
From the 1Academic Department of Rehabilitation Medicine, School of Medicine, Faculty of Medicine and Health, University of Leeds, 2National Demonstration Centre in Rehabilitation, Leeds Teaching Hospitals NHS Trust, 3Independent International Development, Education and Human Resources Consultant, Leeds, UK, 4Centre d’Appareillage de Madagascar, Befelatanana, 101 Antananarivo, Madagascar and 5NIHR Devices for Dignity MedTech Co-operative, Royal Hallamshire Hospital, Sheffield, UK
Objective: Rehabilitation services play an important role in optimizing functional ability and societal integration for people with disabilities. The Madagascar Rehabilitation Programme (2011–2013) resulted from a global training partnership and led to 8 doctors achieving a university diploma in rehabilitation medicine. This paper describes a 2014 evaluation of the programme methods, results and learning points.
Methods: A combination of qualitative methods was used for the evaluation, based on a Theory of Change model, with informants from Madagascar and the UK.
Results: Malagasy trainees and UK volunteers gained new theoretical knowledge and practical skills. For Madagascar, it led to changes in working practice and the formation of a national rehabilitation association. Key to its success was the strong collaboration between Malagasy and UK professionals, with support from the University and Ministry of Health in Madagascar, and the UK partners. Having a clear common vision ensured the programme met the needs of the Malagasy clinicians.
Conclusion: Rehabilitation is increasingly recognized as an important focus for international development. Successful rehabilitation training programmes can be achieved at modest costs with global health partnerships. The combination of factors that enabled this programme to be a success is reproducible in other contexts.
Key words: global health; rehabilitation; teaching; health services; development; partnership.
Accepted Oct 22, 2019; Epub ahead of print Oct 28, 2019
J Rehabil Med 2020; XX: XX–XX
Correspondence address: Helen N. Locke, Academic Department of Rehabilitation Medicine, D Floor, Martin Wing, Leeds General Infirmary, Leeds LS1 3EX, UK. E-mail: helen.locke1@nhs.net
Rehabilitation services play an important role in helping people with disabilities to participate fully in everyday life. In Madagascar, a training programme in rehabilitation medicine was run jointly by partners in Madagascar and the UK from 2011 to 2013. This led to 8 doctors achieving a university diploma in rehabilitation medicine. This paper describes a 2014 evaluation of the programme. Trainees gained new knowledge and practical skills, leading to significant lasting improvements to rehabilitation services. A national association of rehabilitation professionals was formed. UK volunteers also benefited from the experience, gaining skills relevant to their current professional roles. A clear vision and strong working partnerships between the 2 countries was crucial to this success. Rehabilitation is increasingly recognized as an important focus for international development. Successful rehabilitation training programmes can be achieved at low cost with global health partnerships, as described here. These learning points are applicable to other contexts.
Approximately 15% of the world’s population live with a disability and this number continues to increase (1). Persons with disabilities are over-represented in low- and middle-income countries (LMICs). The United Nations (UN) estimate that two-thirds of people with moderate or severe disabilities live in poverty worldwide (2, 3). The World Health Organization’s (WHO’s) World Report on Disability 2011 and Global Disability Action Plan 2014–2021 highlight disability as a truly global public health priority (1, 4). Rehabilitation services are an important actor in optimizing functional ability and societal integration for people with disabilities. Effective rehabilitation encourages participation in society, reducing care costs and supporting people to return to education and employment, contributing to tax revenue and national development (5). However, a considerable gap remains between the need for rehabilitation and the services available. This is particularly true in LMICs such as Madagascar, where training for rehabilitation physicians and associated health professionals is often limited or non-existent (6). It is estimated that there are fewer than 0.5 rehabilitation professionals per 10,000 citizens in many sub-Saharan countries (7).
Madagascar is the fifth poorest country in the world: an estimated 78% of its population of nearly 27 million live on less than US$1.90 per day (8). Political instability and lack of foreign aid have contributed to an enduring social and economic crisis, with a lack of stable public services, high rates of unemployment, food insecurity and diminishing educational level.
