
From the 1Department of Rehabilitation Medicine, Hannover Medical School, Hannover, Germany, 2Graduate Program Faculty of Medicine, Universitas Gadjah Mada, Yogyakarta and 3Department of Physical Medicine and Rehabilitation, Faculty of Medicine, Universitas Padjadjaran/Hasan Sadikin General Hospital, Bandung, Indonesia
People with disability (PWD) in Indonesia are often neglected by society. Improving their life situation towards full participation in society is crucial. As a health strategy, rehabilitation can improve func-tioning, quality of life and participation in society. However, rehabilitation services in Indonesia need improvement. Making a situation analysis of rehabilitation services and their provision in the country is a pre-requisite to taking any action towards improvement. This paper compiles available data related to disability and rehabilitation services in Indonesia, using the Rehabilitation Services Assessment Tool (RSAT) as a framework. Gaps in provision were analysed, resulting in the compilation of a list of generic recommendations to improve rehabilitation services in the country. Indonesia faces many challenges in rehabilitation services, including the health workforce and the provision of services. This situation analysis and list of generic recommendations may be used in further discussions with relevant stakeholders in the country to develop a national strategy to strengthen rehabilitation services.
Key words: rehabilitation service situation analysis; rehabilitation advisory teams; national disability; health and rehabilitation plan; rehabilitation services; rehabilitation professions.
Accepted Feb 26, 2018; Epub ahead of print Mar 26, 2018
J Rehabil Med 2018; 50: 377–383
Correspondence address: Boya Nugraha, Department of Rehabilitation Medicine, Hannover Medical School, Carl-Neuberg-Str.1, DE-30625, Hannover, Germany. E-mail: boya.nugraha@gmail.com
People with disability (PWD) in Indonesia are often neglected by society, as they are regarded as unproductive. Even before Indonesia signed the United Nations Convention on the Rights of People with Disability (UNCRPD) in 2007 (1) the Government of the Republic of Indonesia was concerned about the rights of PWD. Indonesia has many regulations accommodating and facilitating the rights of PWD (2). Four years after signing the UNCRPD, Indonesia ratified it (1). Following this ratification, many regulations have been revised to facilitate greater inclusiveness of PWD into society, including in the fields of education, labour, transport and health. However, there remain unmet needs of PWD, which require further elucidation.
Indonesia also adopted the World Health Organization (WHO) Global Disability Action Plan 2014–2021: “Better health for all people with disability” (GDAP) during the World Health Assembly 2014. On this basis, several actions to improve health service provision for PWD need to be implemented, particularly at the level of health systems. However, before any action is taken, the current situation of rehabilitation services in the country must be analysed. The aim of this study is therefore to evaluate rehabilitation services at the level of health systems by collecting and analysing available data related to disability and rehabilitation services in Indonesia. The study used available methodology; the Rehabilitation Situation Assessment Tool (RSAT) (3). The results were also used to identify gaps in the rehabilitation services. Generic recommendations were generated as a proposed basis for strengthening rehabilitation services in the country.
This was a retrospective review study using secondary data from existing publicly accessible information. Data were collected according to the RSAT framework (3); specifically the following sections:
Sources used to collect data were published WHO, government and non-state actors (NSAs) documents (including their websites), interviews by phone and email with NSAs, which focus on rehabilitation service delivery. All the information was discussed and summarized during an authors’ group held in Hannover, and a list of generic recommendations was generated as a proposal to strengthen rehabilitation services at the level of health systems in Indonesia.
Indonesia is a large country with a population of approximately 260 million. It is the fourth most populated country in the world (4). Indonesia consists of more than 13,000 islands (4), many of which have poor infrastructure and difficulty accessing health services.
