
From the Orthopaedic Research Institute, Bournemouth University, 6th Floor, Executive Business Centre, Bournemouth, UK
Objective: This systematic review aimed to assess the clinical impact of neuromuscular electrical stimulation as a treatment modality for patients with oedema.
Data sources and study selection: PubMed was searched up to July 2018 for randomized and non-randomized clinical trials comparing neuromuscular electrical stimulation vs no stimulation following the formation of oedema. A modified Downs and Black checklist was used to evaluate the quality of the evidence.
Data synthesis: Initial searches yielded 150 results. Removal of duplicates reduced this number to 97 results. Seventy-five studies were excluded following a review of titles and abstracts. Full-text screening eliminated 15 studies. A final total of 7 studies met the inclusion criteria. Six studies supported the use of neuromuscular electrical stimulation for oedema reduction, and one study did not find an effect, but reported inter-group variance.
Conclusion: The results of this systematic review support the use of neuromuscular electrical stimulation for ameliorating the abnormal accumulation of interstitial fluid, which is clinically shown as oedema. Neuromuscular electrical stimulation is effective in a number of rehabilitation settings and patient groups, for treatment of both upper and lower limb oedema. However, further trials are needed to reinforce these findings.
Key words: rehabilitation; physical therapy modalities; electrical stimulation; oedema.
Accepted Jan 29, 2019; Epub ahead of print Feb 19, 2019
J Rehabil Med 2019; 51: 00–00
Correspondence address: Thomas Wainwright, Orthopaedic Research Institute, Bournemouth University, Executive Business Centre, 89 Holdenhurst Road, Bournemouth, BH8 8EB UK. E-mail: twainwright@bournemouth.ac.uk
The aim of this review was to evaluate the effectiveness of neuromuscular electrical stimulation for treating oedema, which is the abnormal build up of interstitial fluid in the body. A web-based search was performed to evaluate clinical trials to assess the effect of neuromuscular stimulation within all medical populations. Six studies were found that support the use of neuromuscular electrical stimulation for reducing oedema and one study that did not. These results suggest that neuromuscular electrical stimulation may be useful for treating oedema in both upper and lower limbs. However, the findings are limited and further research is needed.
Oedema may occur following a wide range of musculoskeletal injuries and in other clinical settings (1). Following injury an abnormal build-up of interstitial fluid in the body can create swelling in the affected tissue, causing pain and dysfunction (2). Oedema may be generalized, meaning it occurs in multiple organs across the body; however, most types of oedema are specific to a single organ. Treatment is individual to the type of oedema, and in some cases the swelling resolves independently. Often, however, the treatment of oedema following injury can be challenging. Treatment of oedema aims to correct the cause of the fluid accumulation; however, it can be difficult for patients to incorporate traditional management strategies (such as rest, ice and elevation) into their daily routines. Voluntary activation contractions can help to improve circulation by stimulating lymphatic flow; however, they are not always possible for a patient presenting with musculoskeletal injuries and the use of compression devices are not always feasible for patients with co-morbidities (3).
As well as activation of muscles via the bodies’ nervous system, muscles can also be contracted by the application of an external electrical stimulation. Electro-physical agents have a long-established place in therapy practice and the emphasis of this mode of treatment has seen significant change over time (4). Neuromuscular electrical stimulation (NMES) is the elicitation of an involuntary muscle contraction using electrical impulses (5). It is proposed that the contraction of muscles causes intermittent venous compression and, because of the orientation of the venous valves, blood is forced from the periphery, through the veins toward the heart. The involuntary muscular contraction lowers the mean venous pressure and serves as an auxiliary pump to assist venous return and lymphatic flow, which may reduce oedema. Therefore, NMES may affect the lymph drainage or the interstitial hydrostatic pressure components of fluid exchange, which can affect oedema formation and resolution.