An estimated 2.8% of the population of Madagascar live with a physical impairment, although the actual number may be much higher (9–11). Access to healthcare for people with disability is limited. For most of the population, the distance to a rehabilitation centre is long, and travel is hampered by poor road and transport infrastructure. Services lack modern equipment, and patients frequently struggle to meet the costs of treatment, as few have access to health insurance. Despite this, the rights of persons with disabilities are increasingly recognized in Madagascar. This is exemplified by the ratification of the UN Convention on the Rights of Persons with Disabilities (UNCRPD) in 2014 and the publication of the National Strategic Plan for Physical Rehabilitation (PNSRP) 2017–2021 (12, 13).
Andrianabela et al. (14) described the Madagascar rehabilitation training programme (2011–13), a training partnership facilitated by the University of Leeds and Leeds Teaching Hospitals Trust (LTHT) and funded by Opt In, a UK-based charity (14, 15). This paper describes the methods, results and learning points from a full evaluation and impact assessment carried out in 2014, a year after completion of training (16), and incorporates an overview of activities that resulted from the programme in the 5 years after the evaluation.
Training programme
The training was jointly devised by the Malagasy and UK leads, and had support from the Malagasy Ministry of Health (MoH). A Memorandum of Understanding (MoU) between LTHT, the University of Leeds and the University of Antananarivo ensured a collaborative approach, with both countries having local coordinating groups (14). The training was delivered in the format of a mid-level university diploma (Diplôme Universitaire; DU), with 3 sections: the general principles of rehabilitation practice, rehabilitation of neurological conditions, and rehabilitation of musculoskeletal conditions (Table I). The programme was delivered over 400 h of face-to-face teaching, with projects, audits, self-directed and collaborative learning, equating to a European diploma (120 credits) (17). The aim was to train at least one doctor and one physiotherapist from each of the national and regional rehabilitation centres. In total, 8 doctors from 6 centres and 10 physiotherapists began the course.
Training was delivered by volunteers, most of whom worked in clinical roles within teaching hospitals in Yorkshire, who gave their annual leave for extensive preparation and delivery of the training. Malagasy interpreters were recruited locally and paid from training programme funds.
Table I. Objectives of the rehabilitation training programme
Evaluation
A combination of qualitative methods was used for the evaluation, with informants from the UK and Madagascar. The evaluation was carried out by an independent international development, education and human resources consultant from the UK, Dr Simone Doctors (16) (Table II).
Table II. Objectives of the evaluation
The evaluation used a Theory of Change model (Fig. 1), developed by the evaluator, which set out the change pathways by which the activities undertaken were designed to produce sustainable change (18–20). The evaluation was overseen by a reference group comprised of representatives of Opt In and UK clinician and academic volunteers, the Malagasy Faculty of Medicine and MoH, and the doctors and physiotherapists who had undertaken the training.
Fig. 1. Theory of Change model for the training programme (12).
Data collection
Sixty semi-structured interviews were carried out (Table III) in Madagascar. Eight focus groups were also conducted; the 50 participants included rehabilitation doctors, physiotherapists and prosthetic/orthotic technicians from 6 rehabilitation centres (Fig. 2).
Table III. Malagasy informants for semi-structured interviews
Fig. 2. Location of rehabilitation centres in Madagascar included in the evaluation (17).
Visits were made to 4 rehabilitation units across the country, each of which had at least one doctor and one physiotherapist trained by the programme, for workplace observations and review of workplace records. The 4 units (Hôpital Joseph Ravoahangy Andrianavalona (HRJA) Antananarivo, Centre d’Appareillage de Madagascar (CAM) Antananarivo, Service d’Appareillage et Réeducation (SAR) Mahajanga, SAR Toamasina) were chosen to represent the geographical and sociological diversity of Madagascar.
In the UK, 13 semi-structured interviews were carried out with informants, including volunteers who had participated in delivering the training, members and trustees of Opt In and representatives of the teaching hospitals.
