
From the 1Institute of Neuroscience and Physiology, Section of Health and Rehabilitation, Physiotherapy, Sahlgrenska Academy, University of Gothenburg, 2University of Gothenburg Centre for Person Centred Care (GPCC), Gothenburg, 3Department of Clinical Sciences, Karolinska Institutet and Department of Rehabilitation Medicine, Danderyd Hospital, Stockholm, 4Department of Dental Medicine, Karolinska Institutet, and Scandinavian Center for Orofacial Neurosciences (SCON), Huddinge, 5Sahlgrenska University Hospital, Rheumatology, Göteborg, 6Pain and Rehabilitation Centre, and Department of Medical and Health Sciences, Linköping University, Linköping and 7Department of Clinical Neuroscience, Karolinska Institute and Stockholm Spine Center, Stockholm, Sweden
Objectives: Resistance exercise results in health benefits in fibromyalgia. The aim of this study was to determine the factors that mediate change in muscle strength in women with fibromyalgia as a result of resistance exercise.
Methods: Sixty-seven women with fibromyalgia (age range 25–64 years) were included. Tests of muscle strength and questionnaires related to pain, fear
avoidance and physical activity were carried out. Multivariable stepwise regression was used to analyse explanatory factors for change and predictors for final values of knee-extension force, elbow-flexion force and hand-grip force.
Results: Change in knee-extension force was explained by fear avoidance beliefs about physical activity at baseline, together with change in pain intensity, knee-extension force at baseline, age and body mass index (BMI) (R2=0.40, p = 0.013). Change in elbow-flexion force was explained by pain intensity at baseline, together with baseline fear avoidance beliefs about physical activity, BMI and elbow-flexion force at baseline (R2 = 0.32, p = 0.043). Change in hand-grip force was explained by hand-grip force at baseline, change in pain intensity and baseline fear avoidance (R2 = 0.37, p = 0.009). Final muscle strength was predicted by the same variables as change, except pain.
Conclusion: Pain and fear avoidance are important factors to consider in rehabilitation using resistance exercise for women with fibromyalgia.
Key words: physiotherapy; rehabilitation; chronic pain; physical exercise.
Accepted Aug 18, 2017; Epub ahead of print Oct 25, 2017
J Rehabil Med 2017; 49: 744–750
Correspondence address: Anette Larsson, Institute of Neuroscience and Physiology, Section of Health and Rehabilitation, Physiotherapy, Sahlgrenska Academy, University of Gothenburg, Box 430, SE-40530 Göteborg, Sweden. E-mail: anette.e.larsson@vgregion.se
Musculoskeletal pain has a negative impact on quality of life and work capacity (1) for individuals, with high costs to society due to long-term sickness absence (2). Fibromyalgia (FM) affects approximately 1–3% of the general population, is more common among women, and the prevalence increases with age (3). FM is characterized by persistent widespread pain, increased pain sensitivity and tenderness (4), and is associated with impaired physical capacity (5) and activity limitations (1).
Muscle strength is needed to accomplish activities of daily living, such as walking, climbing stairs and lifting and carrying heavy objects. Muscle strength decreases with increasing age due to sarcopaenia, i.e. age-related loss of muscle mass and function. Causes of sarcopaenia are multifactorial and could include inflammation, chronic disease and declining levels of physical activity (6). Muscle-strengthening activity, such as resistance exercise, is recommended in the general population in order to prevent age-related loss of muscle mass, impaired physical function (7) and the development of degenerative age-related chronic conditions (8). The prevention of loss of muscle mass and physical function might be even more important in the population with FM, given their impaired muscle strength (5) and reduced levels of physical activity (9). As muscle strength has been associated with pain in FM (10) it is reasonable to assume that a longer duration of FM symptoms is associated with lower levels of muscle strength (5).
Although the precise aetiology of FM is not known, physical deconditioning is expected to contribute to the development of FM (11). One reason for deconditioning is that women with FM are less physically active than healthy age-matched controls. Women with FM engage more in sedentary activities and less in physical activities of all intensities (9).
