
From the 1Musculoskeletal & Sports Injury Epidemiology Center, Institute of Environmental Medicine, Karolinska Institutet, Stockholm, 2Department of Neurobiology, Care Sciences, and Society, Division of Physiotherapy, Karolinska Institutet, Huddinge, 3Department of Public Health Sciences, Karolinska Universitetssjukhuset, Stockholm, 4Department of Public Health and Caring Sciences, Uppsala University, Uppsala, 5Naprapathögskolan – Scandinavian College of Naprapathic Manual Medicine, Stockholm, Sweden and 6Institute of Health Policy, Management and Evaluation, University of Toronto, Toronto, Canada
Objective: The aim of this study was to determine whether job strain, i.e. a combination of job demands and decision latitude (job control), and sleep disturbances among persons with occasional low-back pain are prognostic factors for developing troublesome low-back pain; and to determine whether sleep disturbances modify the potential association between job strain and troublesome low-back pain.
Methods: A population-based cohort from the Stockholm Public Health Cohort surveys in 2006 and 2010 (n = 25,167) included individuals with occasional low-back pain at baseline 2006 (n = 6,413). Through logistic regression analyses, potential prognostic effects of job strain and sleep disturbances were studied. Stratified analyses were performed to assess modification of sleep disturbances on the potential association between job strain and troublesome low-back pain.
Results: Those exposed to job strain; active job (odds ratio (OR) 1.3, 95% confidence interval (95% CI) 1.1–1.6), or high strain (OR 1.5, 95% CI 0.9–2.4) and those exposed to severe sleep disturbances (OR 3.0, 95% CI 2.3–4.0), but not those exposed to passive jobs (OR 1.1, 95% CI 0.9–1.4) had higher odds of developing troublesome low-back pain. Sleep disturbances did not modify the association between job strain and troublesome low-back pain.
Conclusion: These findings indicate that active job, high job strain and sleep disturbances are prognostic factors for troublesome low-back pain. The odds of developing troublesome low-back pain due to job strain were not modified by sleep disturbance.
Key words: musculoskeletal disorder; prevention, stress; job stain; sleep disturbance; low back pain.
Accepted May 11, 2017; Epub ahead of print Jun 28, 2017
J Rehabil Med 2017; 49: 591–597
Correspondence address: Eva Rasmussen Barr, Musculoskeletal & Sports Injury Epidemiology Center, Institute of Environmental Medicine, Karolinska Institutet, Box 210, SE-17177, Stockholm, Sweden. E-mail: eva.rasmussen.barr@ki.se
Low-back pain (LPB) remains an alarming health problem worldwide and is a leading cause of disability (1–2). The lifetime prevalence of LBP is high. Up to 85% of people experience LBP at some point and a high percentage experiences subsequent periods of pain (3). The indirect cost of LBP in Sweden in 2010 was reported to be SEK 90 billion (~ EUR 10 billion) (4).
The prognosis of LBP is affected by biomechanical, psychological, social and work-related factors (2, 5). Biomechanical factors are suggested to affect the occurrence of a new episode of LBP, whereas psychosocial factors are suggested to influence the persistence of LBP (2, 6). There has been an increased focus on work-related psychosocial factors in epidemiological studies of LBP (7, 8). One widely-used measure of work-related psychosocial strain in studies on various disorders is the job strain model, also known as the “demand-control model” (9, 10). Here, high strain is described as a combination of high psychological job demands with low job decision latitude (job control). If job strain (high demands/low control) is present, physiological reactions, such as muscle tension, are proposed to increase the risk of subsequent periods of LBP (11, 12). However, findings on the association between job strain and LBP vary (7, 13). Hartvigsen et al. (7) concluded in a review from 2004 that there is insufficient evidence for the association between low job control and LBP, whereas, to date, evidence is emerging that work-related stress, defined in the “demand-control-model,” is associated with LBP (8, 14, 15).