Relevant documentation was reviewed as secondary evidence including: planning documents and volunteer reports from Opt In; the MoU between LTHT, Opt In and the Malagasy partners; plans and reports from the rehabilitation units; and reports from doctors having undertaken the DU.
A literature review was carried out to place the evaluation in context within the current available literature, specifically national and international rehabilitation policy, international development, skills transmission and medical education in LMICs.
Achievement of programme objectives
All 8 doctors completed the training and passed the required assessments, including written papers and Objective Structured Clinical Examinations (OSCEs) (21). Seven of the 10 physiotherapists completed the training, some of which was specific to physiotherapy although the course was not specifically designed for physiotherapists.
The feedback from the doctors who undertook the DU was unanimously positive and everyone reported that they had gained extensive knowledge and practical skills: “The programme is very objective and recognizes the realities of our country”. Its emphasis on the practical application of rehabilitation techniques alongside theoretical knowledge was highlighted as one of the main benefits of the course. “The training did not only focus on medical conditions but also on how the doctor can improve their day-to-day clinical practice”. The physiotherapists also enjoyed the course and gained skills. However, there was some discontent expressed with regards to the lack of certification or direct career benefit for the physiotherapists.
Impact
Prior to the DU course, there was no specialist clinical training for doctors in rehabilitation medicine in Madagascar. Doctors were seconded from general practice into rehabilitation and there was no continuing professional development. The course provided them with a sound body of relevant clinical knowledge and practical skills. Several doctors went on to undertake managerial responsibilities within their units. Participants felt that it led to improved morale, motivation and confidence in dealing with an increasing caseload and leading a multidisciplinary team: “The knowledge we received from them in different training sessions, for example how to run the department, how to manage the staff, manage patient records, relationships with colleagues in other departments”.
Working practices are now changing. There is a newly learned emphasis on regular multidisciplinary team meetings and case conferences, with all patients routinely reviewed by a doctor, and rehabilitation prescriptions used to plan and tailor therapy appropriately. “Every Monday morning all the staff meet. We have a discussion, exchange information and … if there are physios or doctors who have received training, we try to share that with the others. And when there is a problem, for example with patients’ treatment, either here or in the other departments, we discuss these difficult cases together”. New links have been forged with other, related hospital specialties, for example neurosurgery and orthopaedics.
The doctors trained have become more aware of the needs of patients and their families. Most units are now accessible; all are clean, better maintained and more patient- and child-friendly. In the absence of resources, some of the rehabilitation staff were inspired to make their own improvements at their own expense (Table IV).
The many changes made have contributed to a better understanding and acknowledgement of the value of rehabilitation within the wider hospital environment and the health sector. “It is really very important to be in contact with the different hospital services because there are many patients [in these] who need our [rehabilitation] interventions”.
Table IV. Individual initiatives by doctors, physiotherapists and their teams to improve accessibility and environment of rehabilitation centres
Based on audit, data collection and basic research skills learnt in the DU, the clinicians now routinely collect clinical data that contributes to a national database (11) and are lead authors on a number of published journal articles. Rehabilitation trainees from the UK are now actively involved with their counterparts in Madagascar in conducting research and development work. Recent projects have looked at trauma rehabilitation services in Madagascar (22) describing the current service and identifying barriers to accessing treatment. Continuing support will be required to strengthen these developments along with research capacity, a vital component of long-term development (23, 24).
Benefits to individual volunteers and their institutions
The advantages to volunteers of their working abroad are well recognized (25). This evaluation highlighted several reported benefits to UK volunteers and their employers, the teaching hospital and the NHS. Experience gained on the Madagascar programme contributed to enhanced skills within their current professional role; for example, in teaching and training. Many of the volunteers took an active role in developing the training materials and presentations. They learned to adapt their teaching style to suit the Malagasy audience and deliver the training through interpreters, demonstrating an ability to be flexible and cope with challenging situations: “I have learned to work through interpreters much more effectively in Leeds, checking meaning and understanding and getting feedback from the patient”.