One common hindrance for resistance exercise as well as outcome of exercise in FM is activity-induced pain during isometric loads (12). Pain in FM commonly hinders all exercise at a strenuous level (13) and can raise fear avoidance beliefs about physical activity (14). As activity-induced pain is a common feature in FM, this might be a reason for the avoidance of heavier physical activities (15). An additional hindrance might be being overweight, which is common in FM (16, 17), as a previous study indicated that obesity might negatively influence the outcomes of exercise (18).
Our RCT, investigating the effects of a resistance exercise programme showed a significant improvement in muscle strength at the group level (19). However, the wide standard deviation implied large individual differences in change. Some participants increased their muscle strength, while others did not (19). We found it of interest to study whether the factors presented above might have an influence on a patient’s ability to perform resistance exercise and to increase muscle strength.
We hypothesized that baseline muscle strength, age, disease duration, amount of leisure time physical activity, pain, fear avoidance and body mass index (BMI) may contribute to explain increase in muscular strength following resistance exercise in women with FM.
This is a secondary within-group analysis of women with FM randomized to the resistance exercise arm of a RCT (19), examining explanatory factors for change in muscle strength, and predictors for the final value of muscle strength. The study was approved for all sites by the regional ethics committee in Stockholm (2010/1121-31/3). The trial was registered on 21 October 2010 with ClinicalTrials.gov (identification number: NCT01226784). Written and oral information was given to all participants, and written consent was obtained from all participants.
Recruitment started in 2010 and data collection was completed at all sites (Gothenburg, Stockholm and Linköping) in 2013. Inclusion criteria were: women aged 20–65 years, meeting the American College of Rheumatology (ACR) 1990 classification criteria for FM (4). Exclusion criteria were: other severe somatic or psychiatric disorders that would be anticipated to affect participation in the study, such as high blood pressure (>160/90 mmHg), osteoarthritis (OA) in hip or knee, other dominating causes of pain than FM, regular resistance exercise or relaxation therapy twice a week or more, inability to understand or speak Swedish, and not being able to refrain from analgesics, non-steroidal anti-inflammatory drugs (NSAIDs) or hypnotic drugs for 48 h prior to examinations.
Participants were recruited through newspaper advertisements in the local newspapers of 3 cities in Sweden (Gothenburg, Stockholm and Linköping). A total of 177 women who were interested in participation were referred to a medical examination for further enrollment. The women were screened for eligibility by an experienced physician to verify ACR 1990 criteria for FM (4). A total of 130 women with FM fulfilled the inclusion criteria. After completing baseline examinations, participants were randomized and informed of group allocation. The flow diagram and the randomization process are described in detail in the RCT (19). All participants were invited to post-treatment examinations and 84% (n = 56) of the women in the resistance exercise group completed the examinations and were included in this study (19).
The resistance exercise programme was performed twice a week for 15 weeks in small groups comprising 5–7 participants. Estimation of 1 repetition maximum (1RM) was made by submaximal ratings for health and safety reasons (20). Each participant was asked to perform their maximum number of repetitions until perceived exhaustion at an individually adjusted, given resistance. 1RM was based on the number of repetitions performed. The exercise was initiated at low loads corresponding to 40% of 1RM (1–2 sets, 15–20 repetitions) and progressed up to 80% of 1RM (1–2 sets, 5–8 repetitions) during the 15 weeks. A more detailed description of the procedure of the resistance exercise and the adjustment of loads has been reported previously (19).
Outcomes were assessed at baseline and immediately after the 15-week intervention period. Examinations included self-administered questionnaires, performance-based tests of muscle strength and assessment of current pain intensity. Baseline and post-treatment examinations were performed by the same physiotherapists.
The dependent and independent variables included in the analyses of explanatory factors for variability of change in muscle strength and predictors for the final value of muscle strength are described below.
Dependent variables. Change in muscle strength was analysed using 3 dependent variables: change in maximal isometric knee-extension force, change in maximal isometric elbow-flexion force and change in hand-grip force.