Devices delivering NMES are wide ranging, and some may cause discomfort, therefore such devices are not always utilized within a clinical setting. In addition, whilst increased blood flow is reported to decrease oedema; the outcomes from many individual NMES and oedema studies remain inconclusive. Thus, the current systematic review assessed studies that evaluated NMES devices for patients presenting with oedema. The results of this review could help the development of rehabilitation programmes focused on helping patients with oedema.
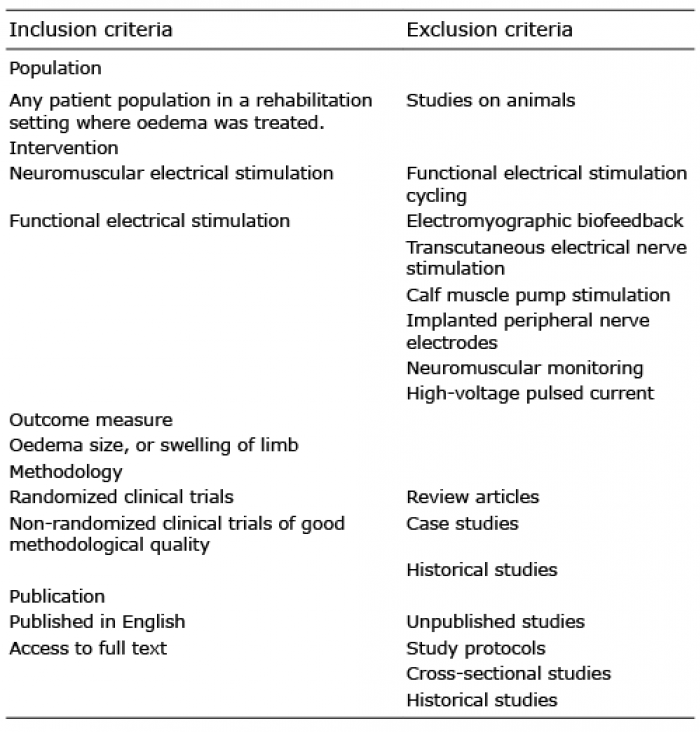
A systematic review was conducted to examine current published evidence regarding the use of NMES for treatment of oedema. The methodology of this review was developed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (www.prismastatement.org/PRISMAStatement) (6). A computer-based search was completed in July 2018, and the electronic database sourced was PubMed (https://www.ncbi.nlm.nih.gov/pubmed/). The search reviewed all fields of the available literature, published in the English language (or those for which a translation was available) to the earliest record on file. A secondary search was also conducted, whereby the reference lists of articles, review papers and textbooks were scanned for additional papers. There are 2 categories of this type of stimulation, one type of device (named NMES) is used to treat muscle atrophy when the muscle is in a resting state, and the other, named functional electrical stimulation (FES), used to enhance functionality of neurologically impaired individuals. Therefore, FES search terms were also included. Other devices delivering electrical stimulation were excluded. Studies were considered eligible for inclusion within the synthesis if they met the specified inclusion and exclusion criteria listed in Table I.
Table I. Inclusion and exclusion criteria
In order to capture studies published across all rehabilitation disciplines; a broad search strategy was adopted (Table II). All titles and abstracts were initially checked for relevance and duplicates by 2 independent reviewers (LB and TW). The remaining results then underwent a full-text appraisal to ensure that the studies were of good methodological quality, that their findings were significant, that they were evaluating a NMES device, and that they were examining the effectiveness of the device to treat oedema. Study design was assessed using the PICO (Patient, Intervention, Comparison and Outcome) framework to ensure the study was relevant (7). Secondary searching was also undertaken, whereby reference lists of the selected articles were reviewed for additional studies not identified in the primary search.
