
From the 1Department of Women’s and Children’s Health, Neuropediatric Unit, Karolinska Institutet, Stockholm, 2Centre for Clinical Research Sörmland, Uppsala University, Eskilstuna and 3Karolinska University Hospital, Stockholm, Sweden
Objectives: To describe social outcomes for young adults with cerebral palsy, and to explore associations of social outcomes with their classification levels within the Gross Motor Function, Manual Ability and Communication Function Classification Systems, and with the presence of intellectual disability.
Design: A cross-sectional study with a population-based inclusion approach at a neuropaediatric referral centre in Sweden.
Subjects: Sixty-one young adults with cerebral palsy, age 20–22 years.
Methods: Physical examination and questionnaires on social outcomes including living arrangements, relationships, occupation, personal finances, extent of family support with personal care.
Results: Twenty percent of the young adults with cerebral palsy had moved out of the parental home. Forty-three percent were dependent on family support for basic activities of daily living. Seventy-nine percent of those without intellectual disability were employed or studying. The Communication Function Classification Systems, and presence of intellectual disability, demonstrated associations with most social outcomes, followed in significance by Manual Ability Classification System.
Conclusion: In this study young adults with cerebral palsy to a high extent lived in the parental home, and more often without employment, compared with their peers. Many were dependent on parental support, financially, and with activities of daily living. Intellectual disability and communication function were important determinants of social participation. Interventions aimed at alleviating the impact of these particular disabilities should be prioritized.
Key words: cerebral palsy; young adult; social participation; classification; communication disorder.
Accepted Dec 19, 2018; Epub ahead of print Feb 27, 2019
J Rehabil Med 2019; 51: 167–174
Correspondence address: Dan N. O. Jacobson, Neuropediatric Unit, Astrid Lindgren’s Children’s Hospital, Karolinska University Hospital, 171 76 Stockholm, Sweden. E-mail: dan.jacobson@ki.se
*This study was performed at the Neuropediatric Unit, Astrid Lindgren’s Children’s Hospital, Karolinska University Hospital, Stockholm, Sweden. Parts of the material were presented as a poster at the 28th Annual Meeting of the European Academy of Childhood Disability, Stockholm, Sweden, in June 2016.
A representative group of young adults with cerebral palsy were studied in order to learn more about social issues, such as living arrangements, employment and relationship status. It was found that, while some young adults were well-established in occupations and relationships, many remained highly dependent on their parental families and their social situation was reduced compared with their peers. Furthermore, low-functioning communication level and intellectual disability were the 2 most important risk factors for having a sub-optimal social situation. This suggests that priority should be given to interventions aimed at alleviating the impact of these particular risk factors.
Cerebral palsy (CP) is the most common cause of childhood onset life-long physical disability and is present in an estimated 17 million individuals worldwide; most having a lifespan similar to the general population (1, 2). Consequently there is a large population of adults with CP. Research has traditionally focused on the childhood years and little is known about the health and social situation of adults with CP. Michelsen and colleagues showed that, in 2006, 55% of Danish adults with CP (mean age 32 years) were unemployed, did not co-habit with a partner, and did not have children, compared with 4% of the control population. This situation appeared unchanged compared with 3 decades earlier (3). A Swedish postal survey of adults with CP (20–58 years of age) found that most lived in a single household and 24% worked full time (4). Population-based surveillance programmes for adults, such as Cerebral Palsy Follow-Up Program Adult, are emerging and have reported results from a population of young adults in southern Sweden in the age range 18–23 years (5). They found that 20% of subjects were employed, but most still lived at home (5). Verhoef and colleagues in the Netherlands reported employment rates of 49% in 20–24 year-olds with spastic CP and average intellect (6).
Social well-being is an integral part of the World Health Organization’s (WHO) definition of health (7). Further, the WHO’s International Classification of Functioning, Disability and Health (ICF) offers possibilities to describe functioning and health from various perspectives (8). The ICF shifts the focus from cause to impact on functioning, which covers body functions/structures, activity and participation, and the contextual factors in the individual’s life (8). From the perspective of young adults with CP, interviews using qualitative methods have shown that living arrangements, occupation, issues with personal care and inter-personal relationships are amongst the more important issues to address; these span the components of activity, participation and contextual factors (9, 10).