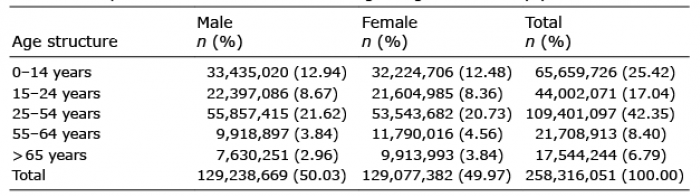
Indonesia has a young population (Table I); more than 42% of the population is below 25 years of age, with 21.6% male and 20.8% female. The total working age population (25–64 years old) is 42.3%. Approximately 7% of the population is over 65 years old. Indonesia is categorized as a lower middle income country according to the World Bank (5). The Government of Indonesia recognizes 6 religions (Islam, Protestantism, Catholicism, Hinduism, Buddhism and Confucianism). Indonesia is quite diverse in terms of ethnic groups, with Javanese the largest group, follow by Sundanese and Malay, at 40.1%, 15.5% and 3.7%, respectively. The proportion of other ethnic groups is less than 3.7%. The official language is Bahasa Indonesia (4), but the diversity of ethnic groups means that Indonesia has more than 700 languages.
Table I. Population of Indonesia according to age structure (4)
The prevalence of non-communicable diseases is higher than that of communicable diseases. Stroke, cancer, coronary heart disease and diabetes mellitus are the most common causes of death in Indonesia (Table II) (6). Risk factors, such as alcohol consumption, are 0.09 (in litres of pure alcohol) per capita (7). The prevalence of tobacco smoking is 76.2% (8).
Table II. Eleven main causes of death in Indonesia (modified; (6))
Indonesia has a national health system (NHS), which was implemented in 1982. This has been revised several times, including in 2004, 2009 and 2012. In the latest version, Indonesia declared that, by 2019, the country will provide an affordable health system that can be accessed by all citizens (9). This policy has been further supported by the establishment of a Social Security Administration (SSA) in 2014, called the Badan Penyelenggara Jaminan Sosial (BPJS) (10, 11). SSA works on health and employment issues.
Health service provision in Indonesia can be divided into primary, secondary and tertiary levels. Community-based rehabilitation services (CBR) are also available in many parts of the country. Other community-related services, including maternal and child health centres (integrated service post/Pos Pelayanan Terpadu (Posyandu)) (12), are spread across the whole of Indonesia and reach the lowest level of governmental structure. In general, the health workforce in Indonesia is quite low; for example, the density of physicians is 0.21 per 1,000 population (13).
Disability in Indonesia is defined in National Law number 8, 2016, based on the framework of the International Classification of Functioning, Disability and Health (ICF) (15).
According to a survey conducted in 2010 by the University of Indonesia and National Team to Accelerate Poverty, the proportion of PWD in Indonesia was 4.3%, based on Washington Group questions (14). This figure is lower than the average world prevalence rate of disability in the adult population, which is 15.6%, according to the World Report on Disability (WRD) (15).
Table III illustrates the prevalence of disability in Indonesia by type and degree in the population over the age of 10 years. Most PWD have visual impairment (3.05%). Other impairments or disabilities are: hearing, walking or climbing stairs, remembering or concentrating, and self-care, at 1.58%, 1.62%, 1.44% and 1.07%, respectively (16).
Table III. Prevalence of disability by type and degree of disability (in population over 10 years of age; modified (16))
The prevalence of disability by age and degree of disability in Indonesia over the age of 15 years is shown in Table IV. Approximately 23% of people between 50 and 69 years old have severe and very severe disability. Furthermore, more than 50% people age 70 years and older have severe and very severe disability. Almost 38% of people age 70 years and older have difficulties with daily living (14). Meanwhile, almost 40% of PWD have more than one disability (17).
Table IV. Disability prevalence in adult (%) by age group and degree of disability (modified; (14))
According to National Law number 8, 2016, described above, disability in Indonesia is classified as physical, intellectual, mental and/or sensory. However, it can also be a combination of these classifications.
The Ministry of Social Welfare is primarily responsible for PWD. It has budget allocation for social services and rehabilitation of PWD. More than 70% of the budget is allocated to provision of social assistance or social security for people with “severe disability” or “irreversible disabilities”. The remainder is used to build infrastructure and develop human resources (2).
Within the Ministry of Health, rehabilitation services are facilitated through the NHS. It provides rehabilitation services and basic assistive devices. There are 7 types of assistive device covered by the Indonesian NHS: eyeglasses, hearing aids, incisors, collar neck/cervical collar/neck braces, corsets, extremity prostheses/dentures, and crutches (18). In addition to national/government health insurance, private insurance is also available in Indonesia. Under private insurance, health-related services are covered according to the contract between consumers and insurance companies, some of which cover rehabilitation-related services.