Table II. Search strategy
The Downs and Black checklist (8) was used to assess the risk of bias within the studies sourced. The 27-item methodological quality checklist has been shown to have good intra-rater (r. 0.88) and inter-rater (r. 0.75) reliability (8) It has been used previously in systematic reviews with various study designs, and has also been amended to suit the structure of the review in which it was utilized (9, 10). Similarly, a modified version of the Downs and Black checklist was employed with the items that were not suitable to the review removed (items 5, 8, 14, 15, 21–27). The adapted version of the tool consisted of 16 items (Appendix 1), including items 1–4, 6, 7, 9–13 and 16–20 from the original list, with a maximum possible score of 16. The higher scores indicated superior quality. The first 8 items on the scale relate to reporting and include aims, outcome measures and results. Items 11–13 relate to external validity and consider whether results from the study can be generalized to a wider population. Items 16–20 relate to internal validity. Risk of bias was assessed by 2 independent assessors (LB and TI) and any discrepancies were resolved through discussion.
All of the studies within this review compared pre- and post-intervention values for oedema size. The majority of the data were not normally distributed and, therefore, non-parametric testing was used to compare means and variation. Six studies also compared between-group changes when electrical stimulation was compared with the following factors: no stimulation, placebo stimulation, compression stockings, limb elevation, and a whirlpool bath.
A flow diagram of the study identification process is shown in Fig. 1 and a summary of the studies sourced is shown in Table III. Seven studies assessed the role of NMES for reducing oedema (11–17). Oedema size, or swelling, was a primary outcome measure in all the included studies.
Fig. 1. PRISMA flow diagram.
Appendix 2 presents the results of the methodological assessment. Quality assessment scores ranged from 56% to 88% (mean =77%). Reporting within the studies was generally consistent. Six studies scored the maximum attainable score for clearly describing the study aims and objectives (12–17). External validity was low scoring, generally due to study participants being selected patients, small study size and a lack of description of the facility in which the study was undertaken. Internal validity was generally high scoring, with 5 studies scoring maximum marks (12, 14–17). Marks were lost from 2 studies (11, 13) due to the absence of reported patient compliance (item 19).
Lower limb oedema. Five studies assessed the use of NMES for reducing oedema in the lower limbs in a variety of rehabilitation settings, detailed thereafter (11–15). Largely, this evidence demonstrates that NMES can reduce oedema, although 1 study found no effect (15); however, the authors attribute this to inter-group variance at baseline. Other benefits of NMES within current literature include improved quality of life and reduced pain (11).
Chronic venous oedema/lymphedema. A study by Bogachev et al. (11) on patients (n = 30, limbs = 32) with chronic evening venous oedema found that total or partial reduction of oedema occurred in 93.8% of limbs with the use of NMES device. The circumference of the lower leg diminished by 20.3 mm (p < 0.001), pain reduced and quality of life improved.
A more recent randomized clinical trial (RCT) by Ravikumar et al. (12) assessed the effect of footplate NMES in treating patients with venous disease (n = 22). Patients were treated with either NMES or a sham device daily for 30 min over a 6-week period. There was a significant difference in the percentage change in the femoral vein flow parameters from baseline between the treatment group and the sham group whilst using the device. Limb volume was observed to increase significantly in the sham group; however, this was prevented in the treatment group, demonstrating that NMES can have a preventative role in orthostatic limb oedema.
A pilot interventional crossover study (n = 10) by Wou et al. (13) compared 2 NMES devices and compression stockings for reducing lower limb occupational oedema in healthy individuals. Without an intervention, leg volume increased by a median of 41 ml. All devices were well tolerated and reduced leg swelling; however, there was no significant effect of NMES and the compression stockings were the only device that created a significant reduction in swelling.
Ankle sprain/fracture. A crossover, counterbalance trial was completed by Man et al. (14) to evaluate the effect of NMES on foot and ankle volume during 30 min of standing (n = 20). A group of healthy patients completed 30 min of standing with and without NMES applied to the gastrocnemius and the tibialis anterior of the dominant leg, on 2 separate occasions. Mean volume changes from pre-test to post-test with NMES and without NMES were significantly different (p = 0.001). The authors concluded that the activation of the musculo-venous pump by a NMES-induced muscle contraction may reduce swelling in the lower limbs of patients by increasing venous return, reducing venous stasis, increasing lymph flow, and increasing hydrostatic pressure, which would reduce capillary filtration and assist fluid absorption.
