
From the 1University of Texas Health Science Center McGovern Medical School and TIRR Memorial Hermann, Houston, TX, USA, 2Multiple Sclerosis Center of California & Research Group, Newport Beach, CA, USA, 3The Walton Centre, Liverpool, UK, 4University of Freiburg, Department of Neurology, Freiburg im Breisgau, Germany, 5Allergan plc, Irvine, CA, USA, 6QuintilesIMS Real-World Evidence, Cambridge, MA, USA, and 7MossRehab Gait and Motion Analysis Laboratory, Elkins Park, PA, USA
Objective: The main aim of this study was to determine the utilization patterns and effectiveness of onabotulinumtoxinA (Botox®) for treatment of spasticity in clinical practice.
Design: An international, multicentre, prospective, observational study at selected sites in North America, Europe, and Asia.
Patients: Adult patients with newly diagnosed or established focal spasticity, including those who had previously received treatment with onabotulinum-toxin A.
Methods: Patients were treated with onabotulinumtoxinA, approximately every 12 weeks, according to their physician’s usual clinical practice over a period of up to 96 weeks, with a final follow-up interview at 108 weeks. Patient, physician and caregiver data were collected.
Results: Baseline characteristics are reported. Of the 745 patients enrolled by 75 healthcare providers from 54 sites, 474 patients had previously received onabotulinumtoxinA treatment for spasticity. Lower limb spasticity was more common than upper limb spasticity, with stroke the most common underlying aetiology. The Short-Form 12 (SF-12) health survey scores showed that patients’ spasticity had a greater perceived impact on physical rather than mental aspects.
Conclusion: The data collected in this study will guide the development of administration strategies to optimize the effectiveness of onabotulinumtoxinA in the management of spasticity of various underlying aetiologies.
Key word: onabotulinumtoxinA; muscle spasticity; research methodology; botulinum toxin; Type A; ASPIRE; baseline characteristics.
Accepted May 8, 2017; Epub ahead of print Aug 14, 2017
J Rehabil Med 2017; 49: 00–00
Guarantor’s address: Aubrey Manack Adams, Allergan plc, Global Medical Affairs, 2525 DuPont Dr, Irvine, CA, USA. E-mail: Adams_Aubrey@allergan.com
Spasticity is a chronic condition defined as “disordered sensory-motor control, resulting from an upper motor neuron lesion, presenting as intermittent or sustained involuntary activation of muscles” with postural limb changes (1). Spasticity is characterized by muscle stiffness, paresis, muscle spasms, muscle fatigue, and rheological change with abnormal upper and/or lower limb postures potentially accompanied by pain and contractures (2–5). Beyond the underlying primary disorder and disease, spasticity negatively influences patient quality of life and increases caregiver burden (6, 7).
Spasticity is commonly associated with central nervous system disorders, including stroke, multiple sclerosis, cerebral palsy, traumatic brain injury, and spinal cord injury, as well as neurodegenerative diseases (3, 6, 8, 9). Post-stroke, ~40% of patients develop spasticity, with severe or disabling spasticity in up to 15% of patients (10, 11). Approximately one-third of patients with multiple sclerosis present with minimal spasticity, while 30% have moderate or severe spasticity, and 4% have generalized spasticity, which impede activities of daily living (12–15). Of those who have sustained a traumatic brain injury, approximately 75% develop spasticity, with half warranting anti-spasticity treatment (16–18).
Treatments for spasticity decrease muscle overactivity, improve abnormal limb posture, and aim to reduce the effect of spasticity on activities of daily living and improve quality of life. Management options include physical therapy, oral medication, chemical neurolysis, intrathecal baclofen, intramuscular botulinum toxin injections, and surgery, with a combination of treatments often recommended (4, 15, 19, 20).
Botulinum toxin treatment is a beneficial option in the management of focal spasticity (15, 19–23). OnabotulinumtoxinA (Botox®, Allergan plc, Dublin, Ireland) acts via blocking neuromuscular transmission by binding to acceptor sites on motor or sympathetic nerve terminals, entering nerve terminals, and inhibiting acetylcholine release (24, 25). Intramuscular injections at therapeutic doses produce muscle chemodenervation, resulting in localized overactivity and hyperactivity reductions in selected muscles with minimal systemic effects. The efficacy and safety of onabotulinumtoxinA has been demonstrated (22), and it is now approved for use in upper and lower limb spasticity in the US and worldwide (25).