The final value for muscle strength was analysed using 3 dependent variables: final value of maximal isometric knee-extension force, final value of maximal isometric elbow-flexion force and final value of hand-grip force.
Maximal isometric knee-extension force (N) was measured bilaterally with a dynamometer (Steve Strong®: Stig Starke HBI, Göteborg, Sweden) using a standardized protocol. The best performance out of 3 trials was recorded. A mean value for the right and left legs was calculated (21, 22). This method has been reported to show satisfactory test-retest reliability (22).
Maximal isometric elbow-flexion force (kg) was measured bilaterally using a dynamometer (Isobex®: Medical Device Solutions AG, Oberburg, Switzerland). The upper arm was aligned with the trunk and the elbow in 90° of flexion (23). The best performance out of 3 trials was recorded. A mean value for the right and left arms was calculated.
Hand-grip force (N) was registered bilaterally using Grippit® (AB Detektor, Göteborg, Sweden). The mean force over a set period of time (10 s) was recorded (24). The best performance out of 2 trials was recorded. A mean value for the right and left hands was calculated.
Selection of independent variables for change in muscle strength. Variables included in the analyses as potential explanatory factors or predictors are described below.
Baseline value of the dependent variable knee-extension force, elbow-flexion force and hand-grip force was included in each model as an independent variable.
Age and symptom duration were selected as muscle strength decreases with older age and a longer period of illness entails a longer period of lowered activity levels.
Leisure Time Physical Activity Index (LTPAI), assessing the total amount of physical activity during a normal week in h (25) was included. It was of interest to investigate whether the baseline amount of physical activity was related to change in muscle strength or final value for muscle strength and whether change in the amount of physical activity was related to change in muscle strength.
Pain intensity was included in the analysis. Pain is associated with muscle strength in FM (10). From a clinical perspective it is reasonable to assume that baseline pain intensity and a change in pain intensity during the intervention period would influence the ability to perform resistance exercise as well as the outcome of the exercise. Current global pain intensity (visual analogue scale; VAS) was rated on a 0–100 VAS, ranging from “no pain at all” to “worst imaginable pain”. VAS has been reported to be a useful measure of pain intensity in most settings (26).
The Fear Avoidance Beliefs Questionnaire, physical subscale (FABQphysical) was included in the analysis. Both baseline values and values for change in fear avoidance were selected, as fear avoidance is thought to influence the ability to perform exercise at a strenuous level. Fear avoidance was expected to change during the intervention period when the participants were confronted with their pain during exercise, and this could influence the ability to perform exercise and thus the outcome of exercise. FABQphysical was used to assess how much fear and avoidance affect physical beliefs (4 items, 0–24). A higher score represents more fear avoidance beliefs (27).
Body mass index (BMI): previous research has shown an association between BMI and muscle strength, thus BMI was included in the analyses (17).
Data were computerized and analysed using the Statistical Package Software for the Social Sciences (SPSS version 22.0, Armonk, NY, USA. Descriptive data are presented as mean, standard deviation (SD), median (min; max) for continuous variables or the number (n) and percentage (%) for categorical variables. All significance tests were 2-sided and conducted at the 5% significance level. Only measured values were included in analyses of changes over time, implying that cases missing were not included in the analysis. The Spearman correlation coefficient was used for correlation between the dependent variables of change in muscle strength and baseline measures, and measures of change in the independent variables as well as for correlation between the final values of muscle strength and baseline values in the independent variables. Variables with a p-value < 0.2 on analysis of correlation were included in further analyses using multiple linear forward stepwise regression analysis. The assumptions of normality were confirmed by checking the residual scatterplots and histograms of each variable, respectively. Multicollinearity was examined by tolerance and variance inflation factor. Linear forward stepwise multiple regression analysis was performed to analyse explanatory factors for change in muscle strength and predictors for final value of muscle strength.
The characteristics of the study population are shown in Table I.