A later study by Man and colleagues (15) randomized 34 patients with an ankle sprain into either: (i) a group with NMES applied to the lower leg muscles; (ii) a group with sub-motor electrical stimulation applied to the lower leg muscles; or (iii) a group with electrodes set up on the lower legs with no electrical stimulation applied (sham group). There were no statistically significant differences between groups for ankle-foot volume and self-assessed ankle function. Ankle girth was significantly improved from session 1 to 3 with the application of NMES; however, the authors note that this result may be confounded due to inter-group variance. A statistically significant difference in ankle girth measurements was recorded among the 3 groups at baseline in addition to an unexpected difference in subjects’ height.
Upper limb oedema. Similar to the results of studies assessing NMES for reducing lower limb oedema, there are 2 studies that support the feasibility and effectiveness of NMES for reducing upper limb oedema (16–17). Other benefits found were improvements in pain, function, range of motion and strength.
Complex regional pain syndrome. A study by Devrimsel et al. (16) compared the effect of whirlpool baths and NMES on complex regional pain syndrome (n = 60). The authors found significant improvements in pain, oedema, range of motion, fingertip-to-distal palmer crease distance, hand grip strength and pinch strength in both groups. The efficacy of the whirlpool bath treatment was considered more effective due to statistically significantly better improvements in outcomes; however, both treatments were regarded as effective in the treatment of complex regional pain syndrome and the reduction of oedema.
Cerebrovascular accident patients. A small study (n = 8) by Faghri (17) used a repeated measure design to compare the use of NMES to limb elevation on hand oedema patients following a cerebrovascular accident. Thirty minutes of NMES of the finger and wrist flexors and extensors was compared with the effects of 30 min of limb elevation alone. The author found both treatments to be significantly effective in improving volume and girth of the arm and hand, and NMES was more effective for the reduction of hand oedema than limb elevation within their sample, although no actual significance values are reported.
In medical research, there is an aim to establish the lowest dose of medication that is effective in producing a clinical benefit with the fewest side-effects possible. The discomfort associated with stimulus may reduce patient acceptance or compliance with NMES as a therapy (18); therefore, it is important that there is a balance between effectiveness and comfort, in order to promote patient compliance. Technical developments of NMES devices have improved patient tolerance by allowing effective stimulation with a lower current density and pulse duration (18). This may be important when comparing the NMES devices that stimulate the motor nerve in comparison with those that stimulate the motor point. Neural stimulation requires lower current intensity for the same level of contraction, and thus devices may be better tolerated by patients. The use of NMES as a rehabilitative device was reported to be feasible and safe in all studies, with no recorded harmful side-effects or adverse events.
Within the studies sourced, there is a wide variation in the parameters utilized, but, in general, NMES was applied for periods of 20–30 min. Stimulation occurred once a day in 5 studies (12–15, 17), 5 times per week in one study (16), and reduced from 3 times, to 2 times, to once per month, in 1 study (11). The majority of studies support the use of a higher dose for a short period of time, as opposed to a low dose for a long period of time. It is important to establish the maximum effect for the lowest intensity of stimulation so that the treatment is comfortable for the patient. The frequency of application and number of repetitions varied between authors, with the range between 1 and 125 Hz. A high pulse frequency setting is more commonly used for the treatment of pain, and a lower frequency may be advantageous for swelling reduction. Duty cycle describes the actual on and off time of an NMES programme, and commonly, full amplitude “on” period, which is one-third of the stimulus “off” time will avoid rapid muscle fatigue. By creating non-fatiguing muscle contractions, NMES can dilate blood vessels and help to increase blood flow. Rehabilitation timing was also non-consistent between studies, with treatment commencing at different times in each intervention. The percentage change in oedema is shown in Table IV; however, variance in methodologies prevents detailed a comparison being made.
Table IV. Percentage change in oedema
Although the variation in patient groups adds generality to the effectiveness of NMES for reducing oedema, it is difficult to compare methodologies from such a variety of clinical rehabilitation settings. Increasing the number of well-conducted, adequately powered RCTs with a standardized methodology would enable practitioners to confidently prescribe NMES as a modality for decreasing oedema.
