasticity on rehab/aboBoNT-A or rehab that were followed by each physiatrist. Physiatrists stratified patients using the Ashworth scale according to their PSS severity (14).
Costs, life-years saved (LYS) and QALYs of hypothetical patients on rehab/aboBoNT-A and rehab were calculated via a decision tree (15) developed using Microsoft Excel® 2010 (Microsoft, Redmond, WA, USA).
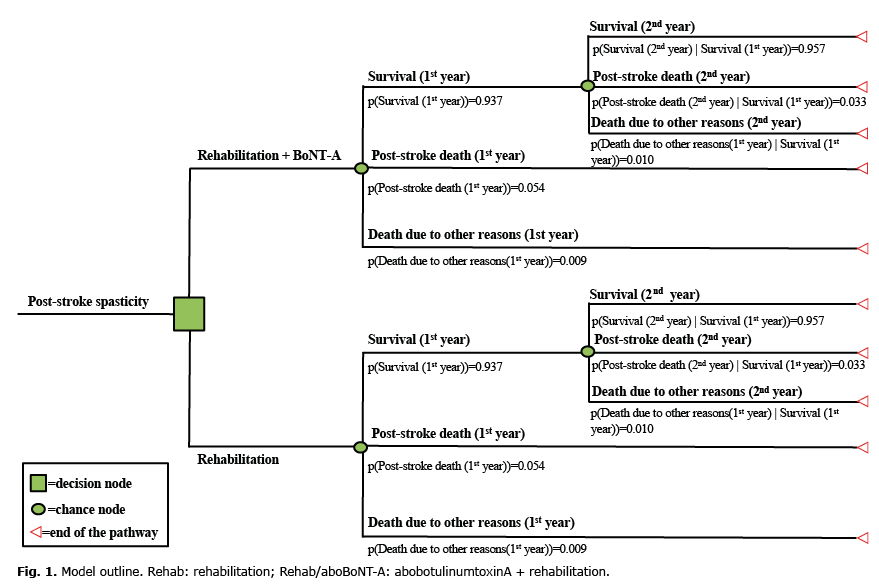
Consistent with the time horizon covered by a previous study of HRQoL in patients with PSS (16), the decision tree covers a 2-year period, during which patients can move from post-stroke survival (i.e. the starting health state when patients enter the model) to stroke-related death or death due to other causes (17, 18). Transitions between these 3 health states are probabilistic (15, 19) (Fig. 1).
Fig. 1. Model outline. Rehab: rehabilitation; Rehab/aboBoNT-A: abobotulinumtoxinA + rehabilitation.
Utility and QALYs
QALYs synthesize improvements in both length of life and desirability of health state with time (8, 9). Calculation of QALYs implies multiplying LYS accrued to patients by a synonym for HRQoL experienced by patients, named utility (8, 9). Utility ranges between 0 (death or other health state perceived worse than death) and 1 (perfect health) (8, 9).
For the 2 years considered in the CUA model, PSS utility for rehabilitation patients was obtained from the literature (first year: 0.60; second year: 0.64) (16) (Table SM231): hence, the first and second years lived with PSS by patients in rehabilitation correspond to 0.60 and 0.64 years lived in full health.
For rehab/aboBoNT-A patients, a percentage improvement (range 0–100%) in utility vs rehab patients was elicited from physiatrists and used to express rehab/aboBoNT-A patients’ utility as a multiple of rehab patients’ utility (Table SM241). Physiatrists’ perception was based on improved mobility and ADL experienced by their patients on rehab/aboBoNT-A vs those on rehab.
As a half-cycle correction was applied (15), 6-month costs, LYS and QALYs were calculated for patients who had died from stroke sequelae or other causes (Tables SM81 and SM101), as these patients were assumed to die halfway through each 1-year period.
Resource identification, quantification and valuation
As the economic evaluation adopted both the Italian National Health Service (INHS) and the societal perspective (8), consumption of healthcare and non-healthcare resources was valued.