Volunteers also reported improvements in workplace attitudes and overall morale and motivation. The volunteers developed a new appreciation for, and commitment to, their clinical roles after seeing the commitment of their Malagasy counterparts working in poorly resourced situations. They reported a heightened awareness of the opportunities available to them in the UK and placed greater value on the infrastructure, facilities and equipment in UK hospitals.
Sustainability and ongoing impact beyond the evaluation
There has been much positive ongoing work since the evaluation was carried out. Whilst these examples are not directly as a result of the DU, they flow from the graduates of the course who are setting up services, identifying needs and developing plans with the support of colleagues in Madagascar and the UK.
Following completion of their training, the 8 rehabilitation doctors went on to form a professional organization, the Association of Physical and Rehabilitation Medicine Madagascar (AMPR Mada) (26). They held their first international teaching congress in 2014, focussed on rehabilitation of children with cerebral palsy. The UK team provided support for the development and delivery of this congress, including the production of a workbook, which forms the basis for national guidelines on the topic. Further congresses focussed on stroke rehabilitation in 2016, and management of club foot in 2018. The Malagasy rehabilitation doctors were also supported to attend the African Spinal Cord Injury Network (AFSCIN) meetings (27) and the Southern African Spinal Cord Association (SASCA) conferences (28). These meetings have brought networking opportunities and Madagascar has now joined AFSCIN as an active member, with a representative on the executive board, and plans for the national congress in 2020 to have spinal cord injury rehabilitation as its main topic.
An outcome of considerable national importance was the development of a specialist rehabilitation team for acute spinal cord injuries in HJRA (29). The team, led by Dr Renaud Rakotonirainy, consists of a rehabilitation physician, 2 specialist nurses and a physiotherapist. This service has shown great success in reducing complications such as pressure ulcers and urinary tract infections (29, 30). Dr Rakotonirainy is now supporting the development of a second service in Fianarantsoa, which is due to start in 2019.
The treatment of clubfoot, a common, disabling, but treatable, childhood condition, has been transformed in Madagascar since the introduction of the Ponseti method. Crucial to this success was a joint study with Malagasy and UK partners into problems faced by parents in accessing this treatment. This not only led to service changes, but helped to secure funding to facilitate uptake of this method (11).
As part of efforts to build the multidisciplinary team, an orthotist from Madagascar was supported to attend training at the Tanzania Training Center for Orthopaedic Technologists (TATCOT), a training school recognized by the International Society for Prosthetics and Orthotics (ISPO) in 2018 (31).
This paper has described the evaluation of a specific teaching and professional development programme co-designed by Malagasy and UK rehabilitation professionals, based on a robust needs analysis. It led to a series of enduring improvements in rehabilitation services in Madagascar.
Key factors for success
The evaluation identified a number of key factors that led to the successes (Table V), as presented briefly below.
Table V. Key factors for success of a global training partnership
Key factors for success
The evaluation identified a number of key factors that led to the successes (Table V), as presented briefly below.
Clearly-focussed aim. The programme had clear, locally determined aims from the outset, with a focus on skills transfer. This is in line with Larkan’s framework for global health partnerships, which states that having a clear focus with common goals is the first step in achieving a successful partnership (32). It was understood from the beginning that it would not tackle wider issues, such as requests for equipment or material help. This was important, given the limitations of budget and time.
Strong collaborative leadership. Much of the pro-gramme’s success can be attributed to the collaborative leadership from Malagasy and UK individuals. Dr Sonia Adrianabela from the Malagasy MoH was a crucial figure with the drive and experience to make change possible. Her clear vision and political astuteness were pivotal in the programme’s success. In the UK, Professor Anne Chamberlain was the driving force behind the development of the DU. She provided strong leadership based on her experiences of developing rehabilitation services over 3 decades in the UK. The 8 “Principles of Partnership” outlined by the Tropical Health and Education Trust (THET), which focus on building sustainable partnerships, place emphasis not only on the role of each organization, but also of individuals committed to effecting change (33–35).
