
From the Department of Orthopedics and National Clinical Research Center for Geriatrics, West China Hospital, Sichuan University, Chengdu, Sichuan, China.
*These authors contributed equally to this work.
Objective: To evaluate the efficacy of classical pulsed electromagnetic field therapy on patients with knee osteoarthritis.
Methods: The databases PubMed, EMBASE, Web of Science and Cochrane Library were searched for relevant studies. Randomized controlled trials comparing classical pulsed electromagnetic field with placebo for patients with knee osteoarthritis were included. Data for primary outcomes, including pain, stiffness and physical function, were extracted. Data from 8 randomized controlled trials involving 421 patients were pooled.
Results: Pulsed electromagnetic field therapy had an effect on improving physical function (weighted mean difference; WMD = −5.28, 95% confidence interval; 95% CI −9.45 to −1.11, p = 0.01), but showed no advantage in the reduction of Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) total score (WMD = −7.80, 95% CI −16.08 to 0.47, p = 0.06), WOMAC pain score (WMD = −1.06, 95% CI −2.30 to 0.17, p = 0.09), visual analogue scale pain score (WMD=−0.88, 95% CI −2.06 to 0.31, p = 0.15) or WOMAC stiffness score (WMD = −0.50, 95% CI −1.09 to 0.09, p = 0.1).
Conclusion: Pulsed electromagnetic field therapy is beneficial for improving physical function despite having no advantage in treating pain and stiffness. Further randomized controlled trials are needed to confirm these findings and determine the optimal parameters and treatment regimen for pulsed electromagnetic field therapy.
Key words: pulsed electromagnetic field; knee osteoarthritis; systematic review; meta-analysis; randomized controlled trial.
Accepted Sep 25, 2019; Epub Oct 4, 2019
J Rehabil Med 2020; 00: 00–00
Correspondence address: Zhou Xiang, Department of Orthopedics and National Clinical Research Center for Geriatrics, West China Hospital, Sichuan University, Chengdu, Sichuan, China, 610041, China. E-mail: xiangzhou15@hotmail.com
Knee osteoarthritis is currently one of the most common joint diseases worldwide. Pulsed electromagnetic field therapy has become popular among patients with knee osteoarthritis in recent years. However, the efficacy of this therapy on joint pain, joint stiffness and physical function is regarded as controversial in published clinical trials and systematic reviews. Several new randomized controlled studies on this subject have been published recently. The aim of this systematic review and meta-analysis is therefore to assess the efficacy of classical pulsed electromagnetic field therapy on patients with knee osteoarthritis, according to the methodology set out in the Cochrane Handbook for Systematic Reviews of Interventions. The results show that, despite showing no advantage in the management of pain and stiffness, pulsed electromagnetic field therapy is beneficial for improving clinical symptoms, such as physical function of the knee joint; thus it may be recommended as a supplementary therapy option for knee osteoarthritis. This review provides some evidence to help resolve current controversies about the efficacy of pulsed electromagnetic field therapy for knee osteoarthritis.
Osteoarthritis (OA) is one of the most common joint strain diseases, and it is generally considered that ageing, obesity, strain and trauma play important roles in the development of OA (1). The main pathological features of OA are degeneration of articular cartilage and reactive hyperplasia of the articular margin and subchondral bone, which can result in chronic pain, stiffness and physical disability (2). In general, OA occurs mainly in weight-bearing areas, such as the knees, hips and spine, with knee OA having the highest prevalence among middle-aged and elderly people (3). At present, the main aims of conservative therapy for knee OA are to relieve pain and enhance joint mobility using treatments such as oral medication, intra-articular drug injection and physiotherapy (4). Although total knee arthroplasty has proved an effective method of treating knee OA, it is not suitable for all patients. In addition, total knee arthroplasty cannot be a permanent solution because patients often need reoperation within 20 years (5). Therefore, it is necessary to validate effective treatments that are beneficial in relieving pain, improving physical function, and blocking the process of joint destruction, so as to delay or avoid surgical options.