Table I. Characteristics of the study population (n = 67)
Results reported elsewhere (19) and used in this study were as follows: mean isometric knee-extension force at baseline (330.1 N; SD 109.4). Isometric knee-extension force improved significantly (p = 0.002) from baseline to post-treatment examination (Δ 30.4, SD 71.9, n = 56) (19). Mean elbow-flexion force at baseline (13.0 kg; SD 5.4). Isometric elbow-flexion force improved significantly (p < 0.001) from baseline to post-treatment examination (Δ 2.4, SD 3.3, n = 56) (19). Mean hand-grip force at baseline (161.8 N; SD 68.7). Hand-grip force improved significantly (p < 0.001) from baseline to post-treatment examination (Δ 20.1, SD 36.1, n = 52) (19). Mean pain intensity at baseline (49.3; SD 23.9). Pain intensity decreased significantly (p = 0.002) from baseline to post-treatment examination (Δ –5.7, SD 15.0, n = 56) (19). Mean Fear Avoidance physical beliefs at baseline (9.7; SD 6.1). Fear avoidance physical beliefs did not improve significantly (p = 0.36) from baseline to post-treatment examination (Δ –0.8, SD 7.0, n = 54) (19). Mean Leisure Time Physical Activity at baseline (5.6 h/week; SD 4.8). The amount of physical activity increased significantly (p < 0.001) from baseline to post-treatment examination (Δ 2.3, SD 4.8, n = 56) (19).
The results of the correlation analyses are shown in Table II. Variables that were found to correlate with change in muscle strength with p < 0.2 were entered into the linear forward stepwise multiple regression of explanatory factors.
Table II. Correlations between changes in muscle strength and independent variables (n = 56)
Variables included in the regression model for change in knee-extension force were BMI, age, baseline values for hand-grip force, knee-extension force, as well as fear avoidance beliefs and change in pain intensity. Change in knee-extension force (n = 56) was partly explained by fear avoidance beliefs about physical activity at baseline, together with change in pain intensity, knee-extension force at baseline, age and BMI. This model explained 40% of the change in knee-extension force (p = 0.013) (Table III).
Table III. Explanatory models for change in muscle strength
Variables included in the regression model for change in elbow-flexion force were BMI, baseline values for hand-grip force, elbow-flexion force, pain intensity and fear avoidance and change in pain intensity. Change in elbow-flexion force (n = 56) was partly explained by pain intensity at baseline, together with baseline fear avoidance beliefs about physical activity, BMI and elbow-flexion force at baseline. This model explained 32% of the change in elbow-flexion force (p = 0.043) (Table III).
Variables included in the regression model for change in hand-grip force were BMI, baseline values for fear avoidance and hand-grip force and change in pain intensity. Change in hand-grip force (n = 52) was partly explained by hand-grip force at baseline, change in pain intensity and baseline fear avoidance. This model explained 37% of the change in hand-grip force (p = 0.009) (Table III).
The results of the correlation analyses are shown in Table IV. Variables that were found to correlate with final value with p < 0.2 were entered into the linear forward stepwise multiple regression of predictors.
Table IV. Correlations between final muscle strength and independent variables (n = 56)
Variables included in the regression model for final knee-extension force were age, symptom duration, BMI, pain, fear avoidance and baseline knee-extension force. Final knee-extension force (n = 56) was partly predicted by knee-extension force at baseline, fear avoidance beliefs about physical activity, age and BMI. This model predicted 75% of the final knee-extension force (p = 0.018) (Table V).
Table V. Predictive models for final muscle strength
Variables included in the regression model for final elbow-flexion force were: age, symptom duration, BMI, LTPAI, fear avoidance and baseline value for elbow-flexion force. Final elbow-flexion force (n = 56) was partly predicted by baseline elbow-flexion force, BMI and fear avoidance beliefs about physical activity. This model explained 72% of the final elbow-flexion force (p = 0.030) (Table V).
Variables included in the regression model for final hand-grip force were age, symptom duration, LTPAI, fear avoidance and baseline hand-grip force. Final hand-grip force (n = 52) was partly predicted by baseline hand-grip force and age. This model predicted 75% of the final hand-grip force (p = 0.023) (Table V).