Furthermore, individual factors, including lifestyle-related factors, are associated with LBP (16). A factor closely associated with work-related stress and musculoskeletal pain is sleep disturbance. Here, diverse associations are reported between work-related psycho-logical and psychosocial factors and the association with sleep disturbances (12, 17–20). In the association between sleep quality and pain, a bidirectional causal relationship is also indicated (21, 22). De Lange et al. (23) found significant associations between job demands and job control on sleep quality and fatigue. The role of sleep disturbances in relation to work-related stress and the development of troublesome musculoskeletal pain episodes have hitherto been investigated in few studies (24–26). To our knowledge, no longitudinal study has investigated the effects of exposure to job strain and sleep disturbances in a general population of working age reporting occasional LBP at baseline. We therefore aimed to study whether job strain, i.e. the combination of psychological job demands and job control, and sleep disturbances among persons reporting occasional LBP are prognostic factors for developing troublesome LBP; and to determine whether sleep disturbances modify the potential association between job strain and such a condition.
This prospective cohort study is based on the Stockholm Public Health Cohort (n = 25,167), a population-based cohort set up by Stockholm County Council to collect information about the factors and consequences of significant contributors to the burden of disease (27). The study was approved by the Regional Ethical Review Board in Stockholm, Sweden (registration no. 2013/497-32).
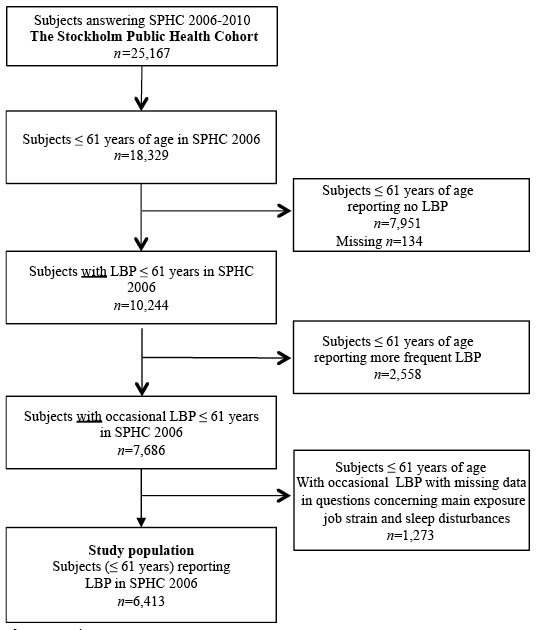
Participants aged 18–84 years were selected using area-stratified random samples of the Stockholm population, an urban region including 24 municipalities with approximately 1.4 million inhabitants (2002). Details of the data collection have been reported elsewhere (27). Randomly selected individuals (n = 56,634) after stratification for sex and residential area received a baseline postal or web-based questionnaire in 2006. Sixty-one percent of these (n = 34,707) answered. Of those who answered at baseline, 25,167 also answered the follow-up in 2010, and members of this group constitute the Stockholm Public Health Cohort 06/10 (SPHC 06/10). The present study included people aged 18–61 years at baseline in SPHC 06/10. This age cut-off was proposed in order to limit inclusion to people of working age, since the follow-up time was 4 years and the official retirement age in Sweden is 65 years. People who reported no or more frequent LBP than occasional at baseline were excluded (n = 2,558) (Fig. 1). Furthermore, those with missing data regarding job demands, job control and sleep were also excluded from the cohort (n = 1,273). The present study population thus comprised those who reported occasional LBP at baseline (n = 6,413). These were people who responded to the question “During the previous 6 months, have you experienced low back pain?”(“No”, “Yes, a couple of days in the last 6 months”, “Yes, a couple of days each month, “Yes, a couple of days each week” and “Yes, everyday”) with either “Yes, a couple of days in the last 6 months” or “Yes, a couple of days each month”.
Fig. 1. Inclusion process.
Baseline data were elicited with questions regarding demographic characteristics, physical health, psychological health, psychosocial work environment, lifestyle factors, socioeconomics, social relations, and sick leave. These questions were those included in the 2006 survey, as reported elsewhere (27).
