
From the 1Department of Physical Medicine & Rehabilitation, Schulich School of Medicine & Dentistry, Western University and 2Parkwood Institute, St Joseph’s Health Care, London, Ontario, Canada
Objective: Burnout, a state of emotional exhaustion related to work or patient-care activities, is prevalent in all stages of medical training and clinical practice. The syndrome has serious consequences, including medical errors, poorer quality of care, substance abuse, and suicide. The aim of this study is to evaluate the prevalence of burnout in Physical Medicine & Rehabilitation (PM&R) specialists and trainees.
Methods: Systematic literature searches were conducted in MEDLINE, CINAHL and EMBASE for peer-reviewed articles in English before March 2019 about the prevalence of burnout amongst PM&R specialists and trainees.
Results: This systematic review yielded 359 results. Of these, 33 full-text records were reviewed; 5 met the inclusion criteria: 3 surveys of PM&R specialists and 2 of PM&R residents (total n = 1,886 physicians; year of publication 2012–2019). Data extracted included prevalence and severity of burnout and, if avail-able, risk or protective factors. Data were analysed using descriptive statistics. Incidence of burnout ranged from 22.2% to 83.3% in trainees and 48% to 62% in specialists. Organizational and system challenges were the primary risk factors for burnout amongst specialists.
Conclusion: Emerging evidence positions physicians in PM&R among the most likely to experience burnout. Although there is limited literature regarding PM&R specialists and trainees, the available evidence suggests that more than half of physicians in PM&R experience burnout.
Key words: Physical Medicine and Rehabilitation; burnout, professional; physician impairment; residency; review.
Accepted Oct 2, 2019; Epub ahead of print Oct 14, 2019
J Rehabil Med 2020; 52: 00–00
Correspondence address: Emma A. (Ali) Bateman, Department of Physical Medicine & Rehabilitation, St Joseph’s Health Care London, Parkwood Institute, Main Building, PO Box 5777, Station B,,N6A 4V2, Canada. E-mail: eabateman@gmail.com
Professional burnout, emotional exhaustion and loss of satisfaction with patient care affects doctors at all stages of their career, from residency trainees to certified specialists. Burnout is a critical emerging issue facing specialists and trainees of all disciplines. Burnout in doctors is linked to serious negative outcomes for patients, including higher rates of medical errors and poorer quality of care. It is also linked to negative outcomes for doctors, including substance abuse and suicide. Although burnout is a serious problem, little is known about burnout in specialists and trainees in Physical Medicine & Rehabilitation (PM&R). Historically, it was thought that doctors in rehabilitation medicine were less likely to experience burnout than doctors in other specialties. A systematic review was conducted to understand if burnout is in fact a problem for doctors in PM&R. It was found that more than half of all rehabilitation doctors, including specialists and trainees, experience burnout; a higher rate than for non-rehabilitation doctors. Working in PM&R is a unique risk factor for burnout among doctors. Important next steps will be to understand what causes such high rates of burnout and what can be done to help.
More than half of all practicing physicians experience symptoms of burnout, a psychological syndrome characterized by emotional and physical exhaustion, reduced sense of personal accomplishment, and depersonalization, in response to chronic interpersonal stressors related to patient care (1, 2). This psychological syndrome is prevalent in all stages of medical training, including medical students (28–45%), residents (27–75%) and practicing physicians (37–72%) (1, 3). Physicians and trainees who report symptoms of burnout are at heightened risk of committing medical errors, delivering poorer quality of care, experiencing reduced career satisfaction, career discontinuation, substance abuse, and suicide (4, 5). As a crucial factor in the quality of care delivered by physicians, burnout is therefore important not only to the medical profession, but also to patients, healthcare institutions, and societies. Importantly, burnout is both preventable and treatable (5, 6).