Since the 1970s, pulsed electromagnetic field (PEMF) therapy has provided an alternative approach to treating bone and joint diseases, especially for elderly patients or those with certain hepatorenal insufficiency who are unable to undergo surgery or take medications (6). Moreover, a large body of basic research has shown that PEMF therapy can promote the proliferation of chondrocytes and the secretion of chondrocyte extracellular matrix, which are beneficial to the repair of cartilage damage caused by knee OA (7). However, a series of randomized controlled trials (RCTs) and systematic reviews on the therapeutic effects of PEMF therapy in the clinical treatment of knee OA have yielded controversial results about joint pain, stiffness and physical function (8). In 2013, Ryang et al. (9) conducted a systematic review of PEMF therapy in the treatment of knee OA, which showed that studies with high-quality or low-quality methodology may report different therapeutic effects of PEMF therapy. Nevertheless, these 4 published systematic reviews (9–12) contained either studies with low-quality metho-dology or studies that reported the results not of classical PEMF therapy but of pulsed short-wave therapy.
Thus, based on controversial clinical trials and systematic reviews, the therapeutic effects of classical PEMF therapy in the management of knee OA remain to be validated in this context. Several new RCTs on this subject have been published recently. The aim of this systematic review and meta-analysis of randomized placebo-controlled trials was therefore to assess the efficacy of classical PEMF therapy on joint pain, joint stiffness and physical function in patients with knee OA.
This systematic review and meta-analysis was based on previously published literature according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement, thus it was deemed exempt by the ethics committee of West China Hospital, Sichuan University, Chengdu, China (13).
Search strategy
Electronic databases, PubMed, EMBASE, Web of Science, and the Cochrane Library, were searched from inception to April 2018 to obtain relevant studies. The main search method was to use both MeSH and the keyword “knee OA”, combined with electromagnetic fields [MeSH] OR pulsed electromagnetic field OR pulse electric-magnetic field OR PEMF OR magnetotherapy OR magnetic therapy. The publication type was limited to clinical trials or RCTs. In addition, a hand search was performed to identify the relevant references included in articles.
Inclusion and exclusion criteria
Inclusion criteria for studies in this meta-analysis were:
All patients had a clear diagnosis of chronic knee OA based on the clinical or radiological criteria of the American College of Rheumatology, with no restrictions on sex or race.
Treatment should be classic PEMF therapy, rather than short-wave, electrical stimulation, magnetic resonance, or other physical therapies.
The control group should be a placebo group.
Patients’ baseline and primary outcome both presented the severity of joint pain, assessed by Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) questionnaire or 10-cm visual analogue scale (VAS) for pain (where 0 means no pain, and 10 means pain as severe as the subject can imagine). The WOMAC questionnaire contains 24 items divided into 3 subscales: pain (5 items), stiffness (2 items), and physical function (17 items). A higher WOMAC score represents a worse outcome (14).
Studies must be RCTs.
Exclusion criteria were:
Animal or laboratory studies.
Studies evaluating the severity of joint pain using the Knee Injury and Osteoarthritis Outcome Score (KOOS).
Insufficient research data, knee OA participants not reported separately, data not extractable, or the corresponding authors did not respond so that they could not be statistically analysed.
The full text of the research was published in a language other than English.
Study selection
First, 2 reviewers independently evaluated the eligibility of the studies by reading the title and abstract according to the aforementioned criteria. If the abstract information was insufficient to judge eligibility, further screening would be performed by obtaining the full text. Disagreements were first resolved through discussion; otherwise a third reviewer would conduct an independent review if necessary.
Data extraction and quality assessment
A standard data extraction spreadsheet was used to collate basic information from the eligible studies, including first author, year of publication, number of patients, age, sex, body mass index, disease duration, pulse frequency, magnetic flux density, and treatment regimen. The primary outcomes were then extracted, including joint pain, joint stiffness, and physical function, as assessed by WOMAC scores or VAS-related measurement. Data evaluated between 3 and 6 weeks after the start of treatment were used to analyse the efficacy of 1 month’s treatment. Data presented in other forms, such as 95% confidence interval (95% CI) and standard error were converted to a form of mean and standard deviation (SD) according to the Cochrane Handbook for Systematic Reviews of Interventions (available from http://handbook.cochrane.org). When the raw data provided only baseline values and values of changes in the form of mean and SD, the mean and SD of the endpoint values were calculated using the formula provided by the Cochrane Handbook for Systematic Reviews of Interventions. All data extraction was carried out independently by 2 reviewers and any disagreements were resolved through discussion. However, when disagreements failed to reach a consensus, the source data were re-examined and a third reviewer was consulted.