Potential prognostic factors studied were: self-reported job strain; combination of job demands and job control (high job strain, active and passive jobs); and sleep disturbances reported at baseline.
Job demands and job control were categorized according to the job strain model and analysed as follows: (i) low strain (low job demands and high job control), (ii) active job (high job demands and high job control), (iii) passive job (low job demands and low job control) and (iv) high job strain (high job demands and low job control) (Fig. 2).The original Job Content Questionnaire (JQC) has 5 items on job demand and 9 on job control (28, 29). To investigate job strain, 4 questions from the baseline questionnaire were used; 2 regarding job demands and 2 regarding job control. To test the internal consistency of the 4 questions, Cronbach’s alpha was calculated for job demands (α = 0.53) and job control (α = 0.77). The use of a partial scale compared with a complete, multi-item job-demands-and-control instrument is reportedly feasible, exhibiting high correlations to a complete instrument (Pearson’s correlation coefficient, r = 0.76–0.88); in addition, the present partial instrument assesses the same underlying concepts as the complete instrument (30).
(a) “Do you have enough time to complete your assignments at work?” The answers were dichotomized into yes (yes, usually/always; yes, sometimes) and no (no, rarely; no, never).
(b) “Are there contradictory demands involved in your job?” The answers were dichotomized into yes (yes, usually/always; yes, sometimes) and no (no, rarely; no, never).
(c) “Are you free to decide what needs to be done at work?” The answers were dichotomized into yes (yes, usually/always; yes, sometimes) and no (no, rarely; no, never).
(d) “Are you free to decide how your work is to be carried out?” The answers were dichotomized into yes (yes, usually/always; yes, sometimes) and no (no, rarely; no, never).
People defined as having an active job situation had a combination of high job demands (question a = no, b = yes) and high job control (question c = yes, d = yes). Those with a passive job situation had a combination of low job demands (question a = yes, b = no) and low job control (question c = no, d = no). Those with high job strain had a combination of high job demands (question a = no, b = yes) and low job control (question c = no, d = no), and those with low job strain a combination of low job demands (question a = yes, b = no) and high job control (question c = yes, d = yes) (Fig. 2).
Fig. 2. The job strain model (10).
We assessed sleep disturbances with one question “Do you have difficulty sleeping?” The response options were: no; yes, somewhat (classified as mild sleep disturbances); and yes, severe (classified as severe sleep disturbances). Mild and severe sleep disturbances were categorized as sleep disturbances in the stratified analysis. The sleep question has been included in the Stockholm Public Health surveys since 2002, to determine the prevalence of such disturbances in the population (31).
The outcome in this study was experience of troublesome LBP during the previous 6 months, elicited with questions from the 2010 follow-up survey. Participants who answered “yes” to both of the following questions were defined as having had troublesome LBP: “During the past 6 months, have you felt pain, (at least a couple of days per week) in your lower back? (yes/no). If so, has this restricted your work capacity or hindered you in daily activities to some degree or to a high degree? (yes/not at all)”.
Potential confounders were chosen from the baseline questionnaire guided by knowledge from prior research, and by clinical considerations (2, 32). The potential confounders were age (continuous and dichotomized into 18–41/42–61 years), sex (men/women) smoking habits (yes, daily), alcohol consumption (some time during a period of 12 months), neck/shoulder/arm pain the previous 6 months (yes; more than 2 days), socioeconomic class (unskilled and semi-skilled workers, skilled workers, assistant non-manual employee, intermediate non-manual employees, employed/ self-employed/professional), low support at work from superior (yes/no), low support at work from colleagues (yes/no), main physical workload in the past 12 months (sedentary, light, moderately heavy, heavy), time spent on household work per day (yes > 10 h), economic stress based on the question “Did it happen that during the past 12 months you ran out of salary/money and had to borrow from relatives or friends in order to pay for food or rent?” (yes), country of birth (Sweden/elsewhere), and leisure physical activity level (sedentary < 2 h per week/active ≥ 2 h per week). We also tested job strain (low strain, active and passive jobs and high strain) as a potential confounder in the sleep-disturbances model.