In addition, within the study results, there is a wide variation within the equipment used to deliver NMES to patients. Therefore, it is not easy to advocate the use of one NMES device over the other, as there are not enough published studies to allow comparative analysis. The majority of studies utilized NMES devices that were applied to the skin surface; however, 2 studies utilized foot-plate NMES (Revitive XI) (12, 13), which is another methodological variance that prevents generality of results. The Revitive IX device has a rocker device that elicits active and repetitive plantar flexion and dorsiflexion and so whether the effect is due to limb movement or purely NMES cannot be defined. Active plantar flexion and dorsiflexion are rehabilitative exercises prescribed to increase lower limb blood flow. Thus, reduction in oedema following treatment with the Revitive XI device may be attributable to the NMES, the active mobility exercises or a combination of both treatments. This has relevance to clinical populations where movement is prohibited.
In order to draw a clinically significant conclusion, it is important that studies are appropriately powered (19). Out of the 7 studies sourced, 2 had fewer than 12 study participants (13, 17). Although these small studies present meaningful results and can assess feasibility, their clinical importance is compromised due to their underpowered methodologies. Across all clinical settings, there is a lack of adequately powered RCTs investigating the effect of NMES for oedema.
Six studies demonstrated that NMES devices are effective in the treatment or management of oedema, with no reported adverse events. There is some evidence, outlined above, to the effect that NMES activation of the venous pumps in the extremities is effective in reducing oedema in those extremities, in a variety of different patient groups. One study did not find a significant clinical effect of NMES in reducing oedema; however, the authors recognize that this result may be confounded by inter-group variance (15). Appropriately powered clinical trials are required with oedema as a primary outcome and a focus on returning to function and recovery. Future studies should also aim to establish the most effective mode of delivery and dose for NMES to facilitate recovery from different diseases, procedures or anatomical locations.
Thomas Wainwright reports personal non-related consultancy fees from ZimmerBiomet, Sky Medical Technology, The Technology Partnership, Medacta, and Medtronic. He is a Director and Shareholder in Healthdecoded Ltd. He has received institutional research grants from Dorset Local Enterprise Partnership, Wessex Academic Health Science Network, OSSIM Technologies, and The Technology Partnership outside the submitted work.
Appendix 1. Modified Downs and Black Checklist


 Click to show fullsize
Click to show fullsize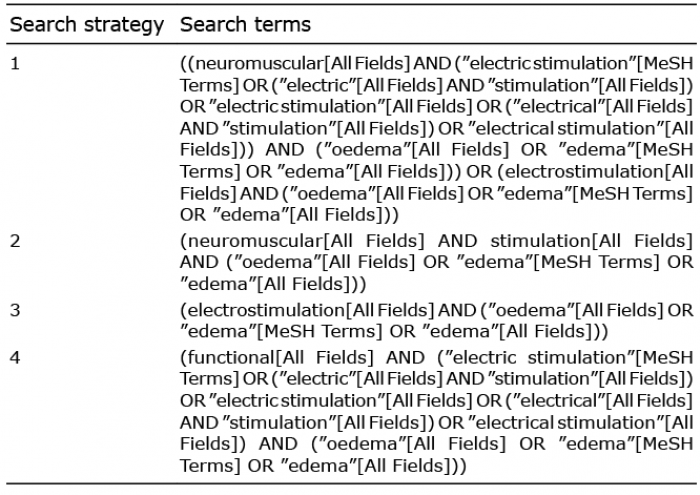 Click to show fullsize
Click to show fullsize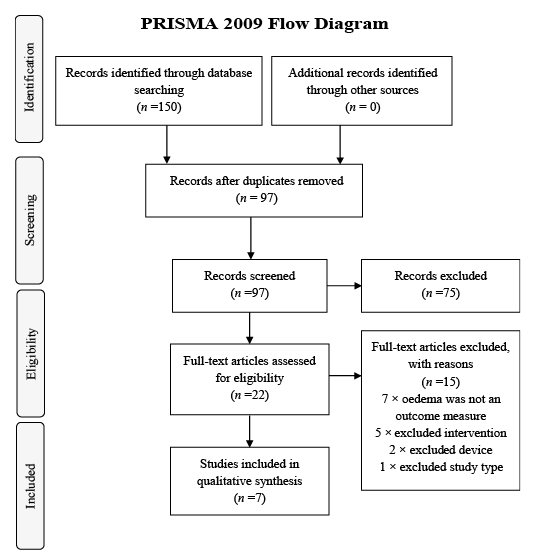 Click to show fullsize
Click to show fullsize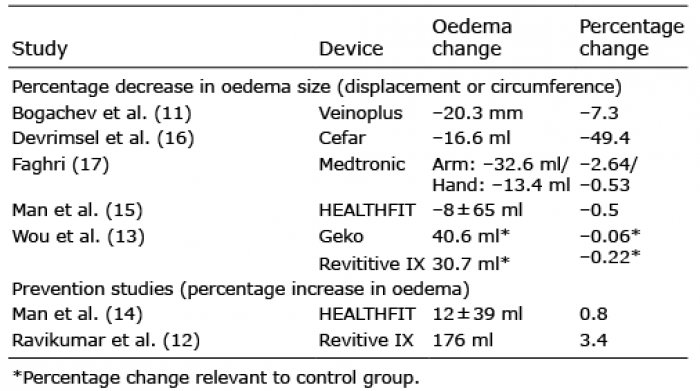 Click to show fullsize
Click to show fullsize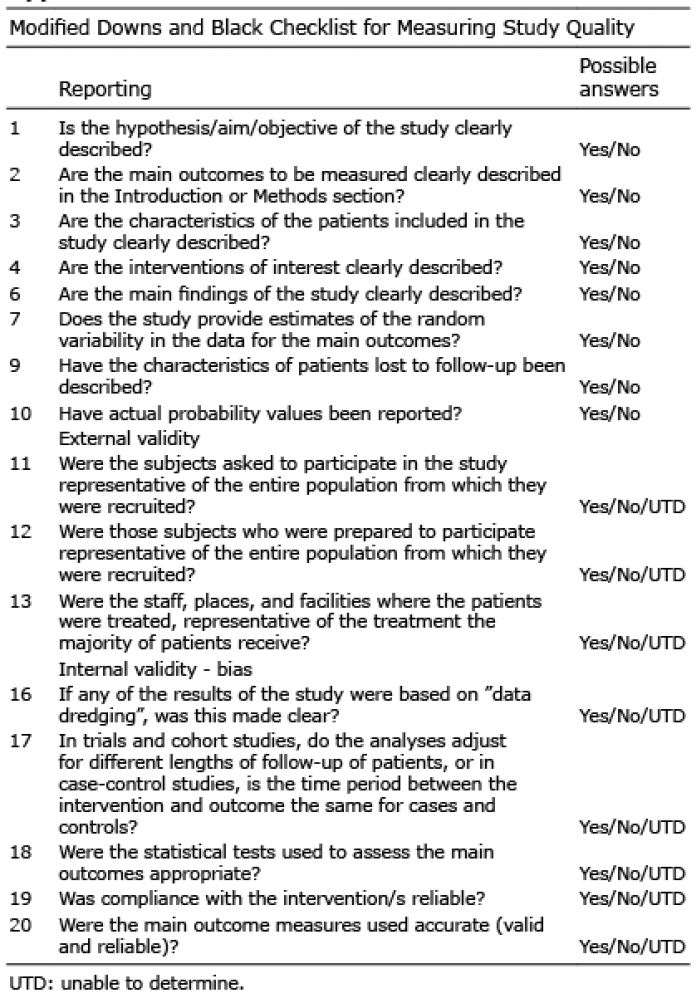 Click to show fullsize
Click to show fullsize