Healthcare resources funded by INHS included: aboBoNT-A and intramuscular administration (in outpatient or day-hospital setting); rehabilitation sessions (in outpatient, day-hospital or home setting); ultrasounds and physiatrist follow-up visits; mobility aids (crutches; orthosis; shoulder braces; walking aids; wheelchairs); baclofen (per os or intrathecal); pregabalin per os; physiatrist and neurologist visits, drugs, electromyography and rehabilitation sessions due to rare aboBoNT-A-related adverse events (AEs), such as botulinic syndrome and chronic urticaria (Tables SM1–SM91; and SM11–SM151).
Healthcare services provided in outpatient, day-hospital or inward hospital settings were costed according to outpatient or hospital tariffs, assumed as a reasonable proxy of the real costs borne by healthcare facilities (20) (Tables SM19–SM211). As it was administered in the hospital setting only, aboBoNT-A was costed at its ex-factory price (which is approximately 33% less than the consumer price (CP)). The other drugs were costed at their CP (Table SM21). Assuming a 5-year useful life for those healthcare goods that support patients beyond the year of purchase (e.g. walking aids), a 5-year straight-line depreciation approach (8) was adopted for calculating their yearly cost (Tables SM20 and SM211).
The mean cost for each AE was determined by multiplying the cost of its management by its incidence (1/5,000 patients, as reported by 1 of the physiatrists in his clinical practice) (Tables SM21 and SM81). Costs to patients and their families consist of out-of-pocket expenses, patient loss of working days and informal care (8). Out-of-pocket expenses include healthcare resources that are not funded by the INHS (shockwave sessions; additional private home rehabilitation sessions; antihistamine/corticosteroid for skin rash management; some type of orthosis and walking canes), as well as all non-healthcare resources (car transport to and from home/healthcare facility; parking at healthcare facility; home help , that is a person whose job is to help ill people at their homes with activities such as cooking and cleaning.) (Tables SM11 and SM2; S6; SM14–SM16; Tables SM221).
Consistent with the gross wage rate approach (21), the daily cost of a home help includes net wage, social security contribution and taxation, as specified by the national labour agreement) (Tables SM161 and SM221). The gross wage rate approach was also applied to value the working days lost by the patient while undergoing healthcare services and by caregivers in providing informal care (Tables SM171 and SM18; SM221). If the patient was unemployed, not engaged in housekeeping or retired (≥ 70 years old), working time was replaced by leisure time, which was costed according to the take-home wage rate (net wage only) (21) (Table SM221). Carers were assumed to be employed or housewives. The daily cost of a patient’s carer was considered a good proxy for costing housewife’s time (20) (Table SM221).
Costs were expressed in Euro (€) based on the year 2018 per patient and updated to that year according to inflation rates for healthcare services or for general consumption whenever necessary (22). A 3% annual real social discount rate was applied to costs, LYS, and QALYs (8, 9, 23) (Table SM21).
As the CUA model is not a clinical trial, no ethics committee approval of the study protocol (including the above-mentioned questionnaire) was required by current Italian legislation (24).
Cost-utility analysis
The difference in costs and QALYs of alternative healthcare programmes (incremental approach) compared via CUA is calculated and summarized via the incremental cost-utility ratio (ICUR), which is the ratio of incremental costs (ΔC) to incremental QALYs (ΔQALYs) (8, 9).
In general, the ICUR provides decision-makers with the cost of obtaining an incremental QALY with the healthcare programme that has a better effect on patient’s HRQoL, but is also more costly than the comparator(s).
Statistical analysis
Point estimate and 95% confidence interval (95% CI) were calculated for most of the parameters included in the CUA model and for ICURs (15, 19, 25). Whenever an analytical calculation was not possible, the standard error for parameters was calculated by imposing an appropriate coefficient of variation on their point estimate (15, 19, 25, 26). For parameters that were not given a statistical distribution, a range was reported. No hypothesis test was performed.
Sensitivity analyses
The uncertainty of the base case ICUR was explored by one-way and probabilistic sensitivity analyses (8, 9). Parameters included in one-way sensitivity analysis were varied individually, holding the others at their baseline values (8, 9).
One-way sensitivity analysis examined the variations in ICUR due to changes in all the parameters classified as event probabilities; resource consumption; unit cost; utility for PSS patients on rehab; utility multiplier for PSS patients on rehab/aboBoNT-A; post-stroke standardized mortality ratio (SMR). In addition, the 3% baseline real social discount rate was changed (0%; 5%) to test its influence on ICUR over the 2-year period covered by the CUA model (8, 9).
Apart from real social discount rate, parameters included in one-way sensitivity analysis were varied by replacing their baseline point estimate with the lower and upper limits of the 95% CI resulting from appropriate statistical distributions, which were fitted to each type of parameter or their range (15, 19, 26). Beta distribution was fitted to binomial data (e.g. a parameter that encompasses 2 categories, such as being employed or not) and utility values for rehab patients. A Dirichlet distribution was given to multinomial data (e.g. a parameter that encompasses ≥ 3 categories, such as attending to INHS-funded rehabilitation sessions in outpatient, day-hospital or home setting). Post-stroke SMR was given a log-normal distribution, whereas unit costs as well as utility multiplier for patients on rehab/aboBoNT-A were assumed to be normally distributed A gamma distribution was used to represent uncertainty in resource consumption. The results of one-way sensitivity analysis are displayed as departures from the baseline ICUR on a Tornado chart. The relationship between ICUR and time was investigated by reducing the CUA model time-span from 2 years to 1 year.
Probabilistic sensitivity analysis assessed the joint parameter uncertainty affecting the base case ICUR via a 10,000-iteration Monte Carlo simulation (8, 9, 15, 19) and supported the calculation of the 95% CI of ICURs (percentile method) (26, 27). For each Monte Carlo iteration, a random value was drawn from the statistical distribution fitted to each parameter included in probabilistic sensitivity analysis (15, 19). An algebraic manipulation of the ICER (net monetary benefit) supported the construction of the cost-effectiveness acceptability curve, which was applied to Monte Carlo simulation results to graphically represent the uncertainty concerning the cost-effectiveness of rehab/aboBoNT-A and rehab (15, 19, 28). Drug posology and costs were not included in sensitivity analyses (19).
Decision tree
Notional patients enter the CUA model aged 66 (range 40–79) years; the probability of being female is 0.475 (Table I). The expected survival probability after the first year is the same for both rehab/aboBoNT-A and rehab patients (0.937), as is the conditional probability of being alive in the second year having survived the first year (0.957) (Fig. 1). The probability of death unrelated to stroke increases by 0.01 from the first to the second year.
Most patients (0.928) are prescribed rehab/aboBoNT-A (Table I). Patients on rehab/aboBoNT-A are more likely to be severe than those on rehab (mild PSS: 0.148 vs 0.624; moderate PSS: 0.332 vs 0.355; severe PSS: 0.287 vs 0.011; very severe PSS: 0.233 vs 0.011) (Table I). AboBoNT-A is more likely to be administered in day-hospital (0.925) than in outpatient setting (0.075) and its posology, which is consistent with PSS severity, ranges from 500 potency unit (U) for mild impairment to 1,500–2,000 U for very severe impairment (Table I).
Patients with severe or very severe PSS on rehab/aboBoNT-A or on rehab have different probability of being active workers (0.052 vs 0.00). The probability of being employed with no reduction in working hours due to PSS is 0.700 for both rehab/aboBoNT-A and rehab (Table I). The average number of working days lost due to PSS treatment is 33.97 (range 6.76–70.27) for patients on rehab/aboBoNT-A and 9.74 (range 1.56–39.89) for those on rehab (Table I).
Among female patients, the probability of being a housewife ranges from 0.417 for rehab/aboBoNT-A to 0.439 for rehab (Table I).
Table I. Main quantitative non-monetary results from the cost-utility analysis (CUA) model
The probability of needing home help depends on being on rehab/aboBoNT-A (0.411) or rehab (0.384) (Table I).
The probability of needing informal care varies according to the severity of PSS and also differs between rehab/aboBoNT-A and rehab (mild PSS: 0.327 vs 0.246; moderate PSS: 0.538 vs 0.349; severe PSS: 0.796 vs 0.608; very severe PSS: 0.796 vs 0.608) (Table I).
On average, patients on rehab/aboBoNT-A receive 10.63 days of informal care (range 1.77–11.50), whereas for patients on rehab caregivers are engaged 1.72 days (range 0.31–2.60) (Table I).
Cost, QALYs and cost-utility analysis
The cost borne by society for rehab/aboBoNT-A and rehab is €22,959 and €11,866, respectively (Table II).
INHS-funded cost for rehab/aboBoNT-A and rehab are €7,593 and €1,793 (33.07% vs 15.11% of the overall cost); out-of-pocket expenses are €11,402 and €8,820 (49.66% vs 74.33% of the overall cost), whereas productivity losses and informal care amount to €3,964 and €1,254 (17.26% vs 10.56% of the overall cost).
For both healthcare programmes the cost-driver is home help (35.85% and 64.83% of the overall cost for rehab/aboBoNT-A and rehab, respectively).
It is noteworthy that the largest share of overall cost (rehab/aboBoNT-A: 49.66%; rehab: 74.33%) is funded out-of-pocket by the patient and their families. These amounts also include healthcare resources that are not funded by INHS (e.g. additional home rehabilitation sessions).
Despite no difference in mortality (LYS 1.858 per patient for both rehab/aboBoNT-A and rehab), during the 2-year period rehab/aboBoNT-A outperforms rehab in terms of QALYs gained (1.620 vs 1.150 per patient), since the mean value of the utility multiplier for patients on rehab/aboBoNT-A as elicited from the 3 physiatrists who co-authored this research is 1.409 (i.e. for each year covered by the CUA model the utility for PSS patients on rehab/aboBoNT-A was considered +40.86% than the utility experienced by PSS patients on rehab).
Following the INHS and societal viewpoints, due to incremental cost of €5,801 and €11,093 coupled with incremental QALYs (0.470 for both perspectives), the ICUR, that is the cost for obtaining an incremental QALY with rehab/aboBoNT-A vs rehab, reaches €12,341 (95% CI: €6,206; €42,242) and €23,601 (95% CI: €8,408; €84,485) (Table III).
Table II. Base case analysis: costs per patient (2018)
Table III. Base case analysis: cost-utility analysis (2018)
Sensitivity analyses
The Tornado chart shows that, from the perspective of both INHS and society, the largest variations in the baseline ICURs are caused by changes in the utility multiplier for post-stroke patients on rehab/aboBoNT-A (from –40.32% to +208.33% vs base case ICUR) (Fig. 2A and B).
Replacing the base case number of INHS-funded rehabilitation sessions prescribed to rehab/aboBoNT-A patients with moderate PSS per year causes the base case ICURs estimate to vary between –12.67% and +18.76% (INHS perspective) and –17.25% and +25.53% (societal perspective).
Varying the age the patient enters the CUA model has a remarkably skewed effect for societal perspective only (from –0.08% to +92.10% vs base case ICUR) (Fig. 2B).
Fig. 2. (A) One-way sensitivity analysis: Italian National Health Service (INHS) viewpoint (2018). Base case incremental cost-utility ratio (ICUR) Rehab/aboBoNT-A= €12,341. ICUR: incremental cost-utility ratio; INHS: Italian National Health Service; LL 95% CI: lower limit 95% confidence interval; UL 95% CI: upper limit 95% confidence interval; Rehab: rehabilitation; Rehab/aboBoNT-A: abobotulinumtoxinA + rehabilitation. (B) One-way sensitivity analysis – Societal viewpoint (2018). Base case ICUR Rehab/aboBoNT-A=€23,601; LL 95% CI: lower limit 95% confidence interval; UL 95% CI: upper limit 95% confidence interval; Rehab: rehabilitation; Rehab/aboBoNT-A: abobotulinumtoxinA + rehabilitation.
Due to the limited time horizon covered by the CUA model, the difference in ICURs between the first and second years is negligible: +3.19% following the INHS perspective (€12,735 vs €12,341) and +3.22% adopting the societal viewpoint (€24,360 vs €23,601).
The cost-effectiveness acceptability curve shows higher probability for rehab/aboBoNT-A to be cost-effective as the threshold value for incremental QALY gained increases. When the INHS (societal) viewpoint is considered, the likelihood that rehab/aboBoNT-A is cost-effective is 91.61% (54.32%) for a threshold value of €25,000 and 97.30% (84.70%) for a threshold value of €40,000 (Fig. 3A and B).
Fig. 3. (A) Cost-effectiveness acceptability curve: Italian National Health Service (INHS) viewpoint (2018). Base case incremental cost-utility ratio (ICUR) Rehab/aboBoNT-A=€12,341. Rehab: rehabilitation; Rehab/aboBoNT-A: abobotulinumtoxinA + rehabilitation. (B) Cost-effectiveness acceptability curve: society viewpoint (2018). Base case ICUR Rehab/aboBoNT-A=€23,601. Rehab: rehabilitation; Rehab/aboBoNT-A: abobotulinumtoxinA + rehabilitation.
This is the first Italian economic evaluation aimed at comparing costs and QALYs gained with rehab/aboBoNT-A and rehab via a CUA model, populated with data mainly provided by a sample of convenience (13) of 3 physiatrists highly experienced in dealing with patients with PSS on rehab/aboBoNT-A.
As far as the Italian setting is concerned, previous notable research focused on costs only (29, 30), with no attempt to provide cost-effectiveness or cost-utility estimates for rehab/aboBoNT-A.
Regardless of the viewpoint adopted, base case and sensitivity analyses show that, compared with rehab, rehab/aboBoNT-A is more costly, but gains more QALYs.
It seems noteworthy that post-stroke patients on rehab/aboBoNT-A totalled higher costs than those on rehab because of the greater number of rehabilitation sessions (most of them funded by the INHS in day-hospital, outpatient or home setting), which, in turn, increases the economic burden placed on patients and their families (8) due to transportation and parking at the healthcare facility, as well as the time devoted by the patient and caregiver to healthcare service provision.
From both the INHS and societal viewpoints, the base case ICURs for rehab/aboBoNT-A fall below the lower limit of the informal acceptability range per QALY gained proposed for Italy (€25,000) (23).
The cost-effectiveness acceptability curve supports the high probability for rehab/aboBoNT-A to be cost-effective compared with the upper limit of the informal acceptability range mentioned above (€40,000) (23).
A simple budget impact analysis (31) highlights that prescribing rehab/aboBoNT-A to all the 930 patients followed by the 3 physiatrists who co-authored this research would cost the INHS €5.39 million more than rehab alone (i.e. the incremental costs of €5,801 for aboBoNT-A/rehab vs rehab over 2 years multiplied by 930 patients). This amount represents a very small proportion (1.17%) of the total gross expenditure for musculoskeletal drugs funded by INHS in 2017 (€460 million) (32).
Interestingly, the current findings appear to go against the prevailing trend. According to the results of previous economic evaluations performed in Europe, the cost-effectiveness of BoNT-A in PSS remains controversial and the need for further research is apparent, especially as far as QALYs are concerned.
A decision-tree supported cost-effectiveness analysis carried out in the UK (11), which used the the cost-per-successfully-treated month as its outcome, advised on the affordability for the UK National Health Service (NHS) of the cost per incremental unit of effectiveness with oral BoNT-A (onabotulinumtoxin A), which ranged from UK £942 to UK £1,697 (2002 values). It is noteworthy that no threshold value was considered to support that recommendation.
An empirical, 3-month CUA in the UK compared rehab/aboBoNT-A with rehab in upper limb PSS (33). The baseline ICUR (UK £93,500 per QALY gained; 2007 values) and the low probability (0.36) for rehab/aboBoNT-A to be cost-effective vs the England and Wales threshold value of UK £20,000 per QALY gained (34) led the investigators to conclude that aboBoNT-A was not cost-effective for the UK NHS in this indication (33).
Limitations
This study has some limitations. Firstly, a model-supported CUA was performed instead of an empirical CUA aimed at comparing rehab/aboBoNT-A vs rehab in PSS. Although in this research field the decision model approach for cost-effectiveness analysis (35) has been questioned (33), an empirical CUA seems to cover too short a time-span (33) to gather ultimate results about the cost-effectiveness of rehab/aboBoNT-A in this indication. However, being aware of the pros and cons of health economic models (8, 9, 15, 35, 36), the robustness of our baseline findings was tested via 2 comprehensive sensitivity analyses, which confirmed the baseline findings.
A second limitation of this study was the decision to consider a single type of BoNT-A in the CUA model. However, this choice was justified by the fact that the Italian Medicines Agency acknowledged aboBoNT-A to be the lowest ex-factory price per U vs other botulinum toxins type A reimbursed by the INHS for PSS (37). Moreover, our analysis is highly conservative for rehab/aboBoNT-A; in practice, it is likely that hospital tender discount policies would decrease the purchasing price for aboBoNT-A; hence reducing the ICUR for rehab/aboBoNT-A accordingly.