In addition, the Ministry of Health has regulated that rehabilitation services should be implemented as an integral part of the service in hospital types A (top referral), B (provincial) and C (city). In Indonesia, acute, post-acute and long-term rehabilitation services also exist, particularly in hospital types A, B and C. However, there are no data available on these services.
The rehabilitation workforce in Indonesia includes Physical and Rehabilitation Medicine (PRM) physicians, physiotherapists (PT), occupational therapists (OT), prosthetists and orthotists (P&O), speech and language therapists (SLT) and psychologists. In Indonesia, there are approximately 600 PRM physicians spread over 26 out of 34 provinces. The numbers of PT, OT, PO, and SLT are approximately 9,000, 1,400, 400 and 900, respectively (Table V).
Table V. Rehabilitation-related professionals in Indonesia
Table VI shows the number of academic institutions and the level of education programmes offered by institutions in Indonesia. A PRM specialist academic certificate is awarded to medical doctors who take an additional 4-year specialist programme in 1 of 5 state universities in Indonesia. PT is offered by state and private academic institutions at 3 different education levels, starting from a 3-year programme until Master’s degree. Meanwhile, OT, P&O, and SLT only have 3 and 4 year’s education programmes in 2 state universities. Social workers have different levels of education programmes, from diploma 1 (1-year programme) up to a Master’s degree, offered either by state or private academic institutions.
Table VI. Number of academic institutions related to rehabilitation professions in Indonesia (24)
Based on our findings from the situation analysis referring to the RSAT (3), the following recommendations were developed by the authors. The recommendations are divided into several topics, as follows:
1. ICF-related recommendations:
Although Indonesia has a law that defines disability based on the framework of the ICF model, some actions to implement ICF in the health services should be taken into account, such as:
2. Government:
In Indonesia, PWD are under the responsibility of different ministries; therefore, the recommendations are as follows:
3. Rehabilitation services:
The poor distribution of rehabilitation professionals in many parts of the country should be overcome.
The aim of this article was to analyse the situation of rehabilitation services and disability in Indonesia. Thus, it does not follow the overall methodology for developing a National Disability, Health and Rehabilitation Plan (NDHRP) (26–28). However, the RSAT questionnaire was used as a tool on which to base the systematic collection of information and data. The data sources were based on available public sources (e.g. the WHO, government and non-governmental organization (NGO) documents and reports, published papers, etc.), consultations with NSAs, including national professional organizations, was carried out by direct discussion, phone and/or email.
The results of this study confirm that the RSAT is feasible for use in analysing the situation of disability and rehabilitation services in a country. However, the analysis was not comprehensive, as some limitations occurred, including site visits, discussion with government offices (such as representatives of the Ministry of Health and the Ministry of Social Welfare) and discussion with NSA of PWD. Site visits to rehabilitation centres were represented by one of our authors (IRD), who works at a rehabilitation centre at a tertiary hospital in West Java Province and has many years’ experience in rehabilitation services.
The results show that the reported prevalence of PWD in Indonesia is lower than the average of worldwide data published by the WHO (4.3% and 15%, respectively). However, it is likely that the number of PWD in Indonesia is greater than 4.3%. This difference, and the difficulties of assessing disability in the country, could be due to a different definition of disability used in the survey, lack of awareness and understanding of disability by the general population, and other factors (29). Therefore, the use of the WHO – Model Disability Survey is recommended in order to collect more comprehensive data for comparison with that from other countries.
An ageing population, chronic health conditions, environmental and other factors are the causes of disability worldwide, including in Indonesia. Regarding the ageing population, Indonesia will face an increased number of PWD within the next 15–25 years. Based on the 2010 survey, approximately 7% of the population are over 65 years old. It is estimated that the proportion of Indonesia’s population over 60 years old will increase to 12.8% and approximately 22.3% in 2025 and 2050, respectively (30). Thus, the rate of ageing of the population in Indonesia is quite high. Various debates related to ageing and disability are ongoing. Some argue that there will be a decrease in the prevalence of disability as life expectancy increases (compression morbidity); others that there will be an increase in the prevalence of disability as life expectancy increases (expansion comorbidity) (31). Disability in the ageing population tends to decrease in high income countries (31). Indonesia is categorized as a lower middle income country. There is no published report, either positive or negative, on the trend of disability and ageing in Indonesia. However, considering the ageing population in Indonesia, together with the risk of disability in these populations, this subject requires serious consideration. In addition, reducing risk factors for disabling health conditions (e.g. stroke, cancer) is of importance to prevent disability (e.g. through non-smoking campaigns or programmes).