Given the heterogeneity of CP, several classification systems have been developed to describe level of functioning; the Gross Motor Function Classification, Extended and Revised (GMFCS-ER), the Manual Ability Classification System (MACS) and the Communication Function Classification System (CFCS) (11–13). These classification systems share similar properties, with 5-level ordinal scales classifying function ranging from mild disability (Level I) to severe disability (Level V). The systems are commonly used for analysing sub-groups. The GMFCS and the MACS are thought to be relatively stable over time and have been used for prognostic purposes (14, 15). Intellectual disability is also of central importance, as it has a large impact on social life trajectories and is present in approximately half of individuals with CP (16, 17).
Young adulthood involves transitioning to independence from the parental family, and as such, this period offers possibilities to explore key factors that promote or disrupt a healthy and well-integrated life.
Thus, the aim of this study was to describe a set of social outcomes in young adults with CP, using a population-based approach. The second aim was to explore associations between the social outcomes with the classification systems GMFCS, MACS, CFCS, and intellectual disability.
A cross-sectional study performed with population-based inclusion approach and collection of data through direct contact.
In 2011, a hospital-based registry was created on behalf of Stockholm County Council to evaluate the effect of a new care programme for youth and children with CP. All individuals born in 1992–95 who had visited any of the 3 neuropaediatric clinics or the paediatric orthopaedic clinic serving all of Stockholm, and received an International Statistical Classification of Diseases and Related Health Problems Tenth Revision (ICD-10) diagnosis of CP within the last 5 years were identified. In Sweden, all children with CP are expected to have regular follow-up at the neuropaediatric clinic at least biannually. This registry was the basis of the study population.
Beginning in September 2013, letters of invitation were sent out to publicly available addresses linked to the personal identity numbers (18). Those who expressed interest were contacted with additional information and invited to the clinic. The recruitment process was scheduled so that the individual would be in the range 20–22 years of age at the time of data collection. If no contact could be established despite letters and telephone attempts, the individual was considered “Unable to reach”. After providing informed consent, the responders were scheduled for structured interviewing, questionnaires and clinical assessment at Astrid Lindgren’s Children’s Hospital, Stockholm as a part of a broader data collection. For individuals with intellectual disability and/or significantly impaired communication, the legal representative of the young adult (most often a parent) provided informed consent and acted as his/her proxy.
Telephone and/or Skype was used for those unable to attend the clinic (e.g. because of university studies elsewhere). In these cases, there was no physical examination and health data were obtained from records of recent clinical examinations. Telephone interviews were performed with the proxy if the individual was unable to attend the clinic and had intellectual disability and/or significantly impaired communication.
All sessions were conducted by the same medical doctor investigator (DJ), together with 1 of 2 physiotherapists with extensive experience of CP (KL, EH), and took 1 full afternoon per participant.
Data collection was completed in August 2016.
The social outcomes of interest were identified in a multimodal approach. The first steps were reviews of the literature on the topic and review of the outcomes used in previous studies. Special emphasis was on studies with patient perspectives, which aided in selecting outcomes of particular interest for further analysis (9, 10). Topics addressed by adolescents and caretakers in the author’s clinical practice were also considered. Lastly, voluntary pilot participants (young adults with CP known to the authors) underwent the structured interview and gave qualitative feedback on the validity of the outcomes and the categorization of the items. The social outcomes identified in this manner were living arrangements, occupation, personal finances, personal care (in this context as the extent of family support with activities of daily living (ADL)), and relationships; both as intimate relationships and friendships. Details on personal assistance were also identified as important in this process, and were included for descriptive purposes. The responses on the outcomes were grouped into categories determined, in the multimodal approach, to be meaningful both clinically and for the individual.
Data on socioeconomic background included country of birth, parental level of education and parental social status.
The clinical subtype of CP was defined, and everyday functioning classified within GMFCS-E&R; describing gross motor functional level, MACS; describing manual ability level, and CFCS; describing functional level of sending and receiving communication (11–13). In accordance with the CFCS description, all methods of communication (including usage of augmented and alternative communication (AAC)) were taken into account in the assessment (11). Present or earlier enrollment in schools for individuals with intellectual disability was used as a marker of intellectual disability. In Sweden, only those with an intelligence quotient (IQ) ≤ 70 are eligible for such schools.
In addition, as preliminary analyses following data collection revealed associations with the CFCS on important outcomes, an add-on data collection focusing on communication by individuals with CFCS levels III–V was then designed. The proxies of these individuals (incidentally always a parent) were contacted and additional data were collected, thereby ascertaining the usage and impact of AAC and the extent to which communication function had been evaluated. In particular, parents were requested to evaluate whether AAC use had resulted in improvement of communication function equalling a shift in level within the CFCS, compared with when AAC was not used.
The study was pre-approved by the Stockholm Regional Ethical Review Board (No. 2013/544-31/2).
Data were analysed in Stata IC 14 for Mac. Descriptive data are presented as frequency and proportion or median and range as appropriate. The descriptive data are presented for the total sample, as well as grouped by level within the GMFCS, MACS, CFCS, and by presence of intellectual disability. The subgrouping was done to increase interpretability of the results given the large variation of disability in CP. The 5 levels within the GMFCS, MACS and CFCS were dichotomized as levels I–II or levels III–V, to enable clinically meaningful presentation given the sample size.
In the analysis of associations, the outcomes of particular interest were further grouped into binary yes/no categories, as “moved away from parental home”, “experience of intimate relationships”, “in regular employment or attending higher education”’, “independent personal finances”, and, as the question on friendships that appeared most reliable during data collection; “socializes with friends, outside home, including on evenings”. These binary yes/no items were analysed for associations with the GMFCS, MACS, CFCS (dichotomized as previously described) and presence of intellectual disability, with crude odds ratios calculated from 2 × 2 tables. Adjusted odds ratios were obtained by controlling for the presence of intellectual disability on each association separately, using logistic regression modelling (Stata IC 14).
The findings of the added data collection on communication function were prepared descriptively.
There were no missing data due to the data gathering approach used.
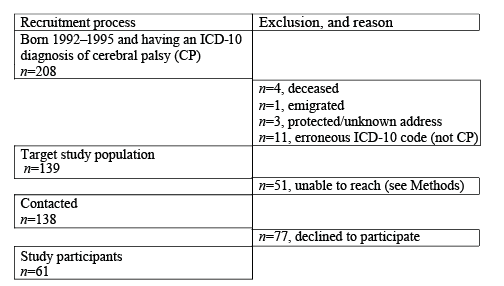
Sixty-one young adults, i.e. 44% of those who could be reached, and 32% of the entire target study population consented to participate (Fig. 1). There was no prior data collection on the target study population, and Swedish legislation prohibits access to patient charts without consent, thus making analysis of non-participants restricted to age (no difference) and sex, with the proportion of women among non-participants (n = 42, 33%) not statistically different from the participants.
Fig. 1. Flow-chart illustrating the recruitment of study participants.
CP: cerebral palsy; ICD-10: International Statistical Classification of Diseases and Related Health Problems Tenth Revision.
Of the 49 subjects who participated on-site, 16 were assisted by a proxy. Twelve participated via telephone, 4 independently and 8 through a proxy (all parents). Reviews of medical records were added, with consent, as needed to complete and confirm data, including diagnosed co-morbidities.
The mean age of the participants was 21 years and 2 months (standard deviation (SD) 8 months). There were 27 women (44%). Distributions of GMFCS, MACS and CFCS levels, clinical subtypes and intellectual disability are presented in Fig. 2a–c. Thirty-five percent were born preterm (< 37 weeks gestational age) and 14% post-term. Thirty-four percent were diagnosed with epilepsy.
Fig. 2. (a) Distribution of levels within the classification systems for the study sample of young adults. GMFCS: I (n = 25, 41%), II (n = 8, 13%), III (n = 7, 12%), IV (n = 9, 15%), V (n = 12, 20%). MACS: I (n = 13, 22%), II (n = 24, 41%), III (n = 4, 7%), IV (n = 4, 7%), V (n = 13, 22%). CFCS: I (n = 33, 54%), II (n = 5, 8%), III (n = 6, 10%), IV (n = 10, 16%), V (n = 7, 12%). (b) Distribution of clinical subtypes of cerebral palsy (CP) in the study sample. Bilateral spastic CP (n = 29, 48%). Unilateral spastic CP (n = 22, 36%). Dyskinetic CP (n = 7, 11%) Atactic CP (n = 2, 3%). Unclassifiable CP (n = 1, 2%). (c) Distribution of intellectual disability (ID) within subgroups of the classification systems. GMFCS: levels I–II (21%), levels III–V (75%). MACS: levels I–II (21%), levels III–V (91%). CFCS: levels I–II (13%), CFCS III–V (100%). CP: cerebral palsy; GMFCS: Gross Motor Function Classification System; MACS: Manual Ability Classification System; CFCS: Communication Function Classification System; ID: intellectual disability.
For 16 participants (26%) 1 or both parents were born abroad, and in 7 cases (11%) both parents were born in a non-Nordic country. Eleven participants (18%) in total were born outside Sweden. Fifty-six percent of the mothers and 58% of the fathers had completed 3 or more years of higher education. Twenty-eight percent of the parents had been separated/divorced during the major part of the participant’s childhood.
The main descriptive results are shown in Table I. Twenty percent of young adults had moved away from the parental home and, of these, most lived in a single household (3 young adults lived with a partner). Approximately half of the study subjects had experience of intimate relationships and 5% were currently living with a partner. Forty-four percent were in some form of employment or tertiary or vocational education, whereas 15% had no activity at all. Thirty-one percent were dependent on parents for personal finances and 43% needed parental family support with ADL on a daily basis. Typical ADL activities where support was needed were: eating, dressing, washing, and toilet visits, and assisting in changing sleeping positions and observing signs of seizures at night.
Seventy-one percent were socializing with friends, outside home, including on evenings.
Forty-eight percent had access to employed personal assistance. Of these, most (20 out of 29 participants) were granted 2 assistants working side-by-side at least parts of the day.
There was substantial variation in the outcomes when the results were plotted by sub-groups, as shown in Table I.
Table I. Age, sex, and social outcomes for total sample, and sub-grouped by classification systems and by presence of intellectual disability
In unadjusted analysis, having moved away from the parental home was not statistically significantly associated with the levels within the classification systems, or intellectual disability. Having experience of an intimate relationship was associated only with the CFCS. Occupational status and personal finances were associated with the levels within the MACS, the CFCS, and with intellectual disability. Socializing with friends outside the home, including in the evening, was associated with the CFCS, and with intellectual disability. All associations described were negative, e.g. increasing disability on the levels of the classification systems meant a lower probability of having achieved the item. There were no statistically significant associations with sex on any of the above items (not shown in table).
Most associations became non-significant when controlling for the presence of intellectual disability. Having experience of an intimate relationship was associated with the CFCS after adjusting for intellectual disability.
Table II. Analysis of the associations between social outcomes and the levels within the functional classification systems GMFCS, MACS and CFCS, and with intellectual disability (ID). Odds ratios (crude and adjusted for ID) of having achieved the social outcome, given that the individual is in levels III–V compared with levels I–II. For ID, the crude odds ratio of having achieved the social outcome, given that the individual has ID compared with not having ID
Of the 23 participants (38% of total) within CFCS levels III–V, 20 (87%) had at some point during childhood or adolescence used augmented and alternative communication (AAC). Eleven of these 20 individuals (55%) reported experiencing a significant improvement in communication (defined here as changing to a higher functioning level within the CFCS) with AAC use.
Twenty percent of participants in this study had moved away from home, compared with 44% in age-matched official Swedish statistics (19). This represents a substantial difference, whereby young adults with CP, to a large extent, appear to remain in the parental home. However, some caution is warranted in interpreting this, as the reference statistics refer to the country as a whole, and the housing market in the Stockholm area is considered tougher than the rest of Sweden. In the previously mentioned study from southern Sweden on adults with CP aged 18–23 years, 43% had moved from the parental home (5). As independent living is a prioritized goal for the young adults, efforts should be made to facilitate the process (10).