The aim of this study was to investigate factors that contribute to explain change in muscle strength and factors that predict the final value of muscle strength following 15 weeks of person-centred progressive resistance exercise. Resistance exercise is difficult for women with FM due to activity-induced pain and the behavioural consequences of this, such as fear and avoidance of physical activities (28). Two factors, pain and fear avoidance, were found to be independent explanatory factors in analyses of change in 3 muscle groups. Fear avoidance at baseline was also a predictor for the final values of knee-extension force and elbow-flexion force. Thus, pain and fear avoidance appear to be important factors to consider when planning exercise to improve muscle strength in FM. Forty percent of the change in knee-extension force was explained by fear avoidance at baseline, change in pain intensity, knee-extension force at baseline, age and BMI. There may be several possible explanations, such as that the participants with lower degree of fear avoidance ventured to exercise on loads sufficient to improve muscle strength. Decrease in pain during the exercise period probably further encouraged the participants to exercise at higher loads. Age was negatively related to change in knee-extension force, implying that the participants with higher age had less improvement in muscle strength, which is in line with a previous study stating that there is a natural age-related decline in muscle mass (6). The inverse relationship was found between BMI and variation in knee-extension force, where participants with overweight and obesity seemed to increase their knee-extension force more than participants with optimal BMI. This finding is supported by a previous study showing good knee-extension force in subjects with overweight and moderate obesity (17). Seventy-five percent of the final knee-extension force was predicted by same variables, except pain intensity, implying that higher baseline knee-extension force, less baseline fear avoidance, lower age and higher BMI predicted higher final muscle strength.
The final elbow-flexion force was to 72% predicted by higher baseline value for elbow flexion, higher BMI and lower baseline value for fear avoidance. Analysis of change in elbow-flexion force showed a slightly different pattern. Thirty-two percent of change was explained by baseline pain intensity, but not the change in pain, together with baseline fear avoidance, BMI and baseline elbow-flexion force. Thus, baseline pain and baseline fear avoidance appear to be important factors to take into consideration when planning resistance exercise for muscles involved in elbow flexion. Muscle strength is substantially reduced in upper extremities in FM (29, 30), which warrants further development of exercise programmes for these muscle groups. A factor not included in the regression model is the resistance exercise itself, as exercise of large muscle groups is supposed to facilitate improvement in muscle strength not only in the muscles exercised, but simultaneously also in small muscle groups (31). General physiological mechanisms, such as growth factors that are mobilized during exercise, might be involved in this process (32).
The final hand-grip force was to 75% predicted by lower age and higher baseline hand-grip force. Change in hand-grip force was explained by 37%, indicating that lower fear avoidance and lower hand-grip force at baseline, together with decrease in pain during the exercise period explained improvement in hand-grip force. As mentioned previously, the exercise of large muscle groups might also have contributed to improvement in hand-grip force. Hand-grip force reflects a person’s general physical capacity (33), and is suggested to be a generic measure of physical function and activity limitations in FM (34).
The final values of muscle strength were not predicted by baseline value of pain in any of the 3 analyses of muscle strength. However, in all 3 analyses of change in muscle strength, either baseline pain, or change in pain, was an explanatory factor, indicating its importance for the rehabilitation process of patients with FM. As pain is usually a barrier to exercise, managing pain during the exercise period is important and the risk for exercise-induced pain can be reduced by gradual introduction to heavier loads (35). Several clinical studies indicate that an adequately designed exercise programme decreases pain over time among people with FM (36), and several components related to exercise may contribute to the decrease in pain. Another recently published study from our research team shows that concentrations of pyruvate, glutamate and glucose decreased during the resistance exercise period (37). As elevated concentrations of pyruvate and glutamate are associated with peripheral nociceptive pain mechanisms, the decrease in these concentrations indicates that exercise probably induced a positive effect on peripheral pain mechanisms.