For the analyses of associations between the prognostic factors and the outcome, logistic regression models were used. Results are presented as odds ratios (OR), along with 95% confidence intervals (95% CI). The significance threshold was set at p < 0.05.
Two separate regression models were built for the analyses: 1 with the 4 levels of job strain: (low job strain (reference category), active jobs, passive jobs, and high job strain), and 1 with the 3 levels of sleep disturbances (none (reference category), mild, severe). For each of the 2 regression models, potential confounding factors were added 1 at a time to the crude regression model. As described by Rothman & Greenland (33), a factor that changed the crude OR by 10% or more was considered a confounder and was entered into the final model. Finally, we stratified the analyses of the association between job strain and troublesome LBP by sleep disturbances/no sleep disturbances in order to study whether the effect of job strain was modified by sleep disturbances.
The final adjusted model for the exposures active job, passive job and job high strain included the confounders as socioeconomic class, workload and support at work from one’s superior. In the final adjusted model for sleep disturbances no confounding factors were included.
To test the goodness-of-fit of the statistical models Hosmer-Lemeshow χ2 test was performed.
Statistical analyses used the STATA® statistical software system version 11.
The characteristics of those who experience occasional LBP at baseline (n = 6,413) stratified by the job-strain-model categories are presented in Table I. Fifty-eight percent (n = 3,713) of the cohort were women, and 73% (n = 4,719) were aged 18–41 years. Mean age for the cohort was 42 years (SD 11) and did not differ among job strain categories. Of the cohort, 929 persons (14%) reported active job at baseline, 470 (7%) reported passive job and 103 (2%) reported high job strain. In total, 2,062 (32%) reported sleep disturbances at baseline. Twenty-four percent (n = 1,541) of the cohort reported troublesome LBP at follow-up (2010).
Table I. Baseline measurements of study population with occasional low back pain (n = 6,413) stratified for job strain types
After adjustment for confounding factors the analysis yielded an OR of 1.3 (95% CI 1.1–1.6) for active job and an OR of 1.5 (95% CI 0.9–2.4) for high strain for the associations with troublesome LBP at follow-up in 2010 (Table II). Individuals exposed to passive job OR 1.1 (95% CI 0.9–1.4) showed no association with troublesome LBP during the previous 6 months, at follow-up. There was a significant overall association between the categories of job strain and the outcome (p = 0.005).
Table II. Associations of job strain and sleep disturbances with troublesome low back pain. The associations are presented as crude and adjusted odds ratios (OR) with 95% confidence intervals (95% CI)
Sleep disturbances at baseline were associated with troublesome LBP during the previous 6 months reported at follow-up (Table II). The analysis yielded an OR of 1.5 (95% CI 1.3–1.7) for mild sleep disturbances and 3.0 (95% CI 2.3–4.0) for severe sleep disturbances, compared with the reference category no sleep disturbances. There was a significant overall association between the categories of sleep disturbances and the outcome (p = 0.000).
The goodness-of-fit measure (Hosmer-Lemeshow) showed that the models fit the data (job strain model: p = 0.89; sleep disturbance model: p = 1.00).
Table III shows the results of the analysis stratified for sleep disturbances. In the stratum no sleep disturbances, the adjusted ORs for the association of active and passive job at baseline with troublesome LBP at follow-up were 1.3 (95% CI 1.0–1.6) and 1.2 (95% CI 0.9 –1.7), respectively, and for high job strain OR 1.4 (95% CI 0.7–2.7). For the stratum sleep disturbances, the adjusted ORs for active and passive job at baseline and troublesome LBP at follow-up were 1.3 (95% CI 1.0–1.7) and 0.8 (95% CI 0.6–1.2), respectively. The OR for high strain was 1.4 (95% CI 0.7–2.6).