The majority (79%) of the young adults without intellectual disability were engaged in some form of employment or higher or vocational education. Fifteen percent of the total cohort, and 21% of those without intellectual disability, had no activity at all. For comparison, the official Swedish statistics for 2015 show that 9% of all 20–24 year-olds were neither employed nor in ongoing education (20). Thus, regardless of intellectual disability status the young adults with CP were, to a larger extent, not in any occupation. In the Netherlands, Verhoef and colleagues found that, similarly, 17% of young adults with CP 20–24 years of age (without intellectual disability) were neither employed nor studying (6). Also in the Netherlands, in a cohort of adults with CP, 50% of 25-year-olds without intellectual disability were employed, but employment rates were consistently lower than the general population during follow-up (21).
Another study from the Netherlands in 2010 in young adults with CP without intellectual disability revealed that intimate relationships and sexuality were set back compared with peers (22). In the referred study, 77% had experience of intimate relationships. This is somewhat higher than the corresponding 64% among young adults without intellectual disability in the present study. However, groups were not equal: the participants in the referred study were predominantly within high-functioning GMFCS-levels.
None of the subjects with intellectual disability and none in CFCS levels III–V had independent personal finances. There were, however, no clear predictors of whether the personal finances were dependent on governmental subsidies or dependent on the parents: overall, approximately one-third of the young adults were still financially dependent on their parents.
Almost half of the young adults were reliant on family members; most often parents but also siblings (not in a role as employed personal assistants) for ADL on a daily basis, often including night-time, typically helping with dressing, washing, toilet visits, and assisting in changing sleeping positions and observing signs of seizures at night. We claim that. at this age, this is a major obstacle in transitioning to a life independent of parental / parental family support. This issue has not previously been extensively studied. Van der Slot and colleagues in the Netherlands demonstrated that almost half of adults with spastic bilateral CP had difficulties with personal care at a mean age of 36 years (23).
Associations with the classification systems and with intellectual disability
In univariate analysis the social outcomes were, to a large extent, determined by the (grouped) CFCS levels, and by the presence of intellectual disability. The MACS also displayed associations. The GMFCS displayed no significant associations with the social outcomes. When adjusting the results for presence of intellectual disability, none of the classification systems were associated with the outcomes, except for the CFCS being independently associated with having experience of intimate relationships. These findings implicate cognitive function and communication abilities as particularly important for social functioning in young adults with CP. In contrast, being classified into different gross motor function levels was of limited importance in this aspect. Other researchers have explored the independent impact of cognition and communication abilities using other definitions than the CFCS. Employing the socialization domain of the Vineland Adaptive Behavior Score, Tan and colleagues found that, for 1–24-year-olds with CP, speech impairment was an independent risk factor for low social participation, although intellectual disability, epilepsy and GMFCS level V were more important risk factors (24). An Australian postal survey of adults with CP at a mean age of 24.7 years associated lack of speech impairment with better educational achievements, with “average intellect” being the most prominent predictor of employment status, living arrangement and marital/partner status (25). In addition, it is important to consider, when attempting to separate communication and intellectual disability, reports that have shown that children with CP and severely impaired communication display progressive cognitive decline (26). Similar findings have been reported in children with specific language impairment (27). The authors of these papers have hypothesized that the ability to communicate could be important for stable cognitive development.
The results of the communication add-on data collection indicate that interventions to improve communication function were plausible in this group.
of the target population could be included. However, the inclusion rate was equal to or higher than for other studies involving similar recruitment (23, 28). Although the sample size was relatively small and certain estimates thereby uncertain, the participants appear to be representative in terms of sex, GMFCS levels, subtypes and important co-morbidities (i.e. epilepsy and intellectual disability), all these present in proportions similar to earlier population-based studies (5, 16, 29, 30).
Another limitation was our use of special schooling, rather than cognitive testing, to identify intellectual disability.
For participants with communication difficulties, data were obtained through a proxy, most often a parent. Some information, such as personal finances and occupation was not disputable, but other, such as related to friends, could have been less reliable.
The strengths of the study include a population-based recruitment approach, a prerequisite for good external validity (i.e. results that are representative for the actual population). Moreover, data collection was through direct contact by a small, instructed team, ensuring data reliability.
The authors recommend that future larger studies include formal cognitive testing as well as CFCS levels, in order to elucidate the contribution of each to the social situation.
At 20–22 years of age, most young adults with CP were still in the parental home. Many were still dependent on their parents, both financially, and for support with daily ADL. A majority of the young adults without intellectual disability were employed or studying. There was, however, an increased risk of not having any occupational activity. Intellectual disability and communication function were important determinants of the social situation. Interventions aimed at alleviating the impact of these particular disabilities should be prioritized.