Cooperative approach. The 2 countries adopted a cooperative approach throughout the development of the programme, with common goals and motivations. This mutual support and commitment to joint learning was highlighted by the evaluation and has led to the development of a lasting reciprocal relationship. This is reflected in John et al.’s 2016 article, whose main resulting theme for success of a global research partnership was “mutual respect and benefit” (36).
Demand driven, based on local needs. Importantly, the training programme was developed with a ground-up approach; the teaching methods and topics were directly related to the needs of the Malagasy clinicians and their patients.
Commitment and motivation from trainees. One of the key factors in this success was the Malagasy trainees, who were receptive to the teaching and had a clear vision of what they wanted to achieve, allowing them to surpass the expected outcomes of the programme and achieve wider change. Involving trainees in the development of programmes and empowering them to make change can help to build and maintain motivation and commitment.
Skilled and motivated trainers. The volunteers who gave their time to teach had the relevant clinical skills and the necessary attitudes and personal attributes to work effectively in a challenging, low-resource environment. They received pre-departure training and support whilst in-country. The benefits of volunteering abroad are well-recognized and are discussed in a UK parliamentary report “Improving health at home and abroad”, which highlights the importance of volunteers having the correct skills, attributes and experience for the task (25).
Support from Ministry of Health and Faculty of Medicine. The DU programme was part of the University of Antananarivo’s Faculty of Medicine, but was developed with the close involvement of key members of the Malagasy MoH. This ensured that it was institutionally embedded, locally appropriate and relevant. It also guaranteed the necessary logistical and administrative support.
Strategic vision and integration into national policy. The training was seen as providing a crucial contribution towards the coordinated vision set out in the PNDSR 2010–2015, the MoH’s first national plan for the rehabilitation sector, which was developed with local partners in consultation with the WHO (37). In addition, the training programme benefitted from the support of international non-governmental organisations, with leadership from the MoH, thus helping to effect change (Fig. 1).
Sustainability. Following the DU, volunteers from Leeds returned to Madagascar twice in 2014 and in each subsequent year to consolidate the learning and to train those who will be training rehabilitation clinicians in the many other centres. The UK and Malagasy teams have developed a strong relationship with ongoing regular contact between individuals.
Barriers to success
Costs. The overall costs of the programme were modest, and represented “exceptional value for money, compared with the costs of comparable training by commercial trainers” (16). However, doctors were required to pay tuition fees for the DU and there were additional travel and accommodation costs. It is perhaps an indicator of their enthusiasm that many were prepared to meet these costs, although some expressed discontent.
Lack of accreditation/recognition. A source of dissatisfaction for the physiotherapists was the lack of certification. Although the doctors received DU accreditation, this did not translate to any career advancement or formal institutional recognition for the skills gained.
Need to formalize ongoing training. The DU was delivered as a series of short courses, in part due to the availability of UK volunteers. (To date, the DU course has not been repeated, but discussions are ongoing for the DU programme, as developed by Opt In and the teaching hospitals, to be continued by the newly formed Global Rehabilitation charity www.globalrehabilitation.org). There now needs to be a focus on succession planning, to identify local programme leaders with the requisite skills and commitment to carry the training forward. This may be in the form of a formal and accredited Continuing Professional Development (CPD) model, whereby regular training is embedded within ongoing service plans (38). Training in leadership and management emerged as a significant need. Many of the doctors now have managerial responsibilities, but few have undergone formal training in this area.
Wider conditions. The remit of the training programme was highly focused towards skills transfer. However, there remain wider limiting factors and material needs, which are key to overall improvement of the rehabilitation service. In addition, there remains a lack of trained staff in allied health professions, with only 8 qualified occupational therapists in Madagascar. There are currently no speech and language therapists in the public sector, but strong awareness of the need.
Limitations of the evaluation
This evaluation used only qualitative methodology. Only change at the level of the direct beneficiaries of the training was considered. The impact on indirect beneficiaries, such as patients and families, was not assessed, although evidence from these was included. The evaluation did not aim to include any national or international data to assess for macro-level change.