A prospective multicentre, observational, real-world study in US patients with stroke or traumatic brain injury with spasticity indicated that 6 months of physical therapy plus onabotulinumtoxinA facilitated functional-based goals (26). However, more research on onabotulinumtoxinA use is needed to determine the most appropriate muscle selection for each presentation, individualized administration strategies for maximizing effectiveness, and outcomes after long durations of treatment. Furthermore, epidemiological data are needed to help optimize understanding of the clinical course of spasticity. Given this information gap, a large observational database, the Adult SPasticity International REgistry (ASPIRE) Study, was developed to describe the clinical characteristics of spasticity and its burden across multiple aetiologies and geographical regions. The dataset will serve to educate clinicians in the diagnosis and treatment of spasticity in clinical practice. The main objective of the ASPIRE Study is to determine utilization patterns and effectiveness of onabotulinumtoxinA for the treatment of spasticity in clinical practice. We present here the methodology, study design, and baseline patient, healthcare provider (HCP) and caregiver demographics and patient disease characteristics for the ASPIRE Study and begin to examine patient, HCP, and caregiver perspectives.
The ASPIRE Study is an international, multicentre, prospective, observational study conducted at selected sites in North America, Europe, and Asia. Treatments were administered at the discretion of the treating physician or HCP in accordance with usual clinical practices and country-specific regulations. Re-treatment with onabotulinumtoxinA took place approximately every 12 weeks; however, time between re-treatments varied in clinical practice, based in part on the perceived duration of intervention effect. Each patient was followed for up to 108 weeks after the baseline treatment, with a follow-up interview conducted approximately 12 weeks after completion of the final treatment in the study period (0–96 weeks).
Patients were required to provide written informed consent, including for the review of medical records and for the enrolling HCP to contact any treating HCP administering onabotulinumtoxinA outside of the study, if applicable. Institutional Review Board approval was granted at each participating site.
Sites were selected to reflect geographical distribution within each country. The number of patients enrolled at a single site was limited in order to collect information on diverse treatment practices across a number of physicians and sites. In addition, target quotas for patient enrolment were recommended in order to facilitate enrolment of patients treated for spasticity with a range of underlying aetiologies, and to enrol patients newly treated with onabotulinumtoxinA (treatment-naïve patients) as well as those who had previously received this treatment (non-naïve patients). Physicians were instructed to identify patients who were eligible for participation during the enrolment period and to consecutively enrol patients who met the inclusion criteria and none of the exclusion criteria for the study.
Male or female patients at least 18 years old at participating sites treated with onabotulinumtoxinA in the course of routine clinical practice for newly diagnosed or established focal spasticity were eligible for inclusion in the study, regardless of whether they had previously received treatment with onabotulinumtoxinA. To be eligible, patients also needed to have the cognitive and linguistic ability to complete study questionnaires, as determined via a subjective assessment by the enrolling HCP, be willing and able to answer questions by telephone or internet on a scheduled basis with or without the assistance of a caregiver, and be willing and able to provide informed consent. Patients actively participating in a clinical trial for the treatment of spasticity or with a condition or situation that would interfere significantly with the conduct of the study, as determined by the enrolling HCP, were excluded from the study.
Data were collected throughout the 108-week follow-up period (Fig. 1). Patient demographics and clinical characteristics, HCP characteristics, and caregiver demographics were collected at baseline. Patient-, HCP-, and caregiver-reported outcomes were collected at selected time-points throughout the study (Fig. 1, Table I).
Fig. 1. Adult SPasticity International REgistry (ASPIRE) study design and assessments. AE: adverse event; BCOS: Bakas Caregiving Outcome Scale; DAS: Disability Assessment Scale ; HCP: Health care provider ; LL: lower limb; MS: multiple sclerosis ; NPRS: Numeric Pain Rating Scale ; SF-12: Short Form 12 Health Survey; SIA: Spasticity Impact Assessment; UL: upper limb.
Table I. Patient-, healthcare provider- (HCP), and caregiver-reported outcomes assessments
Patterns of onabotulinumtoxinA use, including dosages and the effectiveness of those doses, as measured by patient-reported and HCP-reported treatment satisfaction outcomes, were evaluated. Patient-reported outcome data were recorded to evaluate the impact of various levels of spasticity on therapeutic outcomes, and caregiver-reported outcome data were recorded to evaluate the impact of spasticity (and its treatment) on caregiver burden and the quality of life of caregivers in treatment-naïve patients. Estimates of how often botulinum toxins were being used for other indications among patients currently treated with onabotulinumtoxinA for spasticity were also recorded. The incidence of adverse events associated with onabotulinumtoxinA was recorded.
This study aimed to enrol up to 1,000 eligible patients from sites in the US and internationally, with the aim of one-third of the study participants being onabotulinumtoxinA-treatment naïve for spasticity.
The analysis population included all enrolled patients who received at least one dose of onabotulinumtoxinA. All analyses addressing the primary study objective were stratified by treatment site (i.e. upper and lower limb), treatment history (i.e. naïve and non-naïve), and by patients treated with onabotulinumtoxinA for other indications. Secondary analyses may be conducted for additional subgroups of patients depending on available sample size.
All analyses in this study were descriptive in nature and were not testing any specific hypotheses. No formal sample size or statistical power calculations were performed. All analyses were performed using SAS version 9.2 or higher (SAS Institute, Cary, NC, USA).
As of 19 February 2016, 745 patients have been enrolled by a total of 75 HCPs across 54 sites in the US (n = 444, 36 HCPs in 26 sites), UK (n = 88, 5 HCPs in 5 sites), Italy (n = 66, 5 HCPs in 4 sites), Germany (n = 43, 6 HCPs in 6 sites), France (n = 40, 4 HCPs in 4 sites), Spain (n = 23, 7 HCPs in 7 sites), and Taiwan (n = 41, 8 HCPs in 2 sites). This population represents the final enrolled population in this study; no additional patients will be enrolled. Data from 71 HCPs are included in this analysis. Out of the 745 enrolled patients, 474 had received onabotulinumtoxinA treatment for spasticity in the past and 271 had not.
Review of the data revealed that 15 enrolled patients were inadvertently treated with a botulinum toxin other than onabotulinumtoxinA during the study. These patients were classified as having protocol deviations; however, they were included in this analysis as the data presented here reflect baseline demographics. Future analyses will exclude these patients.
Overall, the majority of participating HCPs were identified as physicians (60.6%); however, the majority (74.1%) of HCPs in the European Union (EU) were described as “clinical specialists” (i.e. a medical practitioner with additional specialty training, Table II). Across all countries, the most common primary focus or specialty was physical medicine and rehabilitation (57.7%), while neurology was the primary specialty indicated by physicians in the US (52.8%) and Germany (100%). Approximately one-third of HCPs practiced in a general hospital and one-third practiced in an academic medical centre. In the US, over 40% of HCPs practiced in an office-based setting. Most HCPs had been using onabotulinumtoxinA for the treatment of spasticity for more than 10 years (60.3%). Experience with onabotulinumtoxinA for spasticity was slightly lower in Taiwan, with 62.5% having 6–10 years of experience using onabotulinumtoxinA. In addition, the majority of HCPs (75.4%) indicated that they had previously used botulinum toxin(s) for treatments other than spasticity.
Enrolled patients were, in mean, 53.7 years of age (standard deviation (SD) 15.4), age range 18.5–93.2 years (Table II). The oldest patient population was in Spain (n = 23; mean 62.0 years; SD 15.6 years) and the youngest was in Taiwan (n = 41; mean 49.3 years; SD 14.8 years). The majority of patients (n = 332, 44.7%) were receiving disability benefits. For the remaining patients, 182 (24.5%) were retired, 84 (11.3%) were employed full-time, 80 (10.8%) were unemployed, and 39 (5.2%) were employed part-time at their baseline visit. A total of 430 patients (57.9%) stated that they had a caregiver; 175 (65.1%) were naïve patients and 255 (53.8%) were non-naïve patients (p < 0.05).
Table II. Baseline patient and healthcare provider demographics and characteristics
The majority of enrolled patients (n = 421, 56.7%) had an underlying aetiology of stroke, followed by 120 patients (16.2%) with multiple sclerosis (MS) (Fig. 2). Of these patients, most had either secondary progressive MS (n = 47, 40.9%) or relapsing/remitting MS (n = 40, 34.8%).
Fig. 2. Underlying aetiology of spasticity at baseline. OnabotA: onabotulinumtoxinA. *Data were not available for all patients; some patients had spasticity of more than one aetiology. †Stroke includes ischaemic, haemorrhagic, or embolic stroke. ‡Other includes hereditary spastic paraparesis, stroke during aneurysm clipping, Chiari malformation, and hydrocephalus.
At baseline, approximately half of the enrolled patients (n = 379, 51.1%) were using or had ever used baclofen (Fig. 3), most of whom were using or had used baclofen for spasticity (n = 370). The majority of patients (n = 587, 82.1%) were also receiving physio-therapy or occupational therapy and indicated having assistive devices (n = 505, 70.7%) or orthotics (n = 383, 53.6%). The data were generally comparable between the naïve and non-naïve populations and across aetiologies and clinical presentations (Tables SI–SIII1).
Fig. 3. (a) Oral medications and (b) treatment modalities used at baseline. OnabotA: onabotulinumtoxinA. *Data were not available for all patients for all medications and all treatments, percentages reflect percentage of respondents providing data for each medication or treatment.
The caregivers had a mean age of 58.6 (SD 12.1) years at baseline and the majority (61.9%) were identified as a spouse or live-in partner (Table III). The caregivers were mainly employed full-time (38.1%) or were retired (35.6%) at baseline.
Table III. Baseline caregiver demographics
Overall, more patients (n = 628, 84.5%) presented with lower limb vs upper limb spasticity (n = 535, 72.0%) at baseline. Spasticity presented slightly more commonly on the left side for both upper (55.3%) and lower limb (51.8%) spasticity. The most common upper limb spasticity presentations were flexed elbow (n = 371, 22.6%) and clenched fist (n = 359, 21.9%) (Fig. 4a). For patients with lower limb spasticity, the most common presentation was equinovarus foot (n = 530, 34.7%) (Fig. 4b). The majority of patients had marked or considerable increase in tone, as evaluated by the Ashworth score (Fig. 4c, d).
Fig. 4. Baseline clinical presentation and characteristics of spasticity of the upper and lower limbs. OnabotA: OnabotulinumtoxinA. *Other is other muscles or groups of muscles.
The mean composite physical health score was 33.6 (SD 9.2; range 9.8–58.4). The mean score was slightly higher in the non-naïve vs the naïve population (34.3 vs 32.6, respectively). At baseline, the mean composite mental health score was 47.4 (SD 12.0; range, 11.7–75.1) with a mean score slightly higher in the non-naïve population (non-naïve, 48.3; naïve, 46.0). With regards to the SF-12 domain scores (27), the lowest scores were observed for role functioning (physical) and physical functioning domains, while the highest scores were seen in mental health and role functioning (emotional) (Fig. 5). The mean domain scores were consistently lower in the naïve vs non-naïve population. Overall, the trends in the data were generally comparable across aetiologies and clinical presentations (Tables SIV and SVI1)
To our knowledge, the ASPIRE study represents the largest existing international database prospectively evaluating patients with spasticity of a variety of aetiologies and across multiple geographical regions. This large and diverse sampling of data attempts to provide comprehensive information about the patients receiving and the HCPs administering onabotulinumtoxinA for spasticity. In turn, future data from this study will provide a basis for evaluating a variety of factors that may contribute to and aid in the design of the best treatment strategies for spasticity, by describing patterns such as clinical characteristics and treatment utilization and the associated outcomes. In addition, information from caregivers will help to provide insights into the burden of caring for patients with spasticity, and the impact that patients’ disease and its symptoms and management may have on their own quality of life.
Overall, baseline patient demographics and clinical characteristics were generally consistent between countries and between the naïve and non-naïve populations, providing a good source of data for comparison. The data also show that most patients are being treated with a combination of oral medications and other treatment modalities, as has been advocated (4). Data from this study will help to further clarify the impact of combination treatments on both patient and caregiver outcomes.
The presentation and characteristics of spasticity were also consistent between populations. The most common presentations of spasticity in this study appear to be representative of the underlying population with spasticity (3, 28, 29). The burden of spasticity on the patient also continues to be evident from the baseline quality-of-life data. The SF-12 scores indicate that patients perceive that their spasticity has a greater impact on physical rather than mental aspects, as observed in both composite and domain scores at baseline. Furthermore, at baseline, spasticity appeared to have a consistently greater impact on quality of life in naïve vs non-naïve patients. Further analysis is required to understand whether this is as a result of previous botulinum toxin therapy, other concomitant therapy, or is a factor of the time since the underlying neurological event. It will also be interesting to understand the extent to which onabotulinumtoxinA therapy is used for the treatment of other conditions in patients with spasticity, and the impact such treatment has on the symptoms of spasticity.