The authors wish to thank all the participants for their time and effort. We acknowledge statistician Nicklas Pihlström (Center for Clinical Research Sörmland, Eskilstuna, Sweden) for support with the data analysis.
This study has been supported by grants from the Stockholm County Council and Center for Clinical Research Sörmland, Uppsala University, Eskilstuna, Sweden, as well as from the independent foundations Linnéa och Josef Carlssons Stiftelse, Norrbacka-Eugenia Stiftelsen, Stiftelsen Promobilia, Sällskapet Barnavård, Riksförbundet för Rörelsehindrade Barn och Ungdomar and Stiftelsen Frimurare Barnhuset.
The funders did not participate in the study design, the data collection, data analysis or manuscript preparation or decisions on the manuscript.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize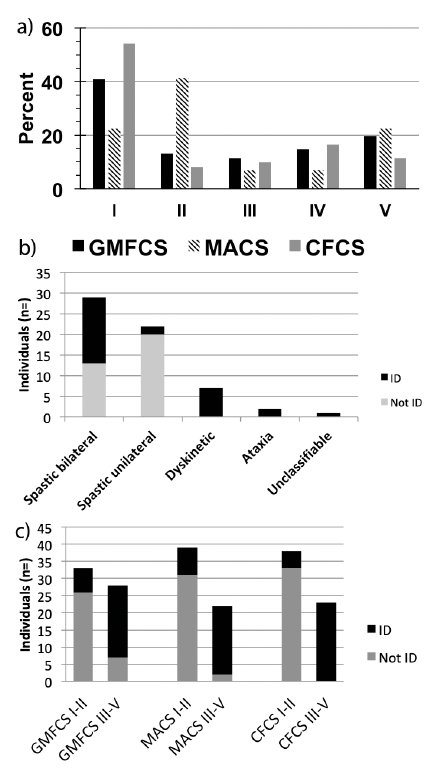 Click to show fullsize
Click to show fullsize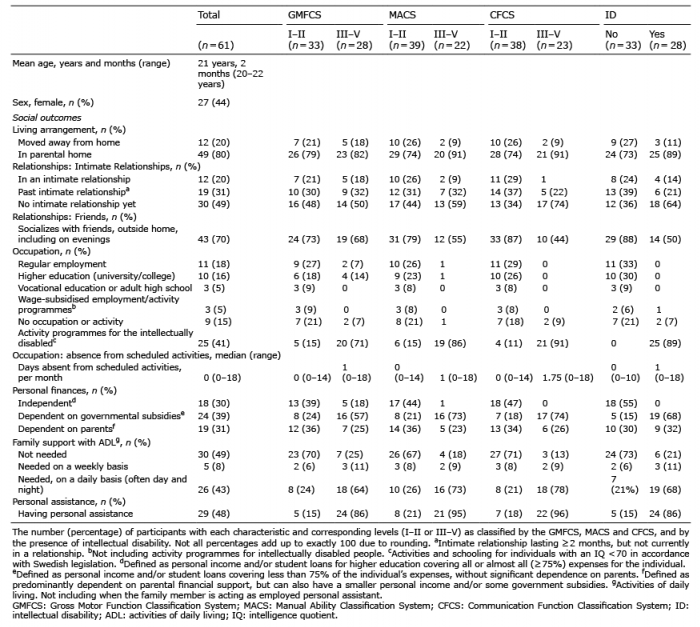 Click to show fullsize
Click to show fullsize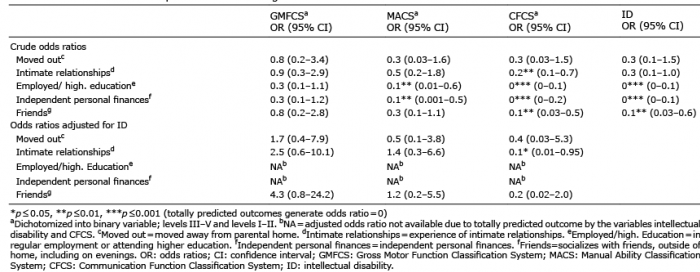 Click to show fullsize
Click to show fullsize