Indonesia has a very large population, of approximately 260 million (6); however, there is an enormous lack of capacity regarding health provision and the number of health professionals, including in the field of rehabilitation. For example, in high income countries, the ratios of PRM, PT and OT per 1 million population are 20, 850 and 4, respectively (32). As shown in Table V, these ratios are much lower for rehabilitation professionals in Indonesia. Other barriers are geographical, e.g. regarding urban and rural areas. Indonesia consists of more than 13,000 islands (4), many of which are isolated islands with poor infrastructure and difficulty accessing health services.
Although the Government of Indonesia has established a regulation that rehabilitation medicine should be an integral part of hospital types A, B and C, the low number and poor distribution of rehabilitation professionals are huge challenges, as most of them work in large cities and there are little data available.
Rehabilitation for PWD in Indonesia is the responsibility of, in particular, the Ministry of Health and the Ministry of Social Welfare; therefore it is strongly recommended that actions and programmes for PWD are coordinated between ministries.
Based on the results of this study, the authors have proposed a number of recommendations to strengthen rehabilitation services in Indonesia. These recommendations are generic, since they were discussed only among the authors according to the results of situation analysis. Furthermore, this generic list of recommendations cannot be classed as priorities according to the most relevant needs of the country, since no stakeholder dialogue was performed.
Based on these situation analyses, it is clear that Indonesia still faces challenges with regard to PWD. In the health services, it is indispensable to strengthen rehabilitation services, including in the areas of the rehabilitation health workforce and its distribution, coordination among ministries, education, and information about disability and rehabilitation service provision.


 Click to show fullsize
Click to show fullsize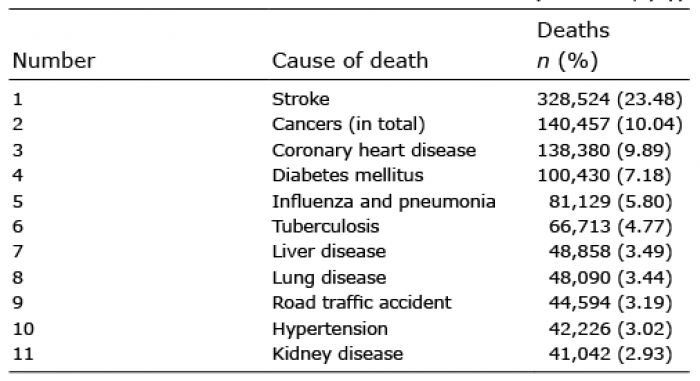 Click to show fullsize
Click to show fullsize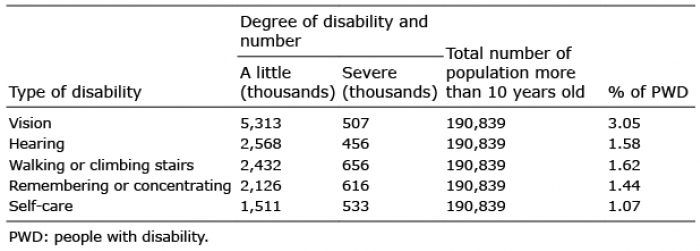 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize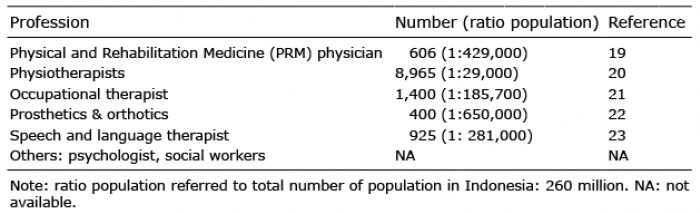 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize