
From the Department of Rehabilitation Medicine, Yokohama City University Medical Center, Minami Ward, Yokohama, Japan
Objective: To assess the prevalence of sarcopaenia and the association between sarcopaenia, activities of daily living, and dysphagia in cancer patients who require rehabilitation.
Methods: A cross-sectional study was performed in 83 consecutive cancer patients referred to the Department of Rehabilitation Medicine. Skeletal muscle index was calculated as total psoas muscle area assessed via abdominal computed tomography divided by height squared. Sarcopaenia was diagnosed using the Asian Working Group for Sarcopenia criteria. Activities of daily living were evaluated with the Barthel Index. Dysphagia was assessed with the 10-item Eating Assessment Tool (EAT-10).
Results: Study participants were 50 males and 33 females (mean age 71, standard deviation 12 years). Sarcopaenia was observed in 66 (80%) patients. The median Barthel Index score was 55 (interquartile range: 25–75). Thirty-five (42%) patients were diagnosed as having dysphagia. Logistic regression analysis of dysphagia adjusted for sarcopaenia, Barthel Index score, age, and reason for hospitalization showed that sarcopaenia (odds ratio (OR) 3.616; 95% confidence interval (95% CI) 0.926–14.114; p = 0.064) and Barthel Index score (OR 0.984; 95% CI 0.966–1.002; p = 0.073) did not reach statistical significance.
Conclusion: The prevalence of sarcopaenia in cancer patients who require rehabilitation is very high. The power of this study was too low to observe a significant association between sarcopaenia and dysphagia.
Key words: activities of daily living; cancer; dysphagia; rehabilitation; sarcopaenia.
Accepted May 30, 2017; Epub ahead of print Jun 30, 2017
J Rehabil Med 2017; 49: 00–00
Correspondence address: Wakabayashi Hidetaka, Department of Rehabilitation Medicine, Yokohama City University Medical Center, 4-57 Urafune-chou, Minami Ward, Yokohama, Japan 232-0024. E-mail: noventurenoglory@gmail.com
Sarcopaenia and dysphagia are important issues in cancer. Sarcopaenia is characterized by an age-related loss of muscle mass, strength and function. The prevalence of sarcopaenia in cancer patients ranges between 27.3% and 66.7% (1). A systemic review demonstrated that sarcopaenia is associated with poor survival in cancer patients (2). Dysphagia is common in patients with head and neck cancer and oesophageal cancer, and may also occur in association with other cancers, such as lung, gastric, colon, and prostate cancer (3). Dysphagia is associated with severe complications, such as aspiration pneumonia and choking. Furthermore, both sarcopaenia and dysphagia are associated with lower quality of life (4). Therefore, sarcopaenia and dysphagia are essential topics in cancer rehabilitation.
The association between sarcopaenia and dysphagia has been investigated primarily in older people, but not in cancer patients. Sarcopaenic dysphagia is characterized by a loss of both swallowing muscle mass and function, and whole-body muscle mass and function (4). A prospective cohort study demonstrated that 26% of older inpatients without dysphagia who had restricted oral intake for more than 2 days developed dysphagia (5). Whole-body sarcopaenia, low body mass index (BMI), and low activities of daily living (ADL) were independent predictors for the development of dysphagia, with all patients who developed the condition having whole-body sarcopaenia. The main cause of development of dysphagia is probably sarcopaenia (5). One study in cancer patients demonstrated that skeletal muscle mass is associated with severe dysphagia, and decreased ADLs may also be associated with severe dysphagia (3). However, this study did not investigate handgrip strength, gait speed, or sarcopaenia. Furthermore, no studies have investigated the prevalence of sarcopaenia and the association between sarcopaenia, ADLs, and dysphagia in cancer patients who require rehabilitation.
Therefore, the aim of the study was to determine the prevalence of sarcopaenia and the association between sarcopaenia, ADLs, and dysphagia in cancer patients who require rehabilitation.
A cross-sectional study was performed in consecutive cancer patients who had been admitted to the Yokohama City University Medical Center and referred to the Department of Rehabilitation Medicine between March 2015 and February 2016. All patients were prescribed physical therapy 5 times a week at the bedside or gymnasium, and some patients were prescribed occupational therapy and/or speech therapy. Patients diagnosed with cancer were referred to the Department of Rehabilitation Medicine by attending physicians, and evaluations included in the study were then carried out. The following patients were excluded: (i) patients who declined to participate in the study; (ii) patients with brain or spinal tumours and/or neuromuscular diseases, because paralysis can affect sarcopaenia, ADLs, and dysphagia; (iii) patients who had not undergone abdominal computed tomography (CT) for clinical purposes during the period 60 days before referral to one week after referral. This study was approved by the ethics committee of Yokohama City University Medical Center. All participants provided informed consent prior to enrolment.
Sarcopaenia was diagnosed using the Asian Working Group for Sarcopenia criteria (6). Skeletal muscle mass was assessed by measuring the cross-sectional area of the right and left psoas muscles via abdominal CT (Slice-O-Matic software v.5.0; Tomovision, Magog, Quebec, Canada) at the caudal end of the third lumbar vertebra (3). Muscles were quantified using a Hounsfield unit range between −29 and 150. Physical therapists who measured the psoas muscle area were blinded to information on ADLs and dysphagia. Skeletal muscle index was calculated by dividing the total psoas muscle area by height squared. Cut-off values for low skeletal muscle mass were 6.36 cm2/m2 for men and 3.92 cm2/m2 for women (7). Cut-off values for low handgrip strength were 26 kg for men and 18 kg for women (6). Low physical function was defined as usual gait speed <0.8 m/s (6).
Dysphagia was assessed by the 10-item Eating Assessment Tool (EAT-10) (8). The EAT-10 scores each item from 0 to 4, with a score of 0 indicating no problem and a score of 4 indicating a severe problem. An EAT-10 score ≥ 3 is considered abnormal and indicates the presence of swallowing difficulties. The reliability and validity of the EAT-10 was confirmed (8, 9). In our previous study, people who could not respond to the EAT-10 were likely to have dysphagia (9). Therefore, patients who could not respond to the EAT-10, or had a score ≥ 3, were diagnosed as having dysphagia. Cancer sites were divided into pharyngeal and oesophageal vs others, because pharyngeal and oesophageal cancers organically cause dysphagia (3).
ADLs were assessed with the Barthel Index (10). Site of cancer, reason for hospitalization, the Mini Nutritional Assessment-Short Form (MNA-SF) (11), body mass index (BMI), serum albumin, haemoglobin, C-reactive protein, number of days from admission to physical therapy, and number of days from physical therapy to discharge were also evaluated.
A sample size calculation was performed using Power and Sample Size Calculation software version 3.0 (http://biostat.mc.vanderbilt.edu/twiki/bin/view/Main/PowerSampleSize). In our previous study the proportion of moderate or severe dysphagia patients in the low skeletal muscle mass and normal skeletal muscle mass groups was 0.32 and 0.08, respectively (12). In order to detect this difference in proportions (i.e. 0.24) between the 2 groups at a ratio of 1:1, 42 patients in both groups are needed to achieve a power (1–β) of 0.8 at a significance level (α) of 0.05. Because we assumed we would be able to recruit 100 cancer patients over a 1-year period, the duration of the current study was set at 1 year.
Statistical analyses were performed using IBM Statistical Package for the Social Sciences (SPSS) version 24 software (IBM Corporation; Armonk, New York, USA). Continuous data were expressed as the mean and standard deviation (SD) and ordered categorical data were reported as the median and interquartile range. The χ2 test, Fisher’s exact test, t-test, and Mann–Whitney U test were used to analyse differences between patients with and without sarcopaenia and dysphagia. Logistic regression analysis was conducted to examine whether sarcopaenia and Barthel Index score were independently associated with dysphagia. The dependent variable was dysphagia, and the independent variables were age, reason for hospitalization, presence or absence of sarcopaenia, and Barthel Index score. A p-value < 0.05 was considered statistically significant, with no adjustments for multiple comparisons being made.
During the research period, 116 cancer patients requiring rehabilitation were referred to the Department of Rehabilitation Medicine, and evaluations carried were out. Three patients who declined to participate in the study, 12 patients who had brain or spinal tumours and/or neuromuscular diseases, and 18 patients whose abdominal CT scans were not available were excluded. The remaining 83 patients participated in the study. Cancer types included lung cancer (n = 14), gastric cancer (n = 8), colon cancer (n = 7), pharyngeal cancer (n = 6), leukaemia (n = 6), breast cancer (n = 5), malignant lymphoma (n = 5), oesophageal cancer (n = 4), bladder cancer (n = 4), pancreatic cancer (n = 3), prostate cancer (n = 3), multiple myeloma (n = 3), ovarian cancer (n = 3), bone cancer (n = 2), kidney cancer (n = 2), and other (n = 5). Occupational therapy and speech therapy were performed in 8 and 9 patients, respectively.
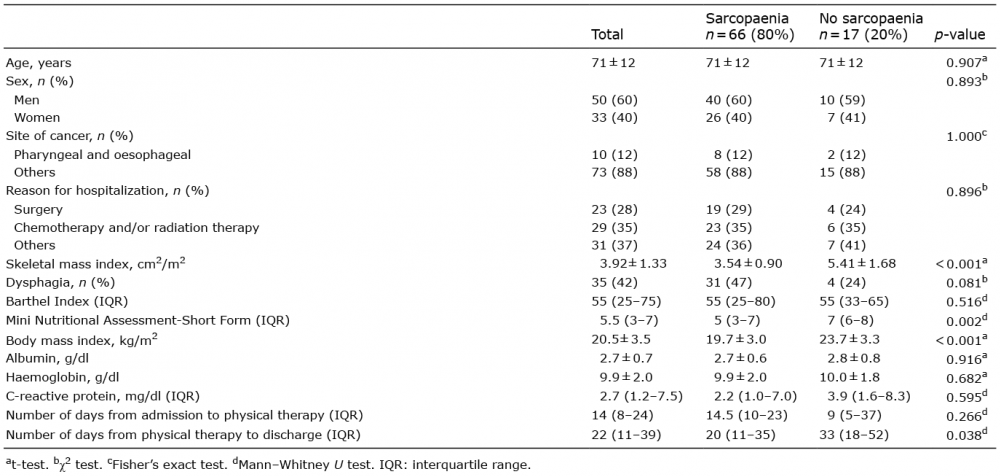
Table I shows the results of the comparative tests for differences between patients with and without sarcopaenia. Sixty-six (80%) patients were diagnosed with sarcopaenia due to low skeletal muscle mass and low handgrip strength and/or low gait speed. Thirty-five (42%) patients were diagnosed with dysphagia due to an EAT-10 score ≥ 3 (n = 20) or inability to respond to the EAT-10 (n = 15). All patients with pharyngeal or oesophageal cancer had dysphagia; thus, the prevalence of dysphagia in these patients was higher than that of patients with other types of cancer. Sixty-two (76%) patients were diagnosed with malnutrition by the MNA-SF.
Table I. Results of comparative tests for differences between patients with and without sarcopaenia
A greater proportion of patients with sarcopaenia had dysphagia than those without sarcopaenia, although this difference was not statistically significant (p = 0.081). We calculated the effect size between the presence of dysphagia and sarcopaenia and showed that the power was 0.469, indicating the study had low power.
We could not include the cancer site as an independent variable in the logistic regression analysis because all patients with pharyngeal and oesophageal cancers had dysphagia. The logistic regression analysis became unstable when we included the cancer site. Logistic regression analysis showed that older age (B = 0.53; standard error (SE) 0.026; odds ratio (OR) 1.054; 95% confidence interval (95% CI) 1.002–1.109; p = 0.041) and reason for hospitalization; surgery (B = 1.601; SE 0.679; OR 4.959; 95% CI 1.310–1.8.779; p = 0.018) were associated independently with dysphagia (Cox-Snell R2, 0.245; Nagelkerke R2, 0.329). Sarcopenia (B = 1.285; SE 0.695; OR 3.616; 95% CI 0.926–14.114; p = 0.064) and Barthel Index score (B = –0.016; SE 0.009; OR 0.984; 95% CI 0.966–1.002; p = 0.073) did not reach statistical significance in the logistic regression analysis.
We identified 2 issues regarding the prevalence of sarcopaenia and associations between sarcopaenia, ADLs, and dysphagia in cancer patients who required rehabilitation. First, the prevalence of sarcopaenia in cancer patients who required rehabilitation was very high. Secondly, both sarcopaenia and ADLs were possibly associated with dysphagia; however, this relationship was not statistically significant.
The prevalence of sarcopaenia in cancer patients who require rehabilitation appears to be very high. In this study, the mean age was 71 years. The median number of days from admission to physical therapy was 14, indicating the occurrence of hospital-associated deconditioning and activity-related sarcopaenia during hospitalization. Furthermore, 76% of patients were malnourished, indicating the presence of nutrition-related sarcopaenia in some patients. Moreover, cancer and cancer treatment can cause disease-related sarcopaenia. Therefore, rehabilitation in cancer patients can be complicated by age-, activity-, nutrition-, and disease-related sarcopaenia, resulting in a very high prevalence of sarcopaenia. The prevalence of sarcopaenia during rehabilitation among older adults is 50% (13). For patients with multiple complicating causes of sarcopaenia, rehabilitation nutrition is useful for eliciting maximum function (4).
Rehabilitation nutrition is defined such that it: (i) evaluates holistically by the International Classification of Functioning, Disability and Health including the presence and causes of nutritional disorders, sarcopaenia, and excess or deficiency of nutrient intake; (ii) conducts rehabilitation nutrition diagnosis and goal setting; and (iii) elicits the highest body functions, activities, participation, and quality of life (QOL) achieved by improving nutritional status, sarcopaenia, and frailty using “nutrition care management that considers rehabilitation” and “rehabilitation that considers nutrition” in people with a disability and frail older people (14). Rehabilitation nutrition is provided by a rehabilitation nutrition care process that includes assessment and diagnostic reasoning, diagnosis, goal setting, intervention, and monitoring (14).
Although sarcopaenia and ADL are possibly associated with dysphagia in cancer patients who require rehabilitation, this study was underpowered to detect this relationship. The power to detect a statistically significant association between sarcopaenia and dysphagia was low (0.469). One reason for this low power was the high prevalence of sarcopaenia in cancer patients who required rehabilitation. If the ratio of sarcopaenia patients to patients without sarcopaenia had been 1, the power would have been 0.599. Another reason for the low power was small sample size because 33 patients were excluded. There is evidence that sarcopaenia of appendicular skeletal muscle is associated with dysphagia in hospitalized older people (5). In addition, malnutrition is associated with lower ADLs and dysphagia in older people (3, 15). Therefore, organic dysphagia due to pharyngeal and oesophageal cancers and sarcopaenia might both cause dysphagia in cancer patients who require rehabilitation.
This study has several limitations. First, it was underpowered to detect a statistically significant association between sarcopaenia and dysphagia. Secondly, cancer types were divided into pharyngeal and oesophageal cancer or other cancers due to the small numbers of patients. In addition, we could not include the cancer site in the logistic regression analysis. Finally, cancer cachexia was not assessed. Further studies investigating associations between sarcopaenia, ADLs, and dysphagia should also assess cancer cachexia in a larger number of patients with specific types of cancer.
In conclusion, the prevalence of sarcopaenia in cancer patients who require rehabilitation is very high. No significant association was observed between sarcopaenia and dysphagia. Further studies with larger sample sizes are needed to assess any potential associations between sarcopaenia and dysphagia in cancer patients.
Hidetaka Wakabayashi, Rimiko Takahashi, Naoko Watanabe, Hideyuki Oritsu, Yoshitaka Shimizu declare no conflicts of interest. This work was supported by a research Grant-in-Aid for Scientific Research C (no. 16K01460) from the Ministry of Education, Science, Culture, Sports, Science, and Technology of Japan.


 Click to show fullsize
Click to show fullsize