Conclusion
The success of this programme is a source of great pride to all those involved. It enhanced the trainees’ clinical knowledge and skills, attitudes and working practices. UK volunteers gained skills applicable to their NHS practice. Strong leadership with a clear vision based around local needs was key to the programme’s success, as was the mutual respect and enthusiasm of all involved. The programme also benefitted from its integration within a wider, coherent plan for the rehabilitation sector. Rehabilitation training programmes fulfil a need to strengthen the healthcare workforce, particularly in LMICs, where the burden of disability is greatest. These programmes can be undertaken at modest cost through global health partnerships, with significant benefit to both parties. It is hoped that the key learning points from this evaluation may serve in developing a model of implementation for future training programmes in other settings.
The authors would like to acknowledge all participants and organizations who contributed to the evaluation, included those mentioned in Table III. In particular we thank Dr Sonia Andrianabela, Professor Luc Samison and Professor Gaétan Duval Solofomalala for their support of the teaching and evaluation. We pay tribute to the volunteers who contributed in many ways to the delivery and evaluation of the project. We also acknowledge and thank the members and trustees of Opt In for their funding and support. RJOC’s research is supported by the National Institute for Health Research (NIHR) infrastructure at Leeds and Sheffield. The views expressed are those of the authors only.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize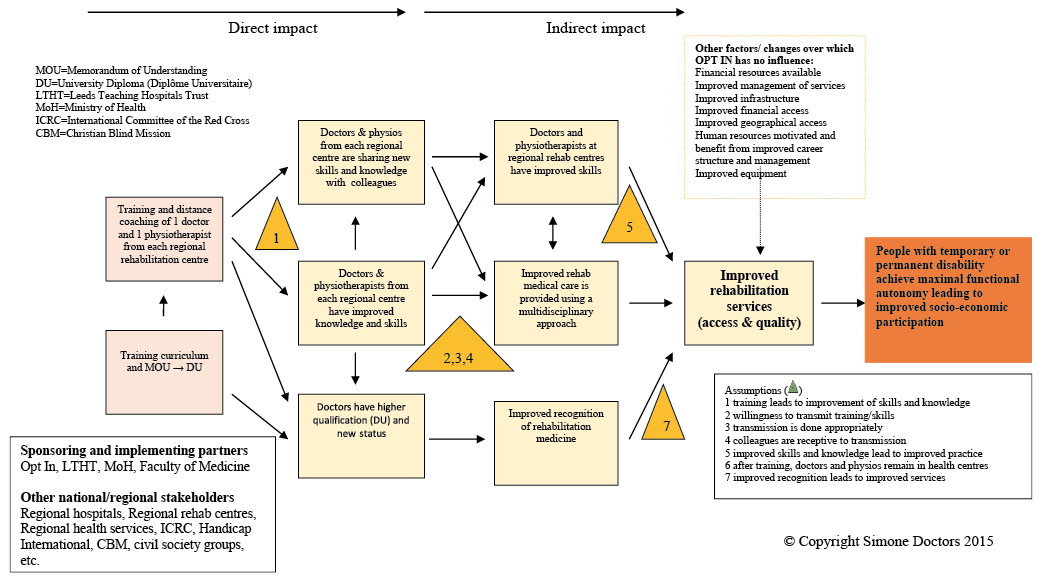 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize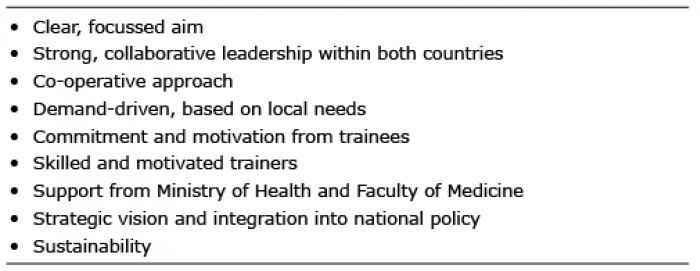 Click to show fullsize
Click to show fullsize