
From the 1Lifestyle and Health Research Group, Faculty of Health Care, Utrecht University of Applied Sciences, 2Center of Excellence in Rehabilitation Medicine, Brain Center Rudolf Magnus, University Medical Center Utrecht, and De Hoogstraat Rehabilitation, Utrecht, 3Department of Epidemiology and Biostatistics and the EMGO+ Institute for Health and Care Research, 4Department of Rehabilitation Medicine, MOVE Research Institute Amsterdam, VU University Medical Center, Amsterdam, and Department of Neurorehabilitation, Reade Center for Rehabilitation and Rheumatology, Amsterdam, and 5Revant Rehabilitation Centre Breda, Breda, The Netherlands
Objective: To systematically review and critically appraise the literature on measurement properties of cardiopulmonary exercise test protocols for measuring aerobic capacity, VO2max, in persons after stroke.
Data sources: PubMed, Embase and Cinahl were searched from inception up to 15 June 2016. A total of 9 studies were identified reporting on 9 different cardiopulmonary exercise test protocols.
Study selection: VO2max measured with cardiopulmonary exercise test and open spirometry was the construct of interest. The target population was adult persons after stroke. We included all studies that evaluated reliability, measurement error, criterion validity, content validity, hypothesis testing and/or responsiveness of cardiopulmonary exercise test protocols.
Data extraction: Two researchers independently screened the literature, assessed methodological quality using the COnsensus-based Standards for the selection of health Measurement INstruments checklist and extracted data on measurement properties of cardiopulmonary exercise test protocols.
Data synthesis: Most studies reported on only one measurement property. Best-evidence synthesis was derived taking into account the methodological quality of the studies, the results and the consistency of the results.
Conclusion: No judgement could be made on which protocol is “best” for measuring VO2max in persons after stroke due to lack of high-quality studies on the measurement properties of the cardiopulmonary exercise test.
Key words: stroke; maximal cardiopulmonary exercise test; VO2max; measurement properties.
Accepted Jun 2, 2017; Epub ahead of print Sep 1, 2017
J Rehabil Med 2017; 49: 00–00
Correspondence address: Harriet Wittink, Utrecht University of Applied Sciences Chair Lifestyle and Health Research Group Heidelberglaan 7, NL-3584 CS, Utrecht, The Netherlands. E-mail: harriet.wittink@hu.nl
Cardiopulmonary capacity (i.e. aerobic capacity or VO2max) is defined as the highest rate at which oxygen can be taken up and consumed by the body during intense exercise (1). Obtaining a valid measure of aerobic capacity in people after stroke is important for the purpose of determining exercise capacity, training prescription, treatment efficacy evaluation, and/or investigation of exercise-induced adaptations of the oxygen transport/utilization system (2). The current gold standard for the assessment of aerobic capacity is considered to be the maximal cardiopulmonary exercise test (CPET) with measurements of ventilation and gas exchange, for direct assessment of maximal oxygen uptake (VO2max). VO2max is the accepted indicator of aerobic capacity and reflects the limits of the cardiorespiratory system to respond to exercise. Peak oxygen uptake (VO2peak) reflects the highest amount of oxygen consumption attained during a test, but does not necessarily define the highest value attainable by the subject (3). Whereas VO2peak is probably a valid index for VO2max in healthy subjects (4), there is no evidence that this is the case in persons after stroke. The assessment of aerobic capacity in persons after stroke seems more challenging than in healthy subjects because they present with stroke-specific impairments, such as muscle weakness, fatigue, poor balance, contractures and spasticity, which can compromise CPET (5, 6). Marzolini et al. (7), for instance, reported that, at the start of an exercise training intervention, only 68.4% of CPETs (n = 98) provided sufficient information to prescribe exercise intensity in persons with chronic stroke, suggesting that many persons after stroke do not reach the limits of their cardiopulmonary system before training. In the search for a CPET protocol that allows persons after stroke to reach the limits of their cardiopulmonary system, a multitude of different protocols have been developed using treadmill exercise (6, 8), body-weight supported treadmill exercise (9), (recumbent) leg cycle ergometry (6, 10, 11) and recumbent stepper exercise (12).
However, little is known about the measurement properties of these different CPET protocols in persons after stroke. To guide further research on CPET protocols in persons after stroke and to be able to interpret changes in aerobic capacity after exercise interventions, the aim of this systematic review was to critically appraise the measurement properties of CPET protocols for measuring VO2max in persons after stroke and, if possible, make recommendations for the “best” CPET protocol to use.
A systematic review was performed in accordance with the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) methodology (13). The findings were reported according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines (14). PubMed, Embase and CINAHL databases were searched from inception until 15 June 2016, without language or date restrictions, in order to find all available studies on measurement properties of CPET protocols in persons after stroke.
The search was performed using the medical subject heading (MESH) terms and text words (or synonyms) for the construct of interest (maximal aerobic capacity OR VO2max,) AND population of interest (stroke OR cerebrovascular accident OR CVA OR brain ischemia). For measurement properties, a validated search filter for finding studies on measurement properties (15) was applied in PubMed, which was adapted for use in CINAHL and Embase. The full search is detailed in Appendix SI. In addition, bibliographies of included articles were searched manually for additional references. For “grey literature” the first 10 pages of Google Scholar were searched using the terms “maximal exercise test” and “cerebrovascular accident”.
The inclusion criteria were as follows: for the construct of interest and type of measurement: studies that directly measured VO2max during a CPET protocol using gas exchange by open-circuit spirometry, rather than indirect estimations, that evaluated at least 1 measurement property of a CPET protocol. Population: persons older than 18 years after stroke. Stroke was defined according to the World Health Organization (WHO) as “a syndrome of rapidly developing symptoms and signs of focal, and at times global, loss of cerebral function lasting more than 24 h or leading to death, with no apparent cause other than that of vascular origin” (16). Finally, only full-text original articles were included
Studies were excluded when a submaximal protocol was used to predict VO2max or when the only criterion for maximal testing was based on predicted maximal heart rate or a percentage of predicted maximal heart rate. Predicted heart rate was excluded since maximal heart rate response to exercise possesses wide variability (±12 beats per min) in the general population, which negatively impacts the ability to gauge subject effort by their heart rate response alone. The widespread use of beta-blocking agents in persons after stroke further complicates this issue by significantly blunting the maximal heart rate response in a disparate manner, negating the validity of the age-predicted maximal heart rate equation (17).
Eligibility criteria were applied independently by 2 reviewers (HW, IvdP) to screening titles and abstracts from all retrieved studies. Full-text review against inclusion criteria was performed of potentially eligible studies by the same 2 independent reviewers. Disagreement was resolved by joint review of the studies to reach consensus. Authors were contacted when relevant information was not available from the article.
Two reviewers (HW and OV) independently evaluated the methodological quality of the included studies using the COSMIN checklist (18). The COSMIN checklist is a standardized modular tool for evaluating the methodological quality of studies on measurement properties of health-related patient-reported outcomes. However, the checklist can also be used to evaluate the methodological quality of studies on other outcome measures (18).
The COSMIN checklist contains 12 boxes: 9 of which can be used to assess the methodological quality of studies on measurement properties, 2 contain general requirements (item response theory (IRT) methods and generalizability) and 1 assesses interpretability. Interpretability is not considered a measurement property, but it is considered an important requirement for the suitability of an instrument in research or clinical practice (18). Three measurement properties (internal consistency, structural validity, cross-cultural validity) were considered not relevant for CPET protocols. Six boxes on methodological quality were used to assess the quality of the studies regarding the CPET measurement properties: reliability, measurement error, content validity, criterion validity, hypothesis testing and responsiveness.
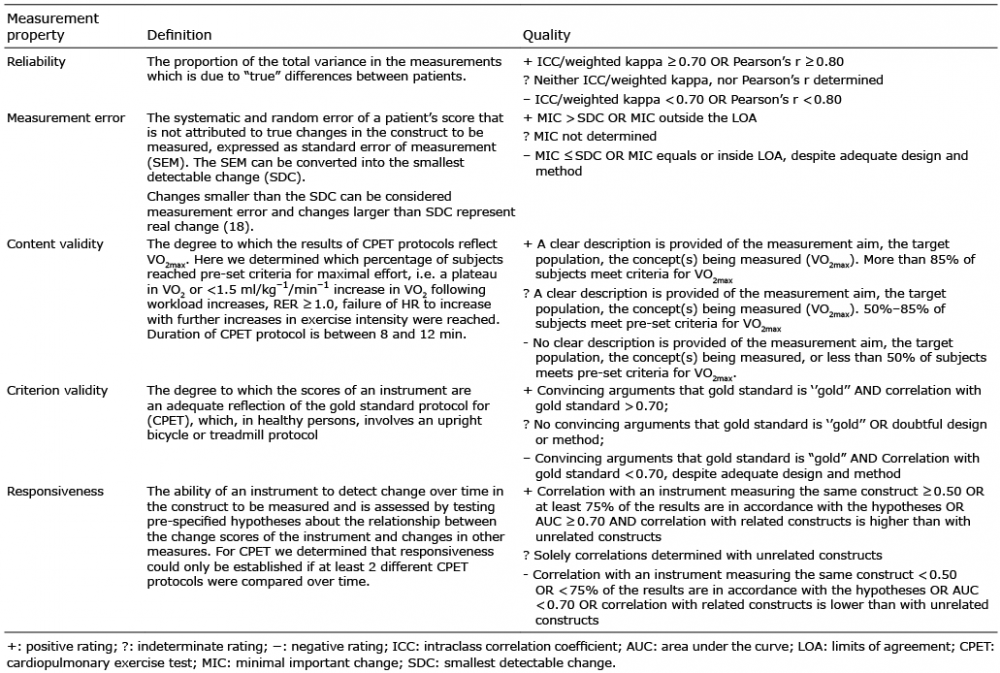
Measurement error of CPET protocols can be established by calculating standard error of measurement (SEM). The SEM represents the extent to which CPET measurements vary if CPET is repeated without any underlying change in the patient (19). The SEM can be converted into the smallest detectable change for an individual (SDCind), which reflects the smallest within-person change in score that, with 95% confidence, can be interpreted as a ‘’real’’ change, above measurement error, in 1 individual. For evaluative purposes, the SDC should be smaller than the minimal amount of change in VO2max that is considered to be clinically important (minimal important change; MIC) for an individual patient (20).
Content validity in this study was defined as the degree to which the result of a CPET protocol reflects VO2max. We therefore assessed whether a clear description of the measurement aim, the target population, the construct to be measured (VO2max) by the primary criterion (plateau VO2) and secondary criteria (respiratory exchange ratio (RER), age predicted maximum heart rate (APMHR)) and the percentage of persons achieving these criteria, were provided. The methodological quality of a study was downgraded if duration of CPET was not reported, as the recommendation is to use protocols with modest, equal increments in work rates to achieve an exercise duration of 8–12 min (17, 21).
The items of each box were rated with a 4-point scoring system; excellent, good, fair, and poor. In line with the COSMIN checklist guidelines, an overall score for the methodological quality was obtained by taking the lowest rating of any item in a box (“worst score counts”) (22). The methodological quality of a study was evaluated per measurement property.
The “Generalizability” box was used to evaluate general requirements: (i) whether the studies adequately described their samples in terms of age, sex, disease characteristics, setting, country, and language; (ii) whether they used adequate selection procedures; and (iii) whether acceptable missing response rates were applied. Missing response rates were defined in this study as the percentage of persons who were unable to complete the CPET protocol after inclusion. This box was used to generate a table on the characteristics of the study populations.
To assess whether the results of the measurement properties were positive, negative, or indeterminate, we applied quality criteria for good measurement properties (Table I) (20). One rater (HW) applied the quality criteria.
Table I. Quality criteria for measurement properties. Adapted from Terwee et al. (20)
A “best-evidence” synthesis was performed to rate the quality of the CPET protocols using the criteria in Table II. The possible levels of evidence for a measurement property are “strong”, “moderate”, “limited”, “conflicting” or “unknown”. Best-evidence synthesis was derived taking into account the methodological quality of the studies (COSMIN score; excellent, good, fair, and poor), the results (positive, indeterminate, negative) and the consistency of the results (Table II). Measurement properties from studies that were rated as poor quality were not included the best-evidence synthesis (23).
Table II. Best-evidence synthesis. Adapted from Terwee et al. (20)
To quantify inter-rater agreement concerning the COSMIN methodological quality assessment, a linear weighted Cohen’s kappa (κ) was calculated on the original items of each COSMIN box scores of the 2 reviewers (before discussion). Any disagreements in scoring were resolved after discussion.
The following interpretation was used: 0.01–0.20 means slight agreement; 0.21–0.40 means fair agreement; 0.41–0.60 means moderate agreement; 0.61–0.80 means substantial agreement; and 0.81–0.99 means almost perfect agreement (24). Where possible, SEM, and SDCindividual were calculated from reported test-retest standard deviations (SDs) and intraclass correlation coefficients (ICCs).
Standard error of measurement (SEM) was calculated using the following formula: SEMagreement σ√ (1–ICC2,1), where σ is the pooled standard deviation of test and retest scores. SEM can be calculated as SEMagreement or SEMconsistency (20). SEMagreement takes the systematic difference between test and retest into account, while the SEMconsistency ignores systematic differences (20). We therefore used SEMagreement in all calculations. The SEM can be converted into the smallest detectable change (SDC) (SDC = 1.96*√ 2 *SEM), which reflects the smallest within- person change in score that, with 95% confidence, can be interpreted as a ‘’real’’ change, above measurement error, in one individual (SDCind).
The COSMIN scoring system used in this review was initially developed for assessing the quality of research into measurement properties of patient-reported outcomes (PROMs) and defines a minimum adequate sample size as 30 (fair) and adequate sample size as 100 (excellent). In this review we expected high reliabilities, because in persons with cardiac or respiratory disease the test-retest reliability was shown to be ICC = 0.95 (25–27). To determine whether sample size was adequate for calculating ICC values in the test-retest trials, we ran a simulation with 100,000 replications under the assumption that “true” ICC values would be approximately 0.95. We wanted to determine the sample size large enough to detect observed ICC values larger than 0.90 with 80% probability. The simulation we ran resulted in a required sample size of n=5 to achieve an 82% probability of measuring an ICC value >0.90.
This is assuming that the data are distributed normally. This assumption might not be met with such a small sample size. However, we decided to accept larger sample sizes than n = 5 as adequate (“fair”) for COSMIN scoring purposes. According to our simulation a sample size of n = 10 results in a 95% probability of measuring an ICC > 0.90, which we considered good, and a sample size of n = 15 yielded a 99% probability of measuring an ICC > 0.90, which we considered excellent.
The selection procedures are summarized in Fig. 1.
Fig. 1. PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram.
The search in Medline, Embase and Cinahl resulted in 1,644 citations. After removing duplicates (n = 472), 1,172 titles and abstracts were screened by 2 reviewers independent of each other for inclusion criteria, after which 1150 citations were excluded. The full texts of the remaining 22 studies were examined in detail by the 2 reviewers. One study was retrieved from reference lists (28), increasing the total to 23 included studies. Of these 23 studies 14 did not meet the inclusion criteria; 1 was an abstract only (29); 8 studies reported on a submaximal test or used the attainment of (a percentage of) maximal predicted heart rate as their only criterion (28, 30–36), and in 3 studies no measurement properties were reported (37–39), 1 study included the same sample as an earlier (included) study (9) and 1 study did not report criteria for determining VO2max (40). Searching the grey literature through the first 10 pages of Google Scholar using “maximal exercise test” and “stroke” yielded no additional articles or additional information.
Finally, 9 studies met all inclusion criteria and were included for review. The 9 studies included 2 studies with a test-retest design (6, 41), 1 RCT (10), one prospective cohort design (5), 3 cross-sectional feasibility studies (11, 42, 43), one retrospective study (7) and one within-subject design study (12).
The 9 studies reported on 9 different CPET protocols; 2 upright bicycle protocols with workload increments of 10 W/min (10) or 20 W/min (6) in persons with chronic stroke, 1 upright bicycle protocol with increments of 5 W/min in persons with acute stroke (42), 1 semi-recumbent bicycle protocol with increments of 5 W/min in persons with acute stroke (11), 2 treadmill protocols, both based on self-selected speed with different % inclines/min; 1 with body weight support (5) and 1 without (41), 1 robotics assisted tilt table (43), 1 recumbent stepper (12) and in 1 study a combination of protocols was used (7) in persons with subacute or chronic stroke.
Test-retest reliability was tested in 5 studies (5, 6, 10, 11, 41). Three studies tested test-retest reliability in a subsample of their persons who were part of a larger study (5, 10, 11). One of the 5 studies assessed measurement error (6) and in 1 study measurement error could be calculated from the available data (11). No studies explicitly mentioned content validity, but 6 studies reported on the feasibility of the test protocol (5, 7, 11, 41–43), which provides some information on content validity. In one study criterion validity was assessed (12). No studies were found in which responsiveness was measured or where hypothesis testing was performed.
Study characteristics are described in Table III.
Table III. General characteristics of included studies
Out of the 9 studies, 6 included persons with chronic stroke and 3 included persons early after stroke (mean days post-stroke 9.9 (standard deviation (SD) 2.0) (42), 17.6 (SD 2.2) (11) and 26.0 (SD 8.8) (5)). Sample sizes ranged from 6 (5) to 98 (7) persons. All studies, except one (10) specified where testing took place. Six studies described the method to select their subjects (random, consecutive or convenience), in 3 studies this was unclear (5, 41, 43).
All studies included persons with mild-to-moderate impairments, except for Billinger et al. (12), who included persons with mild-to-severe impairments according to mild-to-severe lower extremity Fugl-Myer test scores, and Shaengsuwan et al. (43) who included dependent ambulatory persons with a mean Functional Ambulation Score (FAC) score of 1.8.
The inter-rater agreement of the independent methodological quality assessment of included studies was linear weighted kappa = 0.86 (95% confidence interval (95% CI) 0.77–0.96). This was interpreted as almost perfect agreement (24). Disagreement was mainly due to errors in interpretation and was easily resolved using a consensus method between the 2 raters.
Among the 5 test-retest studies (total n = 116), 2 studies reported the evaluation of the test-retest reliability of CPET as the main purpose of their study (6, 41). In these 2 studies sample sizes ranged from 12 (6) to 53 (41) persons with chronic stroke (> 6 months), with mean ages ranging from 62.5 (SD 8.6) (6) to 64 (8) years. The other 3 studies (5, 10, 11) reported on testing a subsample of their subjects within a larger study and included sample sizes ranging from n = 6 (5) to n = 25 (10) and persons with acute (5, 11) and chronic stroke (10).
Five different protocols were found, including treadmill (6, 41), body weight supported treadmill (5) and (recumbent) leg cycle ergometry (6, 10, 11).
ICC values were higher than 0.90 for 3 studies (5, 6, 10) 1 study reported an ICC of 0.50 (11) and 1 study reported an undefined correlation of 0.92 (41).
The methodological quality of the reliability studies was rated as poor (5, 11), fair (6, 41) and good (10). In all studies there was ambiguity about independent administrations. None of the studies specified whether subjects were stable in the interim period. The reported interim period was 1–4 days (11), 2 days (10), 3–4 days (5) and 1 week (41). One author did not report the interim time-period (6).
Two out of the 5 studies reported on whether test conditions were similar for both measurements (11, 41). Only 1 study explicitly reported similar test conditions using the same equipment and raters for both tests (11). The main methodological flaws included inappropriate or not-reported time intervals between tests (6, 11) and selection bias (5, 11).
Due to poor methodological quality 2 of the 5 studies were excluded from the best-evidence synthesis (5, 11). In the 3 remaining studies 3 different protocols were used; 2 different upright bicycle protocols (6, 10), and a treadmill protocol (41). As the 2 bicycle protocols used similar pedalling rates and increases in Watts per min, we felt we could combine the results in an evidence synthesis, and concluded there is moderate evidence for positive reliability in upright bicycle protocols in persons with chronic stroke. In addition, there is limited evidence for positive reliability for a treadmill protocol (41), based on one study of fair quality (Table IV).
Table IV. Methodological quality/measurement properties and best evidence
Of the 5 reliability studies only one reported on measurement error in terms of standard error of measurement (SEM) (6). SDCindividual was calculated from the SEM given by Eng et al. (6), although we were not able to verify whether SEM was calculated correctly, as test-retest data were not given in the paper. We were able to calculate SEM and SDCindividual for one more study based on the pooled SD of test and retest SD (11). Mean SEM varied between 0.36 ml/kg/min (11) and 1.0 ml/kg/min (6). SDCindividual ranged from 1.0 ml/kg/min in persons with sub-acute stroke (11) to 2.77 ml/kg/min in persons with chronic stroke (6).
One study was rated of fair quality (6) due to not reporting of the time interval between measurements. Four studies were rated as poor due to not calculating any measurement error, as we would expect in a reliability study.
As we could not find any research on minimal clinically important change (MIC) in persons after stroke, we set the MIC for oxygen uptake at 1 ml/kg/min based on the study by Keteyian et al. (44), which found that in persons with coronary heart disease VO2peak is a strong predictor of all-cause death, with every 1 ml/kg/min increase in VO2peak associated with an approximate 15% decrease in risk of death. The MIC was smaller than the SDCindividual in one study of fair quality (6) and equal to the SDCindividual in one poor-quality study (11). Excluding the poor-quality study from the best-evidence synthesis, there is limited evidence for negative measurement error in an upright bicycle protocol (Table IV).
Out of the 9 studies, 6 reported the criteria for determining the attainment of VO2max and the percentage of persons that reached these criteria (5, 7, 11, 41–43) (Table V). None of these studies set out to explicitly test content validity, but they set out specifically to determine the feasibility of a protocol.
Table V. Criteria for construct validity cardiopulmonary exercise test (CPET) protocols
Criteria for determining VO2max were not consistent across studies (see Table V).
Two studies did not report on the formula used for determining APMHR (11, 41) and 2 studies used an adjusted formula for subjects taking beta-blockers (5, 7). Only one study reported on the duration of testing (5).
The quality of all 6 studies was rated as good. In these studies consistently a clear description was provided of the measurement aim, the target population and the concept(s) being measured (VO2max). Subject achievement of pre-set criteria for VO2max was 87.5% in 1 study (43), 50–80% in 3 studies (5, 11, 42) and less than 50% in 2 studies (7, 41) (n = 151). Main methodological flaws were including systolic blood pressure > 200 mmHg as a criterion for attainment of VO2max (5), incomplete reporting on criteria set for determination of VO2max (41) and not reporting on duration of testing (7, 11, 41–43).
The studies could not be combined due to the difference between the study protocols; therefore we determined the evidence for content validity per protocol.
In 3 good-quality studies (5, 11, 42) (n = 83) we rated the evidence for content validity as unknown for a body weight supported treadmill protocol, a semi-recumbent, and an upright bicycle protocol. In 2 good quality studies (7, 41) (n = 151) in which less than 50% of subjects achieved criteria for VO2max, we found moderate evidence for negative content validity of a treadmill protocol (8) and protocols chosen by testing staff (7).
In 1 study of good quality 87.5% of subjects met pre-set criteria for VO2max. However, the sample size was small (n = 8), we therefore downgraded the evidence to limited evidence for positive content validity of a robotics-assisted tilt table in dependent ambulatory persons after stroke (43) (Table IV).
Only one study determined criterion validity. A semi-recumbent stepper protocol was compared with an upright bicycle ergometer protocol (gold standard protocol) (12). The methodological quality of this study for criterion validity was rated as fair due to the small sample size (n = 11).
The level of evidence for criterion validity was provided by one study of fair quality (12). With a correlation of r = 0.91 between VO2peak obtained by the 2 protocols, the criterion validity measurement was rated as positive. This study therefore provided limited evidence of positive criterion validity of the recumbent stepper protocol compared with a cycle protocol in persons with chronic stroke with mild-to-severe impairments.
The results of this review reveal a lack of high-quality studies into the measurement properties of CPET protocols for persons after stroke. Nine studies were found, which reported 9 different CPET measurement protocols. Most studies reported on only one measurement property. No studies were found on hypothesis testing or responsiveness. In most of the studies in this review a substantial proportion of subjects were reported to not reach the limits of their cardiopulmonary systems during the CPET protocol. Although authors agreed on a VO2 plateau as a primary criterion to determine the attainment of VO2max, we found substantial variation between secondary criteria. As a plateau in VO2 is often not found, secondary criteria are frequently relied upon to determine attainment of VO2max, which means that these criteria directly impact on the content validity of CPET protocols.
At present, due to the heterogeneity of CPET protocols and secondary criteria, as well as the scanty information on measurement properties of CPET protocols, we are unable to make recommendations as to which protocol to use to “best” measure VO2max in persons after stroke. However, for readers interested in recommendations for clinical practice, we refer to our recent systematic review (45).
Test-retest reliability depends on daily or weekly fluctuations in VO2max and is based on the assumption that no real change in VO2max occurs between tests. Subjects who have undergone maximal exercise testing will need time to recover from this exhaustive work. Although there is no research available to guide an appropriate time interval between tests in persons with stroke, we considered 1 day (11) as too short to allow these deconditioned individuals to recover from exhaustive testing. Although the CPET protocols used were diverse, and the time interval varied between 1 and 7 days, ICC values between the reliability studies were remarkably similar. There was moderate evidence for positive reliability for upright bicycle CPET protocols, consistent with studies on healthy adults and in persons with cardiac or respiratory disease (46–48). The one exception was the study by Tang et al. (11) reporting an ICC of 0.50. This study also reported the smallest SD of VO2peak values, representing a fairly homogeneous sample of subjects, which probably also explains the low ICC value found in this study. This homogeneity might be the result of selection bias (taking the “best” subjects for test-retest). We found moderate evidence for positive reliability in CPET in 2 upright bicycle protocols (6, 10) in persons with chronic stroke. However, CPET with an upright bicycle protocol may not be able to distinguish between clinically relevant change and measurement error in individual persons after stroke.
Measurement error can occur due to technical factors, natural variation in the subject, variation in the measurement process, or a combination of these factors (1, 49).
Individual measurement error (SDCindividual) ranged from 1.0 ml/kg/min in persons with sub-acute stroke (11) to 2.77 ml/kg/min (6) in persons with chronic stroke and was equal to or larger than the minimal clinical important change (MIC) we set at 1 ml/kg/min based on the available literature. Therefore, clinically relevant changes cannot be distinguished from measurement error in individual persons with 95% confidence (50). It would thus be helpful if future studies, instead of reporting group mean improvements and statistical significance, would report on the percentage of individual persons who achieved a clinically important change in aerobic capacity.
Secondary criteria for the determination of attainment of VO2max directly impact content validity. Although all studies reported a VO2 plateau as the gold standard for attainment of VO2max, secondary criteria varied substantially. For RER a range of 1.0–1.15 was used, but RER values greater than 1.1 are probablytoo high for persons after stroke as they tend to be older. For instance, the 2 studies using RER > 1.1 reported 91% (41) and 61.8% (7) of their sample (mean age 60+) to not reach the limits of their cardiopulmonary systems (VO2max), despite reported maximal effort. Edvardsen et al. (51) report RER to decline by age and recommend using a RER of ≥ 1.05 for 50–64-year-olds and RER ≥1.0 for those 65 years and older for both males and females. We propose to adopt these criteria.
We found only one study in which protocols were compared to determine which protocol is most valid in measuring VO2max in persons after stroke. Billinger et al. (12) compared a semi-recumbent stepper protocol with an upright bicycle ergometer protocol in persons with mild to severe impairments, and found that VO2peak values were significantly higher for the semi-recumbent stepper protocol, although RER values (both RER = 1.1 (0.1)) were not significantly different. Unfortunately, they did not report on the percentage of persons that attained criteria for VO2max in either protocol.
We struggled with the definition of “content validity” as given by Terwee et al. (20), as what we wanted to know was whether actual CPET results reflected criteria set for VO2max. As there are no criteria for content validity assessment of CPET, we determined our own. These criteria included the reporting of the duration of CPET as we feel this helps in interpreting CPET results. Using this criterion resulted in lower quality scores for 3 of the 6 content validity studies that did not report duration of testing (5, 7, 11). One could consider this too strict, as, formally, duration of testing is not a criterion for determining VO2max.
We were unable to find what constitutes a MIC in aerobic capacity in persons after stroke. Therefore we used the findings by Keteyian et al. (44), as these were based on persons with coronary heart disease, and we felt this population resembled the stroke population. A recent systematic review (45) concluded that most CPET studies do not or insufficiently adhere to existing cardiopulmonary guidelines. Of the 9 included studies 8 reported adhering to ACSM guidelines for contraindications to maximal exercise testing and for termination criteria. Only Billinger et al. (29) did not refer to any guideline. Most studies did not report on pre-exercise testing or abstinence from alcohol, caffeine or tobacco prior to testing. This may have affected the reproducibility and validity of the CPET protocols.
Although we performed a comprehensive search for studies on measurement properties of CPET protocols, we may have missed studies, especially sub-studies on measurement properties embedded in larger (clinical) studies.
This review reveals the lack of high-quality measurement property studies on CPET protocols for persons after stroke. Our findings show the urgent need for further measurement property studies on CPET protocols in persons after stroke. We need to find consensus on which secondary criteria to use in CPET protocols in persons after stroke to determine attainment of VO2max. Given the reported difficulty of measuring VO2max in persons after stroke, we may need to consider an alternative; for instance, the determination of the ventilatory anaerobic threshold (VAT), or the respiratory compensation point (RCP). The VAT and RCP are recommended as an appropriate target intensity level for the prescription of exercise as they are effort-independent measures and maximum testing is not necessary. Measuring VAT in persons after stroke is feasible for the majority of subjects, as evidenced by the reports of 5 studies (7, 11, 42, 43, 52). A recent study has found the determination of VAT to have good reliability (ICC3,2 = 0.87, 95% CI 0.80–0.95) in persons after stroke (52). RCP has been shown to be identifiable in 96% of persons after stroke and to have reasonably good reliability (ICC3,1 = 0.77 (95% CI 0.24, 0.87)) (53).
Further high-quality research is needed into the measurement properties of different CPET protocols in the acute and, more severely impaired, chronic population of persons with stroke.
This study was funded by Utrecht University of Applied Sciences. The authors would like to thank Jurgen Mollema MSc for his support with constructing the search string and searching the databases.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize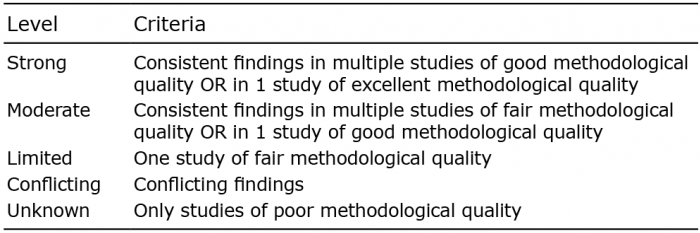 Click to show fullsize
Click to show fullsize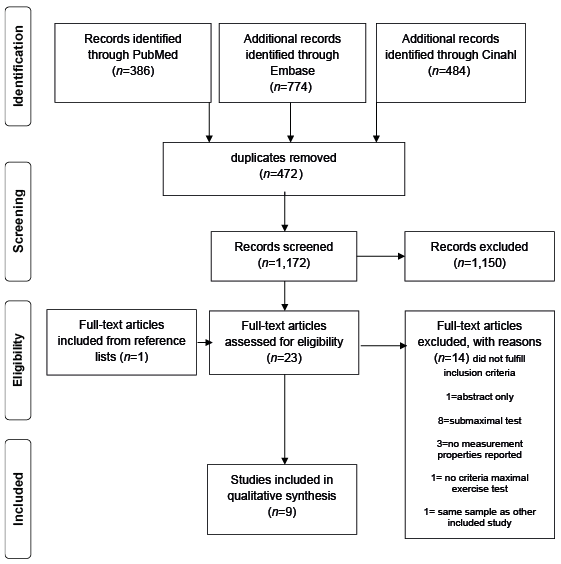 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize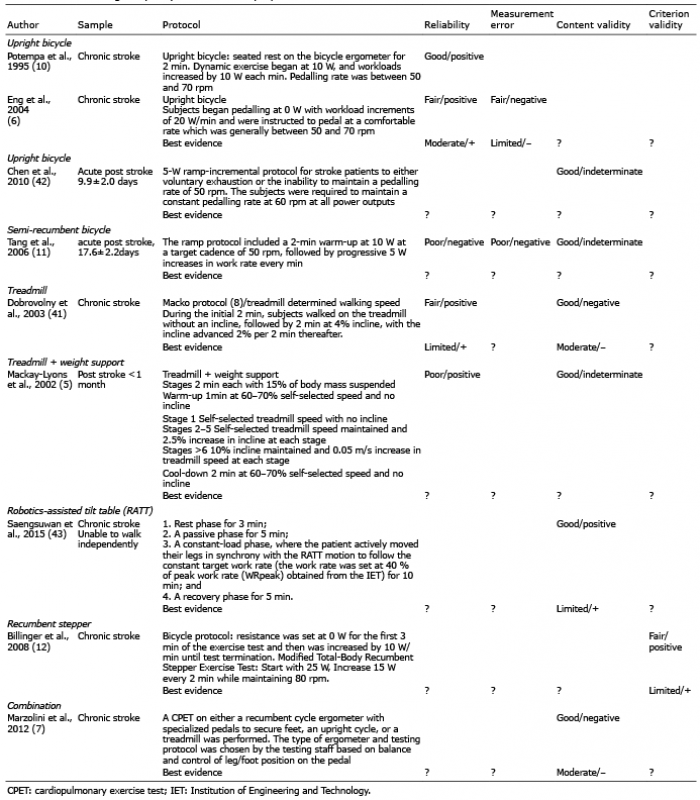 Click to show fullsize
Click to show fullsize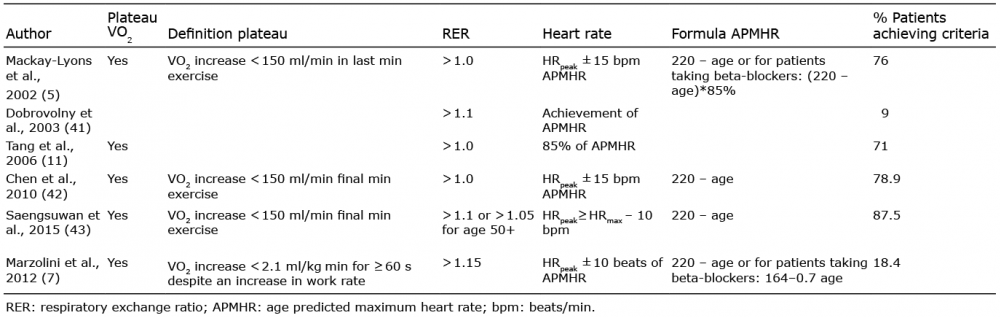 Click to show fullsize
Click to show fullsize