Freudenberger first described burnout in 1974 in the context of severe or prolonged stress in providing “healing” care to marginalized persons (6). In 1981, Maslach et al. characterized the 3 key tenets of burnout: emotional exhaustion, depersonalization, and a decreased sense of accomplishment, which are captured in the Maslach Burnout Inventory (MBI), the gold standard for assessing burnout (8). In the 44 years since Freudenberger first described burnout, researchers have attempted to elucidate risk and protective factors for burnout. Although it is well-established that physicians are at increased risk of burnout compared with the general population, other factors that increase a physician’s risk of developing burnout vary by study, with few studies yielding reproducible results (1, 2, 9–12). Among the heterogeneous findings, individual, system, institutional, and patient factors have been shown to play a role (4, 6, 10, 12).
Medical specialty has been shown to play a role in predisposing specialists and trainees to burnout, but the specialties found to be at highest risk varies by study (1–3, 10–11). Little is known about burnout in PM&R. In their role caring for persons with disabilities and after catastrophic accidents, physiatrists are adept at fostering resilience amongst their patients, which may confer resilience as physicians, although the high degree of empathic demand may, conversely, increase the risk of emotional exhaustion. This systematic review aims to consolidate available literature to enhance our understanding of this critical problem in a potentially vulnerable physician population.
Objective
To evaluate the prevalence of burnout in PM&R specialists and trainees. This systematic review was registered with the International Prospective Register of Systematic Reviews (PROSPERO, registration #CRD42018104133).
Inclusion criteria
Studies reporting the prevalence of burnout in specialists and/or residents in PM&R were included. Studies that grouped PM&R specialists or residents with healthcare providers from other medical disciplines were excluded, unless PM&R-specific outcomes were reported separately.
Search strategy
Systematic literature searches were conducted in MEDLINE, CINAHL and EMBASE for peer-reviewed full text articles and published abstracts in English published before 1 July 2018, using a combination of keywords and Medical Subject Headings (MeSH). The search strategy is shown in Appendix I. Hand searches of studies for which the full text was reviewed were used to identify other relevant citations. During manuscript preparation, the authors became aware of additional potentially relevant publications from September 2018 and January 2019, after the initial systematic review search strategy was completed. Updated systematic searches were performed in February 2019 using the same search strategy to ensure the inclusion of relevant studies. The authors became aware of a retraction and replacement (13) applicable to one of the included studies during the course of manuscript preparation; the reasons for retraction were reviewed and data extracted was revised to reflect the replacement. Citations obtained from the searches were screened for eligibility by 2 independent reviewers (EAB and RV). Disagreements between the reviewers were resolved by discussion to reach consensus. Agreement between reviewers was determined using Cohen’s kappa.
Data extraction
Data extracted included number of participants, recruitment method, participant characteristics (career stage, sex, age), country of study, year of publication, study methodology, tool or criteria used to assess burnout, incidence and severity of burnout and, if available, prevalence of depression, suicide, measures of wellness including resiliency and satisfaction, and risk or protective factors. Data were compiled using a standardized collection form.
Data analysis
Data were analysed using descriptive statistics. Content analysis was performed for qualitative data. Risk of bias was assessed using the Cochrane Risk of Bias Tool (14).
Study selection
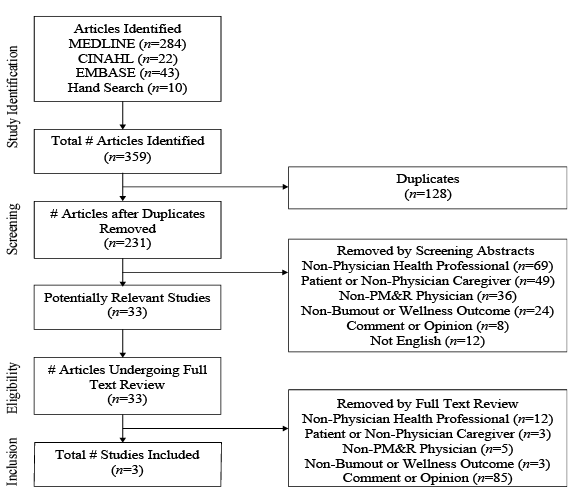
The search strategy yielded 359 articles, of which 128 were duplicates. A total of 33 articles underwent full text review, and 5 met the inclusion criteria (Fig. 1). Four articles (1, 2, 11, 12) were peer-reviewed publications, and one (15) was a peer-reviewed abstract. Cohen’s kappa was 0.89 between the 2 reviewers, indicating excellent agreement in identifying the relevant studies.
Fig. 1. PRISMA study selection flow chart. Flow chart of strategy used for study selection.
Study features
All studies meeting the inclusion criteria were cross-sectional surveys. Their characteristics and findings are summarized in Table I. Convenience sampling was used in one study (15) of residents and fellows; purposive sampling was used in one study (12) of PM&R specialists; and modified stratified random sampling was used in 2 studies (1, 2) of PM&R and other physician specialists and one study (11) of residents in PM&R and other specialties. The year of publication ranged from 2012 to 2019. All 5 studies were based in the USA. A total of 1,886 PM&R trainees and specialists were surveyed (83 trainees, 1,803 specialists). One study surveyed American board-certified PM&R specialists, 2 studies surveyed PM&R and other specialists, one study surveyed PM&R residents stratified by postgraduate year, and one surveyed PM&R and other residents. All studies used the MBI or its components to measure burnout, except one study (12) which used one item from the Mini-Z Burnout Survey. In addition, 2 studies measured depression and suicidal ideation using the 2-item Primary Care Evaluation of Mental Disorders, and a single item for suicidal ideation and self-reported satisfaction (1, 2). One study evaluated career choice regret using 2 items for which PM&R-specific data were available; this study also evaluated anxiety using the Patient-Reported Outcome Measurement Information System (PROMIS) anxiety short form, empathy using 8 items from the Jefferson Scale of Physician Empathy, and availability of social support using the Tangible Support and Emotional Support subscale of the Medical Outcomes Study Social Support Measure, but PM&R-specific results were not published (11). One study identified risk or protective factors for burnout in PM&R specialists. No studies reported on wellness or resilience.
a”During the past 12 months, have you had thoughts of taking your own life?”. bMy work schedule leaves me enough time for my personal/family life. c”If you could revisit your career choice, would you choose to become a physician again?” and “If you could revisit your specialty choice, would you choose the same specialty again?”. dMaslach Burnout Inventory single item “I have become more callous towards people since I took this job.”
MBI: Maslach Burnout Inventory (22-item); PCEMD: Primary Care Evaluation of Mental Disorders; JSPE: Jefferson Scale of Physician Empathy; PROMIS: Patient-Reported Outcomes Measurement Information System; TSES: Tangible Support and Emotional Support subscale of the Medical Outcomes Study Social Support Measure; MOSSM: Medical Outcomes Study Social Support Measure.
Risk of bias
All of the studies meeting inclusion criteria were surveys (level of evidence III); none of the studies meeting inclusion criteria were controlled trials. None of the included studies reported a priori clinical trial registration. None of the included studies described investigator blinding for MBI or other outcome measure assessment. Three studies (1, 2, 11) did not advise participants that they were measuring burnout as the purpose of assessment, consistent with best practices for administering the MBI; one study (15) did not disclose this practice; one study (12) asked participants to self-identify as burned out, which qualified them as experiencing burnout. Complete data were not reported in one of the included studies (15) in which the authors did not describe the total number of physicians available to be surveyed; this report by Kao et al. is a published abstract with minimal methodological information (15). No other sources of bias were identified. The overall study quality is low, due to the survey methodology, small sample sizes, and population-based assessment of burnout. Based on the Cochrane Collaboration’s tool for assessing risk of bias (14), all studies may be subject to detection bias, and 2 studies have a very high risk of reporting bias (12, 15).
Burnout prevalence
The prevalence of burnout in PM&R specialists was reported in 3 studies (1, 2, 12); the weighted mean prevalence of burnout amongst PM&R specialists was 51.6%. In a survey of physicians from multiple specialties, burnout amongst physiatrists increased from 48% to 62% between 2012 and 2015, respectively, and was consistently higher than the mean for physicians across all specialties (1, 2). During this time, the prevalence of burnout increased by 29% amongst PM&R specialists, 1.5 times the rate for all specialists. Out of 24 specialties, PM&R increased from 10th highest prevalence of burnout to 3rd highest. Being a specialist in PM&R was an independent predictor of having burnout (1). The odds ratio for burnout in PM&R specialists compared with primary care physicians was 1.6 (1). In a 2019 survey of 1,536 American board-certified physiatrists, 50.7% self-identified as being burned out based on the Mini-Z Burnout Survey (12).
Amongst PM&R residents, Kao et al. found the prevalence of burnout ranged from 22.2% in new PGY4 residents to 83.3% in residents at the end of PGY2 in their convenience sample of 53 residents and fellows at one institution (15). The national survey of second-year residents carried out by Dyrbye et al. found the prevalence of burnout in PM&R residents to be 50.0% based on 30 survey respondents (11). This was higher than the mean for all residents (45.2%). The relative risk for burnout in PM&R residents was 1.17 compared with internal medicine residents (11).
Other measures of physician distress and wellness
Only one study (12) characterized factors that specialists in PM&R felt contributed to burnout. It found that increasing regulatory demands, workload and job demands, and practice efficiency or lack of resources were the causes physicians identified as contributing to burnout. This was true for burned out PM&R specialists and those that did not meet the criteria for burnout. In this study, job satisfaction, stress, control over workload, insufficient time for documentation, and misalignment of values with departmental leaders were significantly associated with burnout. No individual factors, such as age, sex, or number of years in clinical practice, were associated with burnout.
With respect to other measures of physician wellbeing or distress, 3 studies (1, 2, 12) characterized work-life balance satisfaction in PM&R specialists, and 1 (11) characterized career choice regret amongst resident physicians. PM&R specialists reported slightly below-mean satisfaction with work-life balance in 2012, and slightly above-mean satisfaction with work life balance in 2015, despite an overall decrease in satisfaction and an above-mean rate of burnout in both studies (1, 2). Residents in PM&R were more likely to experience career choice regret (prevalence 16.7%) than residents on average (prevalence 14.1%) (11); the relative risk for career choice regret was 1.37 compared with internal medicine residents (11). Two (1, 2) studies characterized risk factors for burnout in specialist physicians and one (11) in second-year residents across all specialties, but did not report PM&R-specific data.
Current evidence about burnout amongst physiatry specialists and trainees is limited. The available data consists of 5 studies examining 1,886 PM&R specialists and trainees in an exclusively American context. Given this narrow focus, the authors take a cautious approach to generalizing these results to the field of PM&R as a whole. However, physicians in PM&R must not dismiss burnout based solely on limited evidence; this limited data paints an alarming picture of higher than average prevalence of burnout in PM&R specialists and trainees. At present, there is no available data to explain why physiatrists experience the third highest rates of burnout amongst specialists and, as such, comprehensive analysis is beyond the scope of the present review. However, amongst all physicians, system and institutional factors were identified as the greatest contributors to the development of burnout (12). It is possible that system factors, such as challenges accessing affordable allied healthcare specialists, such as physiotherapy, appropriate equipment, and affordable accessible housing, may disproportionately affect physiatrists. Alternatively, institutions may not provide adequate access to administrative and allied healthcare team supports. Although possible, it is difficult for the authors to accept that such problems are unique to specialists and trainees in physiatry. The present study emphasizes the need for additional research to understand whether high rates of burnout are unique to the USA, potential causative factors, and rates of burnout in allied health disciplines.
In the present study, the authors were surprised by the paucity of data outside of the American context. The fundamental structural differences between the American healthcare system, in which most individuals’ healthcare is purchased in a private marketplace with a multi-payer system, and socialized, single-payer systems which are most common in Canada and Europe (16), make it difficult to determine whether system and organizational factors contribute to burnout in physicians in the same way. One study from Italy that did not meet inclusion criteria for this review examined burnout in a multidisciplinary rehabilitation team, finding a “medium-low” pooled level of burnout amongst all team members, including physicians and other allied healthcare workers (17). Although this study did not report the prevalence of burnout in physicians or other allied health providers, such as physiotherapists, understanding the prevalence and risk/protective factors for burnout amongst all members of multidisciplinary teams may be critical for individuals and institutions committed to tackling burnout and developing organizational culture that promotes wellbeing.
Limitations of this systematic review include the exclusion of non-English language studies, and the narrow scope, focussing solely on burnout rather than all mental or physical ailments that might contribute to physician distress. The present study is also limited by the small number of available studies, small sample sizes in many of these studies, low quality and American-only evidence of PM&R-specific burnout literature.
Scientific journals specific to rehabilitation medicine have featured diverse opinions on burnout, ranging from acknowledging that physicians in PM&R are at increased risk by the nature of work they do (18), to rebuking burnout as a legitimate condition threatening physician wellbeing and viewing it as a “myth” and a “cop-out” (19), to describing the prevalence of burnout as a research priority (20). This systematic review presents evidence that strongly challenges the notion that burnout amongst physiatrists is a myth, and underscores the need for additional research to evaluate the prevalence of burnout in PM&R physicians outside of the American context, to confirm or refute current evidence with larger sample sizes, to explore why physicians in PM&R experience such high rates of burnout, and to better understand risk and protective factors specific to physiatrists. Given that burnout has well-established detrimental consequences for physicians, patients, and healthcare institutions, the physiatry community needs to take burnout seriously, particularly because burnout is preventable and treatable (5–7). As a crucial first step, it must be acknowledged that burnout is prevalent in PM&R.
There is no consensus on how best to prevent or treat burnout. To date, the authors are not aware of any studies of prevention or treatment of burnout in specialists or trainees in PM&R. Previous recommendations ranged from individual and organizational interventions (5, 7, 22) to focusing on physiatrists’ mission (20) to using collective action to target root causes of marginalization amongst our patients (21). On an individual level, PM&R specialists and trainees should be given tools to understand, prevent, identify, and treat burnout. Establishing relevant core competencies in residency training and continuing medical education resources for specialists are two important ways to start. However, placing the onus solely on individuals, and judging burnout as an individual problem, ignores the larger context in which burnout develops. National associations outside of the USA should also undertake to better understand the prevalence of burnout in their members, possible risk or protective factors, and design further initiatives around these findings. Our understanding of putative risk factors amongst physiatrists comes from a single large study (12) that identified system and institutional factors as the main drivers of burnout in PM&R specialists. The authors therefore recommend that departments, institutions, and national associations make burnout a priority to support the health and wellbeing of PM&R specialists and trainees, which is an investment to ensure the delivery of the best possible rehabilitative care.
Conclusion
As far as the authors are aware, this is the first systematic analysis of literature regarding burnout in PM&R. Three studies report burnout prevalence in specialists in PM&R and 2 report burnout in trainees in PM&R. The prevalence of burnout ranged from 48% to 62% in surveys of USA-based PM&R specialists; the prevalence of burnout ranged from 22.2% to 83.3% in trainees in different stages of training at one institution, and was 50% in a national survey of second-year residents. In the only study (12) reporting risk factors for burnout amongst physiatrists, system and institutional factors were the main drivers of burnout; individual factors were not significantly associated with burnout. All 5 studies use survey methodology and are of low-quality evidence. All available data come from a single country; there is no data on the prevalence of burnout in PM&R specialists or trainees outside of the USA, indicating a significant gap in knowledge.
The authors thank the Department of Physical Medicine & Rehabilitation at Western University for making physician wellness a departmental priority.
The authors have no conflicts of interest to declare.
Appendix I. Search strategy


 Click to show fullsize
Click to show fullsize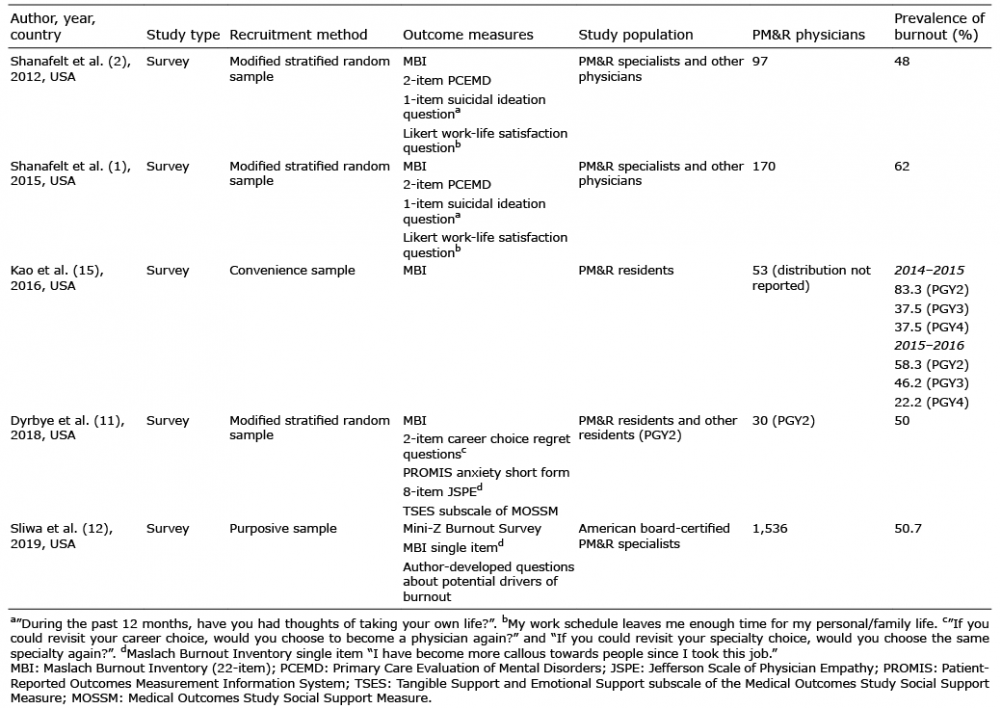 Click to show fullsize
Click to show fullsize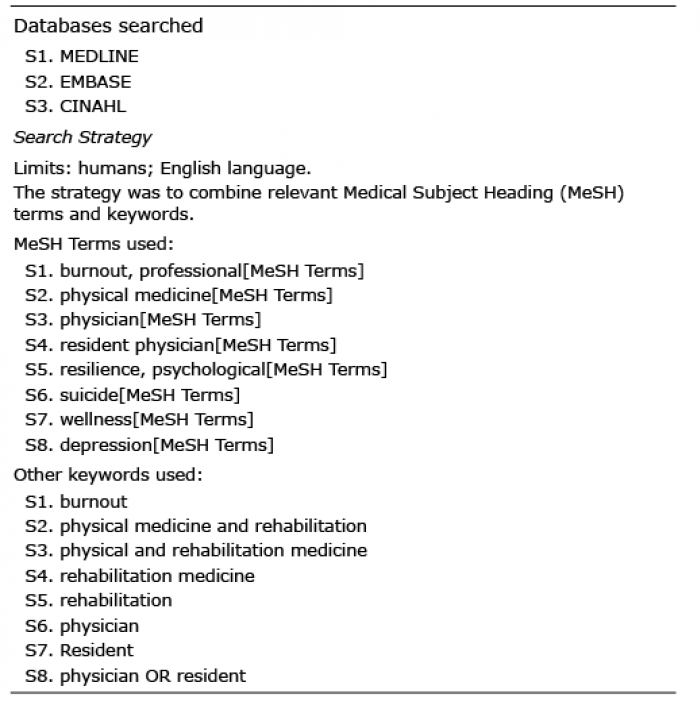 Click to show fullsize
Click to show fullsize