In our sample the levels of fear avoidance were relatively low at baseline, with only 23% of the participants displaying high fear avoidance, i.e. FABQ physical >14 (0–24). The results of this study show that, even though baseline values are rather low, fear avoidance seems to be an important factor to address when treating patients with FM. Symptom duration and baseline physical activity level did not have any explanatory value for change in muscle strength. This indicates that all persons with FM with interest in improving their physical capacity by means of resistance exercise should be encouraged to try this mode of exercise.
Physical exercise is important; it is part of first choice management of FM, and has been shown to improve physical capacity and reduce pain (36) when appropriately prescribed. Several factors interact during a complex intervention, for example how exercise is planned, adjusted and progressed in order to reduce the risk of increased pain.
Muscle strength is a fundamental component of fitness which refers to the capability of an individual to have the physical requirements for work and daily activities (38). High muscle strength is consistently associated with lower levels of pain and lower scores on psychological factors associated with pain (10). There seems to be a reciprocal relationship between physical function and self-efficacy, implying that improving physical function improves self-efficacy and vice versa (39).
The submaximal rating of 1RM, together with the participant’s experience, was used for guidance when deciding the exercise loads and the progression in the resistance exercise. This is not an exact measure of strength, but it was considered applicable for this study.
This study has some limitations. The recruitment procedure, i.e. newspaper advertisements, may have resulted in recruitment of participants who were motivated to exercise, and this could bias the results. To minimize this risk the advertisement was designed to recruit participants to both interventions, so that none of the participants would know in advance which intervention was the active intervention or the control intervention. In addition, the R-square values in the regression models for change in muscle strength are fairly low and the results indicate that there are unknown factors that also contribute to change in muscle strength.
Decreased pain and low fear avoidance contributed to the change in muscle strength in this study following the resistance exercise intervention. This emphasizes the importance of adjusting the programme to each individual and stresses the importance of carefully selected loads and exercises intended to increase muscle strength without increasing pain and fear avoidance. Using person-centred principles in rehabilitation (19, 40) seems to be effective in changing avoidance behaviour towards physical activity.
The authors gratefully acknowledge colleagues who performed examinations and supervised the groups in Gothenburg, Alingsås, Linköping and Stockholm during the intervention.
The study was supported by the Swedish Rheumatism Association, the Swedish Research Council (K2009-52P-20943-03-2, K2011-69X-21874-01-6 & K2015-99X-21874-05-05), the Health and Medical Care Executive Board of Västra Götaland Region, ALF-LUA at Sahlgrenska University Hospital, Stockholm County Council (ALF) and Gothenburg Center for Person Centered Care (GPCC), Swedish Research Council (K2009-69P-21300-04-4, K2013-52X-22199-01-3, K2015-99x-21874-05-4, 2011-4807, K2009-52P-20943-03-2), Karolinska Institutet Foundation and AFA Insurance (140341). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize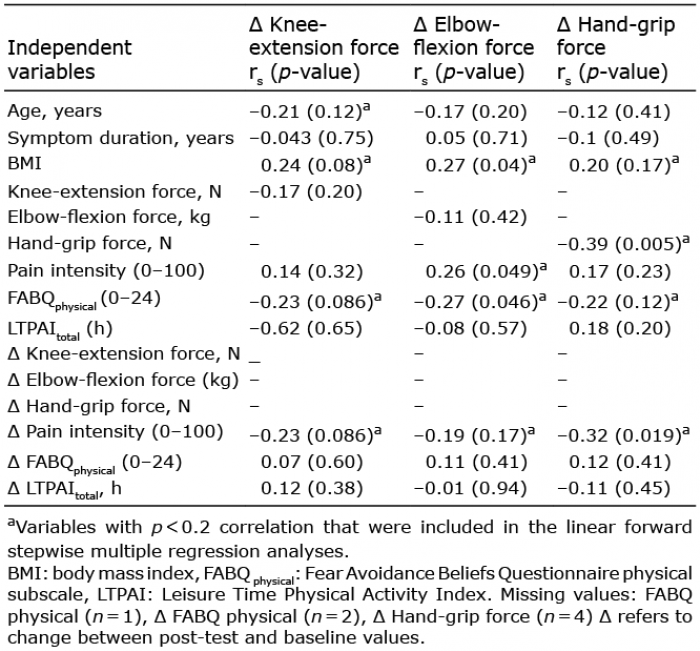 Click to show fullsize
Click to show fullsize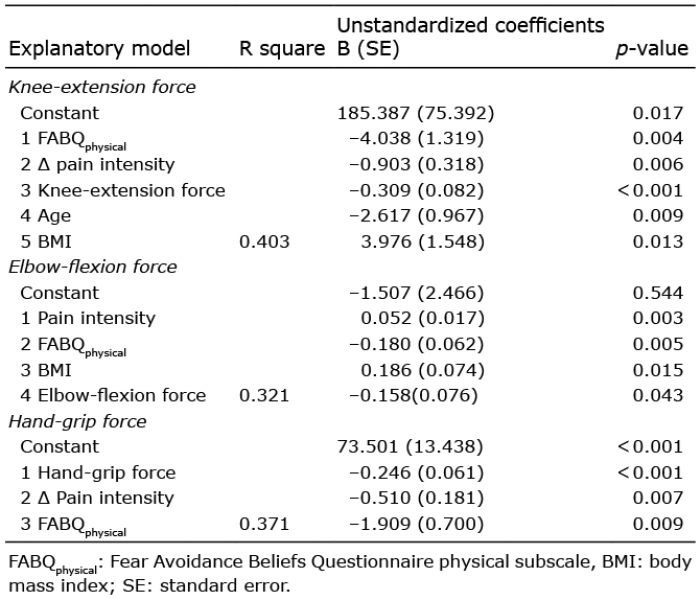 Click to show fullsize
Click to show fullsize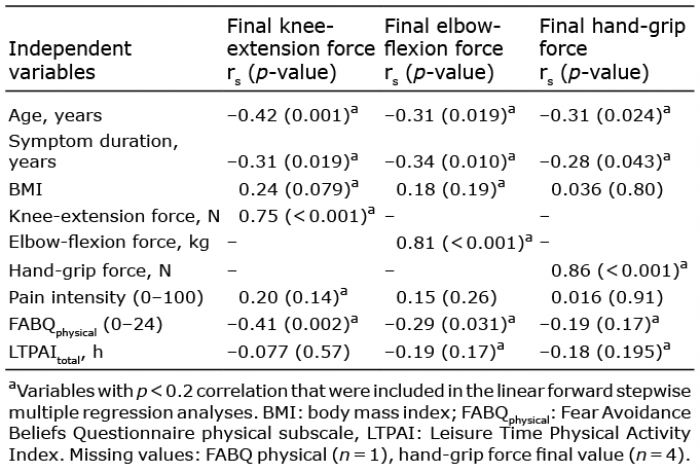 Click to show fullsize
Click to show fullsize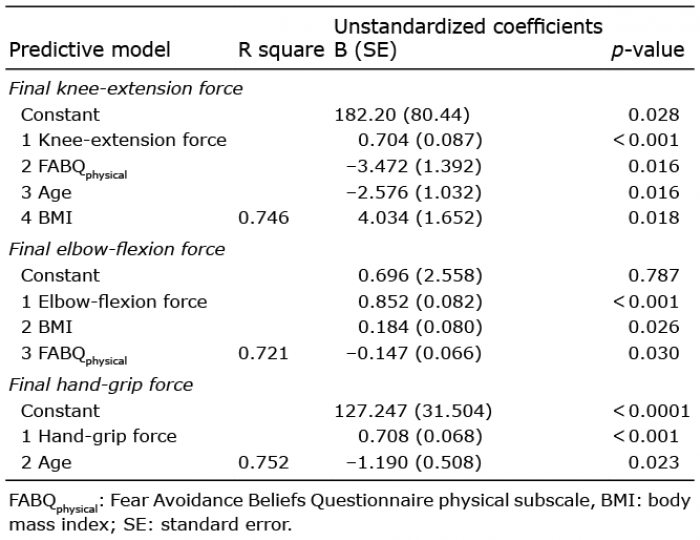 Click to show fullsize
Click to show fullsize