Table III. Associations of job strain with troublesome low-back pain, stratified into no sleep disturbances/sleep disturbances (mild/severe), presented as crude and adjusted odds ratios (OR) with 95% confidence intervals (95% CI)
This study aimed to determine whether work-related stress in terms of job strain, and in addition sleep disturbances, were prognostic factors for developing troublesome LBP in a population of working age reporting occasional LBP at baseline. In addition, we studied whether the association between job strain and troublesome LBP was modified by sleep disturbances. Our findings indicate that the “quadrants” in the “demand-control model” (9, 34); active job (high job demands and high job control) and high job strain (high job demands and low job control) were associated with at least one episode of troublesome LBP during follow-up. This association was not modified by sleep disturbances. Our findings align with those from a recent study from our group in which high strain and active job emerged as prognostic factors for troublesome neck/shoulder/arm pain in a population with occasional such pain (26). Whereas active jobs and job strain are reported as important factors for the development of several disorders, passive jobs seemingly are not. Passive jobs are proposed to be related to an overall low activity resulting in more passive lifestyles (34). Karasek proposed that the exposure to passive jobs may “damage health by inhibiting learning ability and contributing to learned helplessness”(34). On the contrary, having an active job situation might give physiological reactions, such as muscular strain, important for the development of neck/shoulder/arm and seemingly also occurring in LBP (11, 12).
Hitherto, studies on job strain in relation to LBP show diverse findings. A meta-analysis concluded that this kind of relationship does not exist in LBP (7). This is in contrast to a more recent meta-analysis (8) reporting on associations between work-related high demands and low control and the onset of LBP. In addition, a report from the the Swedish Council on Health Technology Assessment (SBU) concluded that there is insufficient evidence that work “demands” (high or low) are associated with LBP, whereas there is moderate evidence that low control has such an association, partly aligning with our findings (35).
Sleep disturbances emerged as a prognostic factor for developing troublesome LBP. Sleep quality is important for recovery (36, 37), and the role of poor sleep quality appears important for a negative prognosis of pain (19–20, 23). The relationship between sleep disturbance and pain is, in several studies, suggested to be reciprocal: pain disturbs sleep quality and poor sleep quality further exacerbates pain (21, 38, 39). It might be that sleep disturbance is a mediator in the causal pathway between job strain and troublesome LBP, but since sleep disturbance and job strain were measured at the same time point, this was not investigated in this study. For this reason also, sleep disturbance was not tested as a potential confounder in the association between job strain and troublesome LBP, but as an effect modifier. The results did not support that sleep disturbances are effect modifiers for this association.
Sleep disturbances are common and proposed as a modifiable factor important to consider from a public health perspective. In addition, management of sleep disturbances might have possible benefits beyond the improvement in sleep, for example in pain processes (21). In our cohort, 32% reported mild or severe sleep disturbances consistent with our earlier findings in a population with occasional neck/shoulder/arm pain (26). In the present study however, sleep disturbances did not modify the association between job strain and troublesome LBP.
A strength of the present study is its prospective design, which was based on a general population of working age and included several important work-related factors: the job strain model and sleep disturbances prior to outcome. Moreover, several potential confounders were taken into account: among others, support from superior and colleagues, socio-economic class and working situation. Even so, we cannot rule out the risk of unmeasured or residual confounding, for instance from other psychosocial factors, such as catastrophizing and somatization.
The well-recognized job strain model was used to assess work-related stress (9, 34). A frequently used questionnaire is the Job Content Questionnaire (JCQ), developed to measure the construct job strain (28). The JCQ comprises 5 items addressing job demands and 9 addressing control. We used 4 items from the JCQ to measure the constructs of job strain; these were included in the Stockholm Public Health Cohort 06/10. This was judged feasible based on findings of consistently high agreement between partial scales measuring job strain and a complete survey. A potential limitation is that the lower sensitivity of a shorter scale may increase the risk of non-differential misclassification of exposure (i.e. in this case, the prognostic factors, possible resulting in a dilution of the true effect). However, the sensitivity of the shorter scales was reported to be high (r > 0.94) (30). In addition, low sensitivity of the exposure measure is mainly a problem when the exposure is common; this is not the case with job strain, but with sleep disturbances.
Despite that this study is based on a cohort of > 25,000 persons, there were only 37 exposed cases in the analysis of the association between high job strain and the outcome. This relatively low statistical power could explain why the association was not statistically significant, and larger studies are needed to confirm the results. Another limitation of the present study is that sleep disturbances were investigated at baseline based on a single question, as was also the outcome troublesome LBP. This may lead to a misclassification of this exposure and/or the outcome. Since we have no reason to believe that a potential misclassification of the exposure is related to the outcome in a prospective cohort study, or that the potential misclassification of the outcome is related to the exposure, the most probable effect would be dilution of the true association between the exposures and the outcome. In view of this, since we found associations between mild and severe sleep disturbances and troublesome LBP, the true association is likely to be stronger in such a case.
We lack information about the duration of the exposures prior to baseline or about the presence of the exposures during the 4-year follow-up period. This may introduce a misclassification of exposure that, again, most probably is non-differential. Some study participants classified as exposed at baseline, might, after a while, be unexposed, and some participants classified as unexposed at baseline may, after a while, be exposed, which might result in a dilution of a true association.
In addition, selection bias is a potential threat to validity and may be present if the loss to follow-up differs among participants who are exposed and unexposed, and if the loss is also related to the outcome (33). Additional analyses showed that the proportion of those exposed to job strain and sleeping disturbances differed only marginally between those who completed the follow-up and those who did not. Accordingly, selection bias is not likely to affect our findings.
Logistic regression was used for the analyses of the associations in the study. Since the outcome (that is, troublesome LBP) is relatively common, the calculated OR might be higher than a corresponding relative risk (RR), and the results should not be interpreted as such.
Job strain is extensively studied and reported to be harmful in various lifestyle-affected disorders, among others such as type II diabetes and heart disorders (40–42). It is also one of several important work stress-related factors that seem to influence musculoskeletal pain, such as troublesome LBP. We propose that active job, high job strain and sleep disturbances are modifiable prognostic factors. It is important for employers and caregivers to consider psychosocial factors when implementing measures to minimize the risk of troublesome LBP at workplaces. People with occasional LBP reporting high job stain and active job need to be recognized in their working situation and be given opportunities to lower the job stress.
Our findings indicate that active job, high job strain and sleep disturbances are prognostic factors for troublesome LBP. The increased odds of developing troublesome LBP due to job strain were not modified by sleep disturbance. Additional large prospective studies are needed to confirm our results.
The Stockholm Public Health Cohort was financed by the Stockholm County Council. Financial support for the study was obtained from the AFA Insurance postdoctoral scholarship.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize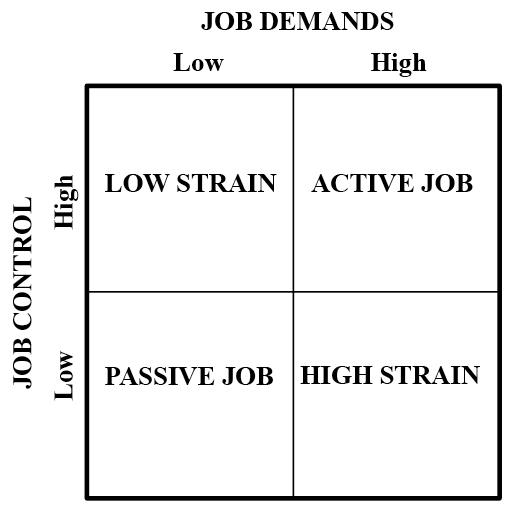 Click to show fullsize
Click to show fullsize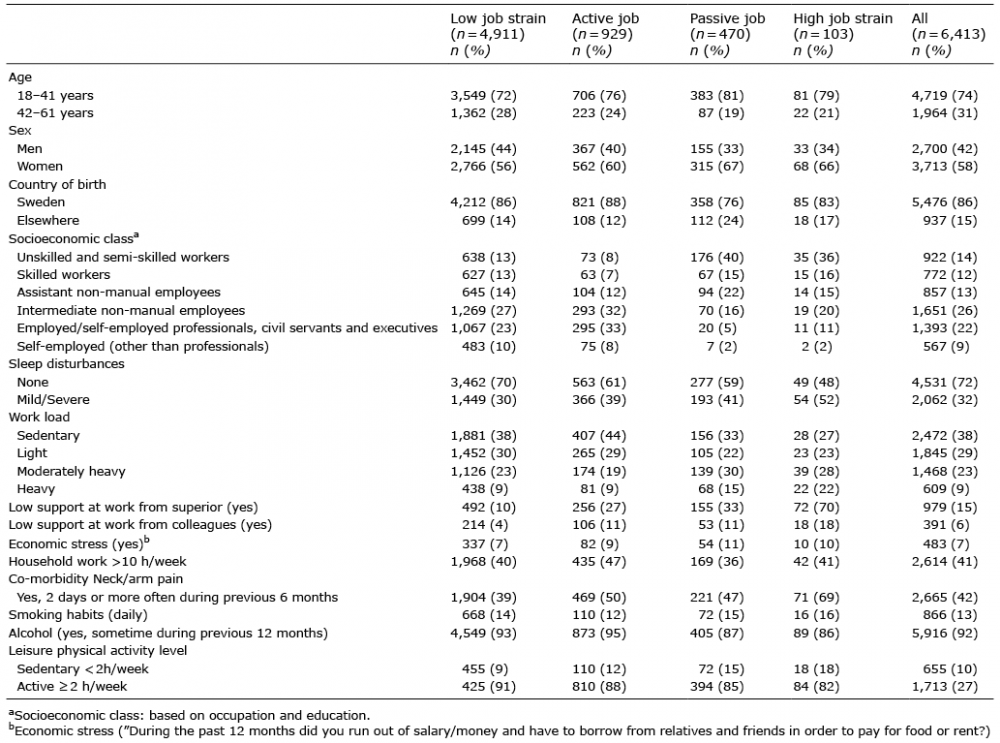 Click to show fullsize
Click to show fullsize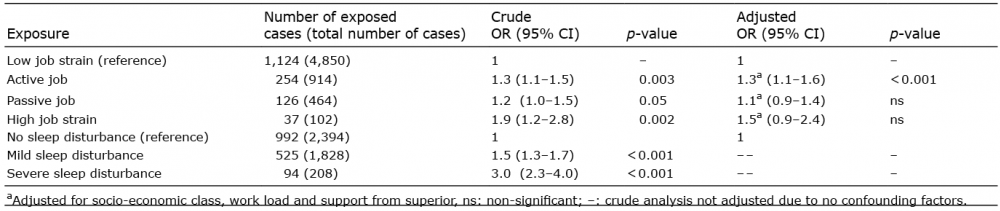 Click to show fullsize
Click to show fullsize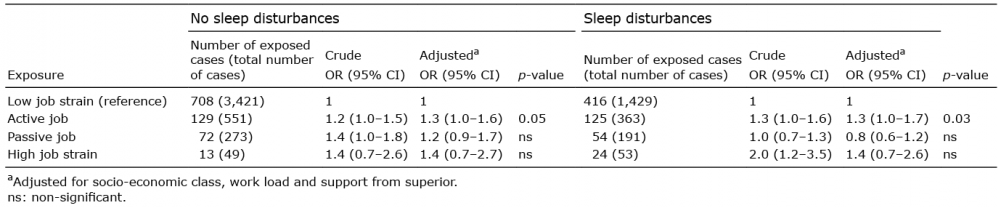 Click to show fullsize
Click to show fullsize