As all included studies were RCTs, 2 reviewers used Review Manager (RevMan) version 5.3 (The Cochrane Collaboration, Oxford, UK) to independently assess the risk of bias in accordance with the method recommended by the Cochrane Handbook for Systematic Reviews of Interventions. The content of the assessment consisted mainly of the following items: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other bias. There were 3 evaluation options for each item: low risk, high risk, and unclear, based on the original research. A third reviewer participated in the assessment when differences could not be resolved through discussion.
Statistical analysis
Weighted mean differences (WMD) and 95% CIs were used to estimate the pooled effects for continuous outcomes, including VAS for pain and WOMAC scores. In addition, Cochrane’s Q test and the I2 test were used to evaluate heterogeneity among all studies. When the I2 test value exceeded 50%, indicating high heterogeneity, a meta-analysis was performed using a random effects model, whereas a fixed effects model was chosen when the I2 test value was 50% or less. In addition, sensitivity analysis was performed by eliminating each study in turn so as to estimate the effect of a single study on overall heterogeneity and pooled effects. Publication bias was not performed, due to the limited number of studies (n < 10) included in this analysis. p < 0.05 was defined as a significant difference, and all statistical analyses were performed by RevMan version 5.3.
Search results
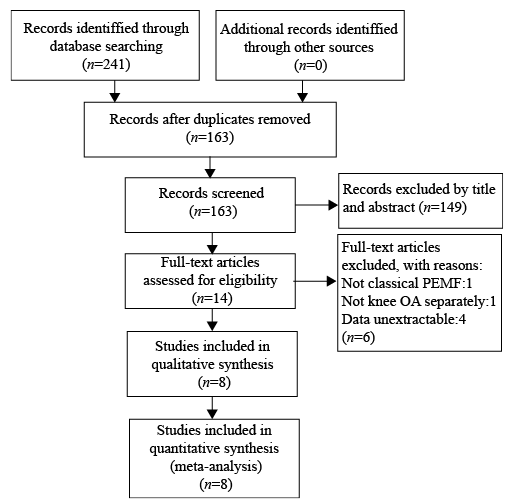
A total of 241 studies were retrieved through searching the electronic databases listed (Fig. 1). No additional records were identified from other sources. Seventy-eight duplicate studies were excluded initially, and a further 149 studies were excluded after reading the title and abstract. This left 14 studies that needed to be further screened by reading the full text. As a result, 6 studies were excluded due to unextractable data, non-classical PEMF therapy, or knee OA not reported separately. A final total of 8 studies was included in this meta-analysis (15–22).
Fig. 1. Study flow diagram of search results and study selection.
Study characteristics
The baseline characteristics, PEMF therapy parameters, and treatment regimen of the 8 included studies, with a total sample size of 421 patients, are shown in Table I. These studies were all randomized placebo-controlled trials involving patients of similar age, sex ratio, and body mass index, which were published between 1994 and 2016. There were some differences in the parameters and treatment regimen of PEMF therapy among all studies. In addition, 3 studies reported the outcome of pain using a VAS score, while 4 studies reported joint pain using a WOMAC score, as well as providing the outcomes of joint stiffness and physical function, and one other study used VAS score and WOMAC score together to report the outcomes.
Table I. Baseline characteristics, PEMF parameters and treatment regimen of included studies
Quality assessment
Randomization was unclear in one study, and allocation concealment was unclear in 5 studies. With regards to blindness, one study was unclear with regard to detection bias, while all the other studies showed low risk with regard to performance bias and detection bias. In addition, all studies showed low risk in terms of attribution bias and reporting bias, but were unclear for other bias. Overall quality assessment indicated that all included studies had a low or moderate risk of bias (Fig S11 and Fig. S21).
Meta-analysis
WOMAC total score. Four studies reported the WOMAC total score of 218 patients (Fig. 2A). Meta-analysis was performed using the fixed effects model due to the lack of heterogeneity among studies (χ2 = 1.14, df = 3, I2=0%, p = 0.77). Pooled results showed that there was no significant difference in WOMAC total score between the PEMF treatment group and the placebo group (WMD = −7.80, 95% CI −16.08 to 0.47, p = 0.06).
WOMAC pain score and VAS pain score. As shown in Fig. 2B and 2C, there were 5 studies with data from a total of 301 patients that were used to evaluate the WOMAC pain score through a fixed effects model for no significant heterogeneity (χ2 = 4.33, df = 4, I2 = 8%, p = 0.36); no significant effect on joint pain was observed in the PEMF treatment group (WMD = −1.06, 95% CI −2.30 to 0.17, p = 0.09). In addition, data from 5 studies, involving 233 patients, were used to analyse VAS pain score by random effects mode. The pooled results showed that the VAS pain score was not notably reduced in the PEMF treatment group compared with the placebo group (WMD = −0.88, 95% CI −2.06 to 0.31, p = 0.15) and also show significant heterogeneity (χ2 = 32.01, df=3, I2=91%, p < 0.00001).
WOMAC stiffness score. Analysis of the WOMAC stiffness score was achieved through 5 studies involving 301 patients. There was no significant difference in the pooled results between the PEMF treatment group and the placebo group, which demonstrated that PEMF therapy had no advantage in improving joint stiffness (WMD = −0.50, 95% CI −1.09 to 0.09, p = 0.1, Fig. 2D). In addition, a fixed effects mode was used, which indicated no heterogeneity (χ2 = 2.17, df = 4, I2 = 0%, p = 0.7, Fig. 2D).
WOMAC physical function score. WOMAC physical function score was reported by 5 studies involving 301 patients. Pooled results showed that the WOMAC function score in the PEMF treatment group was significantly lower than in the placebo group (WMD = −5.28, 95% CI −9.45 to −1.11, p = 0.01, Fig. 2E). Since no significant heterogeneity was found (χ2 = 0.86, df = 4, I2 = 0%, p = 0.93, Fig. 2E), the fixed effects model was used to perform this analysis.
Fig. 2. Forest plots comparing pulsed electromagnetic field (PEMF) therapy with placebo for patients with knee osteoarthritis (OA). (A) Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) total score. (B) WOMAC pain score. (C) Visual analogue scale (VAS) pain score. (D) WOMAC stiffness score. (E) WOMAC physical function score.
Sensitivity analysis
Analysis of WOMAC total score, WOMAC pain score, WOMAC stiffness score and WOMAC physical function score showed no significant statistical heterogeneity; thus it was not necessary to perform sensitivity analysis for these parameters. Nevertheless, there was a significant heterogeneity in the analysis of VAS pain score. As a result, significant heterogeneity remained after sensitivity analysis was conducted by eliminating each study individually, but this heterogeneity was notably reduced if the study published by Ay & Evcik (18) was omitted (χ2 = 4.25, df = 2, I2 = 53%, p = 0.12, Fig. 3). Moreover, pooled results showed that there was also a significant difference between the PEMF treatment group and the placebo group if the study published by Ay & Evcik (18) was omitted (WMD = −1.47, 95% CI −2.14 to −0.80, p < 0.0001, Fig. 3).
Fig. 3. Forest plot of visual analogue scale (VAS) Pain score after exclusion of data from Ay & Evcik (18).
Knee OA is currently one of the most common
chronic joint diseases and often causes joint pain, joint dysfunction, and even disability. PEMF therapy is an accepted physical therapy and is an effective method for the treatment of various pathological conditions and diseases, especially in trauma, orthopaedics and rheumatology (23). Although PEMF therapy is not recommended for treating OA by the American College of Rheumatology due to the lack of clinical studies, it has become popular among patients with knee OA in recent years (18). In the past 2 decades, PEMF therapy has been used more and more frequently for OA (24). Moreover, current clinical trials have yielded different results regarding the efficacy of PEMF therapy in the treatment of knee OA, including some systematic reviews (8–12). Consequently, it is necessary for us to verify the efficacy of PEMF therapy in the management of joint pain, joint stiffness, and physical function for patients with knee OA. In this study, an effect on improving physical function was observed, while PEMF therapy showed no advantage in the reduction of WOMAC pain score, VAS pain score or WOMAC stiffness score.
Joint pain and stiffness are the most common and prominent symptoms of knee OA, and the guidelines developed by the OA Research Society International recommend that improving pain and stiffness should be the primary goal of treatment (25). However, previous systematic reviews have shown significant controversy over whether PEMF therapy has any effect on improving pain and stiffness in knee OA. Only one review clearly supports its ability to relieve pain (11). Furthermore, studies often neglected to analyse the effect of PEMF therapy on join stiffness. In addition, we found that previous studies included some low-quality non-randomized controlled trials and the pooled results included other physical therapies, such as pulsed short-wave (9, 11, 12). Unlike previous systematic reviews, only randomized placebo-controlled trials concerning classic PEMF therapy, as well as 3 newly published RCTs with high-quality methodology (15–17), were included in this analysis, and the results confirmed that PEMF therapy had no advantage in improving patients’ joint pain or joint stiffness over a period of approximately 1 month. A possible explanation for this is that subchondral bone, periosteum, synovium, ligament, and joint capsule are rich in innervation, thus the nerve endings are the origin of pain caused by OA nociceptive stimulation (26, 37). However, studies have shown that PEMF therapy has an effect on articular cartilage regeneration and repair, but since there are no nerves or blood vessels in cartilage, cartilage injury does not directly cause pain and, consequently, there is no significant improvement in pain with PEMF therapy (28–30).
In the meta-analysis of VAS pain score, significant heterogeneity was found among the included studies. This significant heterogeneity remained after sensitivity analysis was conducted by eliminating each study individually, although this heterogeneity was notably reduced if the study published by Ay & Evcik (18) was eliminated. Nevertheless, there was insufficient evidence to suggest that this study had methodological deficiencies or was of poor quality, thus it was not excluded, although this may have resulted in an influence on the pooled result of VAS pain score. A possible explanation for this is that there may be differences in the frequency, intensity, or treatment regimen of PEMF therapy among these included trials. At present, due to the limited clinical research data on the application of this treatment to OA, there is no consensus on standardized parameters of PEMF therapy, such as frequency, intensity, pulse length, or pulse waveform for the safest and most effective treatment, and more clinical research data is needed (31, 32).
Previously, there have been 3 systematic reviews that analysed whether PEMF therapy can improve physical function for patients with knee OA. Among them, one review (12) concluded that PEMF therapy had no significant effect on physical function, while the other 2 (9, 10) showed that PEMF therapy was beneficial in improving physical function. A possible explanation for this discrepancy is that 2 clinical studies involved classical PEMF therapy, while another 2 clinical studies used typical pulsed short-wave. These were all included without subgroup analysis in the previous systematic review, which drew the opposite conclusion (12). In this meta-analysis of physical function, the observed WMD was –5.28, and reached above minimal clinically important differences, suggesting that PEMF therapy may improve physical function (33). Possible factors for this are that PEMF therapy can elicit strong effects on the vitality and proliferation of human chondrocytes and on the synthesis of chondrocyte extracellular matrix in vitro (34–36). Despite bone and cartilage metabolism promoted by short-term PEMF therapy, the treatment may not lead directly to improvement in local joint symptoms; it may reduce the clinical global impression of severity and improve patients’ global impression, which may be related to the improvement in activities of daily living measured by the WOMAC physical function subscale.
There are still some limitations to the current study. Firstly, only 8 RCTs were included, resulting in a relatively small sample effect. Secondly, only studies published in English were included. Finally, there was significant heterogeneity in the meta-analysis of VAS pain score, possibly due to variations in the frequency, intensity, treatment regimen, and duration of PEMF therapy among the included trials. In addition, since the VAS is a self-report measure assessing pain intensity, it may result in relatively strict or loose ratings among included studies. Although the PRISMA guidelines and Cochrane Handbook for Systematic Reviews of Interventions were used to assess the included studies to ensure reliable and verifiable results, more RCTs are needed to provide further validation.
In conclusion, this meta-analysis showed that, despite having no advantage in the management of pain and stiffness, PEMF therapy is beneficial for improving clinical symptoms such as physical function in patients with knee OA. This means that PEMF therapy may be a useful and economic adjuvant treatment for non-surgical management of knee OA. Further research is needed to determine the optimal frequency, intensity, treatment regimen and duration of PEMF therapy.
This work was supported by the National Natural Science Foundation of China (31870961), the International Cooperation Project of Sichuan Provincial Science and Technology Department (2015HH0049), the Sino-German Center for Research Promotion (GZ1219), and the National Clinical Research Center for Geriatrics, West China Hospital, Sichuan University (Z2018A11). The authors would like to thank International Science Editing Co. for editing the language.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize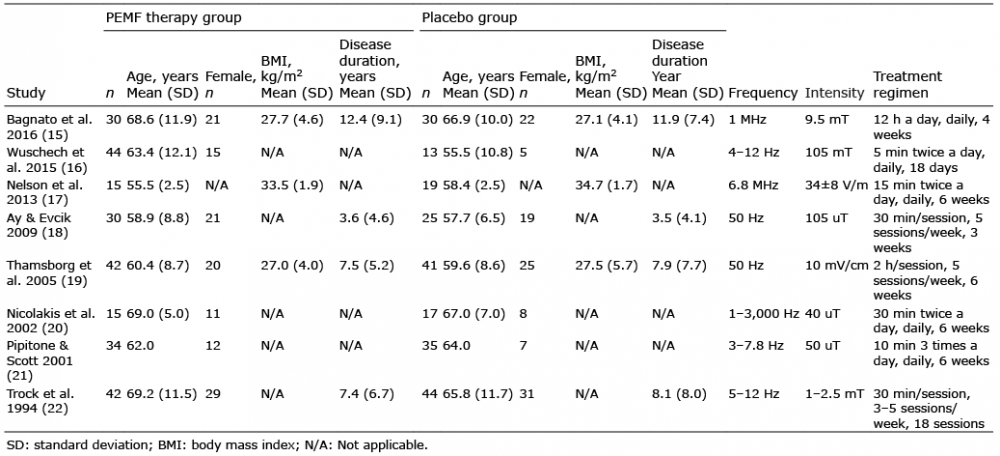 Click to show fullsize
Click to show fullsize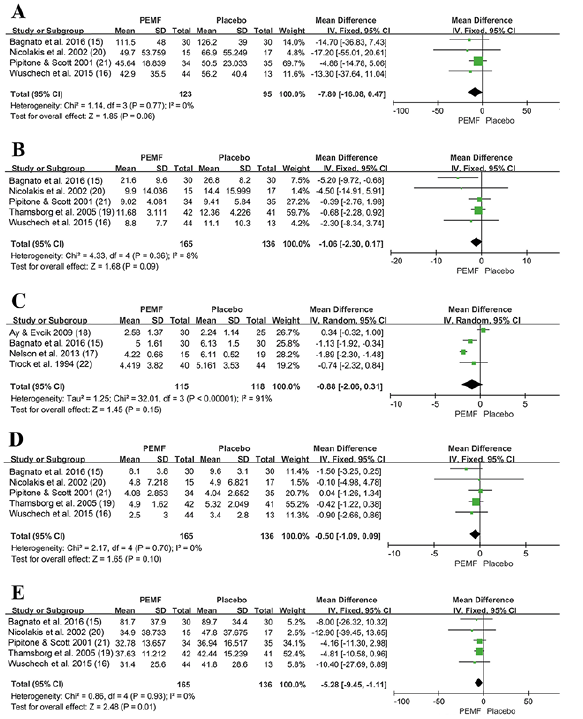 Click to show fullsize
Click to show fullsize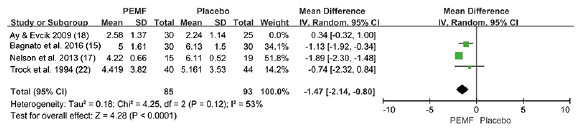 Click to show fullsize
Click to show fullsize