A third limitation concerns utility values used for QALYs calculation. As reported for other diseases (38), utility values exert a remarkable impact on ICUR because of their prominent role in the calculation of QALYs. It therefore follows that, all other things being equal, different QALYs can lead to diverse decisions about the sustainability of rehab/aboBoNT-A when the resulting ICURs are contrasted against the threshold values adopted in different jurisdictions (38). For rehab patients, utility values were collected from a sample of US patients with PSS during a 2-year follow-up (16). While it is known that patients in different countries treated for the same severe disease are likely to return similar HRQoL scores (27), notwithstanding it would be interesting to compare these values with the utility values elicited from a sample of Italian patients with PSS on rehab. Following the approach adopted in previous research (8, 39), the calculation of QALYs for rehab/aboBoNT-A patients relies heavily on physiatrists’ opinion. Being aware of the relevance of this assumption in influencing the denominator of the ICURs for rehab/aboBoNT-A, the uncertainty surrounding utility values and multiplier was carefully investigated in one-way and probabilistic sensitivity analyses. Importantly, replacing the baseline estimate of the utility multiplier for calculating rehab/aboBoNT-A QALYs with the lower limit of the 95% CI (i.e. +13.3% vs utility for rehab patients) in a one-way sensitivity analysis, the resulting ICURs (INHS viewpoint: €38,052; societal viewpoint: €72,769) were lower than both the upper limit of the acceptability range proposed for Italy (€40,000) (23) and the informal threshold value that led the Italian Medicines Agency to reimburse cancer drugs (€87,330) (40).
In conclusion, the results of this study show that, for both the INHS and society, rehab/aboBoNT-A is a cost-effective healthcare programme for treating patients with PSS in Italy.
This study was funded by Ipsen S.p.A, which has had no influence on the interpretation of data and the conclusions drawn.


 Click to show fullsize
Click to show fullsize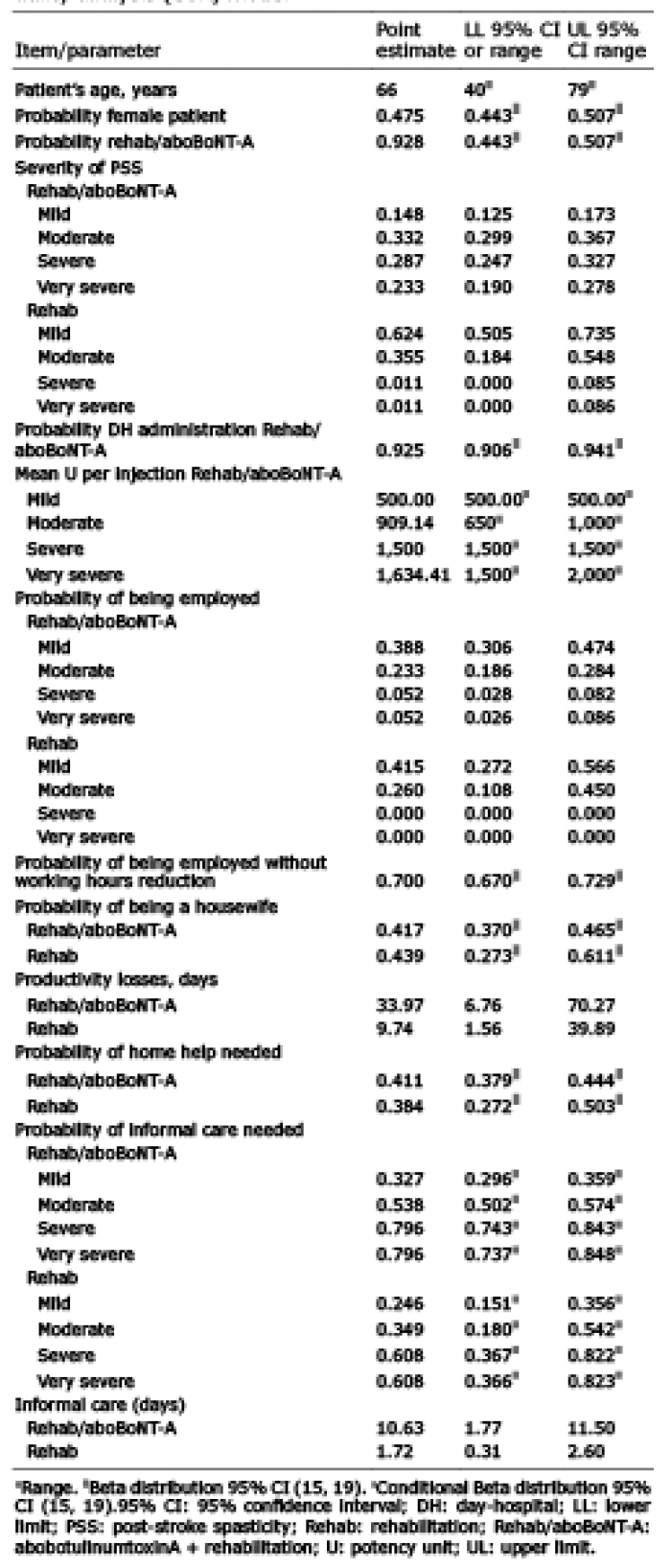 Click to show fullsize
Click to show fullsize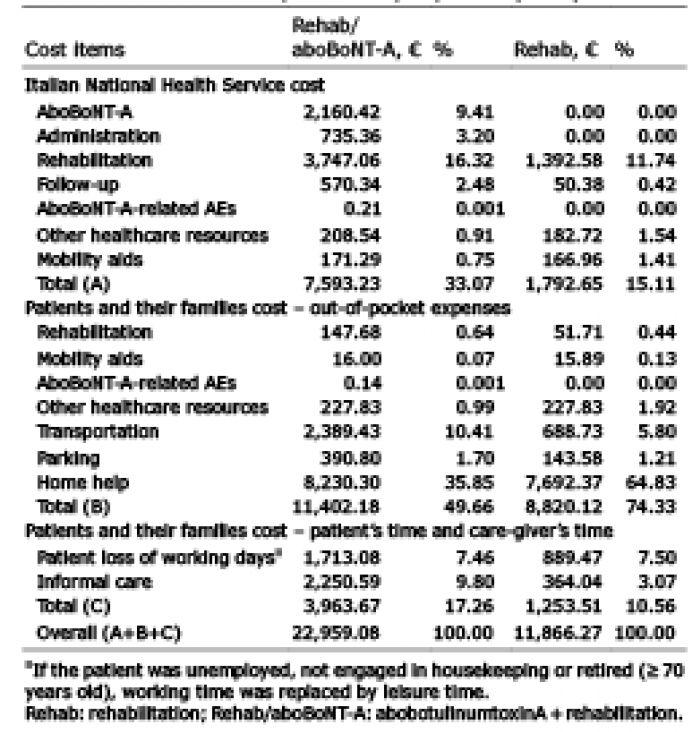 Click to show fullsize
Click to show fullsize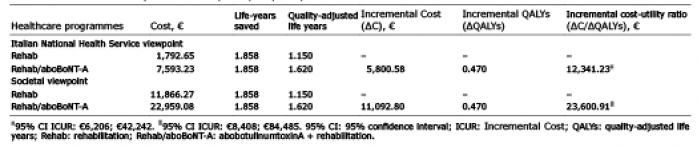 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize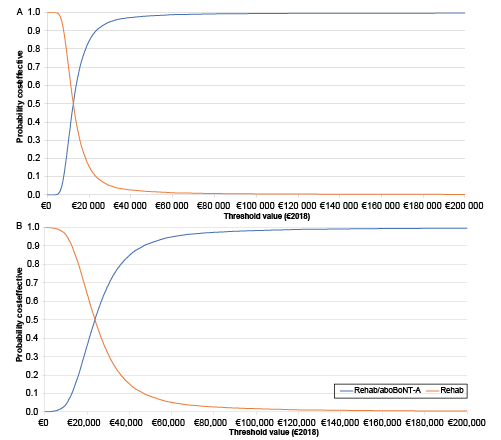 Click to show fullsize
Click to show fullsize