In addition to the data from the patient population, the data from the caregiver population are representative of the diverse pool of caregivers in the real world. Caregivers vary widely in age and employment status, both of which may be factors in the degree of burden experienced by the caregiver. They may also be important factors in how the caregiver perceives the impact that any improvement in the patient’s spasticity has on their own personal quality of life. The data gathered from caregivers in this study will provide useful information on the extent of burden experienced and the correlation between patient- and caregiver-outcomes. Reports have shown that caregiver burden is related to the degree of patient disability (6, 7, 30), caregivers who experience burden have a greater risk of depression and a lower quality of life (13). Therefore, when adequate treatment reduces the patient’s degree of disability, one would also expect treatment to have a significant impact on caregivers (7, 13).
Lack of reliable, valid and sensitive measures of spasticity and heterogeneity across studies has led to limitations in data on spasticity (10). One of the first large studies of patients in the USA with stroke or traumatic brain injury-related spasticity conducted over a 6-month period reported real-world injection data and concluded that physical therapy, together with onabotulinumtoxinA treatment, facilitated functional-based goals, such as gait, balance, and assisted activities of daily living (26). The collection of data from patients with spasticity due to a range of underlying aetiologies and across a range of geographical regions will help to enable greater standardizing of measures and support a greater understanding of the clinical course of spasticity.
Regarding our baseline data, it is important to recognize that, since the ASPIRE study source population represented those who were seeking treatment with onabotulinumtoxinA, findings regarding the clinical characteristics, demographics and burden may not extrapolate to the untreated spasticity population. The untreated population, for example, may differ in spasticity severity, age, time since diagnosis, adjunctive treatment, and/or caregiver status. In addition, it is important to note that the practice settings included in this study were pre-selected and vary in type within and across countries. These differences in site characteristics may have an influence on treatment practices; therefore, data may not be generalizable. Given the lack of data in this area, these findings help reduce the epidemiological data gap among the onabotulinumtoxinA-treated population, but there is still a need for population-based studies to understand the prevalence and natural course of spasticity.
Regarding the design of the ASPIRE study, while large registry studies can provide a considerable amount of valuable data, they have certain limitations. Due to the observational nature of this study, there is a lack of control over the study elements. In addition, while the long-term nature of this study will provide important information, the length of the study often leads to high levels of patient drop-out causing some challenges in interpreting data at later visits. Furthermore, limited inclusion/exclusion criteria may lead to additional complexity in analysing and interpreting the data due to confounding factors, such as different combinations of treatment and treatment modalities, and the use of botulinum toxin for other indications. The need to limit our study to patients with the cognitive ability to complete study questionnaires may mean that our results are not as applicable to the most complex and severely affected patients presenting with spasticity. However, the study features will allow data from this international study to help inform the management of the large majority of the overall population with spasticity of varying underlying aetiologies, and be representative of their real-world clinical management.
In conclusion, baseline data from the ASPIRE study provide valuable information about the demographics and characteristics of patients being treated for spasticity and the impact of spasticity on their quality of life. It will also provide valuable information about those providing treatment and care.
Overall, this study will provide long-term data from up to 108 weeks of follow-up, examining the use of onabotulinumtoxinA, including patient and provider treatment satisfaction. These data will help to guide the development of appropriate administration strategies to optimize the effectiveness of onabotulinumtoxinA in the management of patients with spasticity of various underlying aetiologies.
This study was sponsored by Allergan plc (Dublin, Ireland). Writing and editorial assistance was provided to the authors by Amy Kuang, PhD, of Allergan plc and funded by Allergan plc (Dublin, Ireland). All authors met the ICMJE authorship criteria. Neither honoraria nor payments were made for authorship.
Dr Francisco received research support or consulting honoraria from Allergan, Ipsen, Mallinckrodt, Medtronic, Merz, Microtransponder, and Nexstim. Dr Bandari has no financial disclosures to report. Dr Bavikatte received research support, honorarium and travel grants from Allergan, Ipsen, Merz, Pfizer, Grunenthal. Dr Jost is a speaker and an Advisory Board Member for Abbvie, Allergan, Bial, Desitin, IPSEN, Merz, UCB and Zambon. Dr Manack Adams is a full-time employee of Allergan and owns stock in the company. Dr Largent is a full-time employee of QuintilesIMS, the contract research organization responsible for the management of this study and was formerly a full-time employee of Allergan. Dr Esquenazi received research support from Allergan and Ipsen.


 Click to show fullsize
Click to show fullsize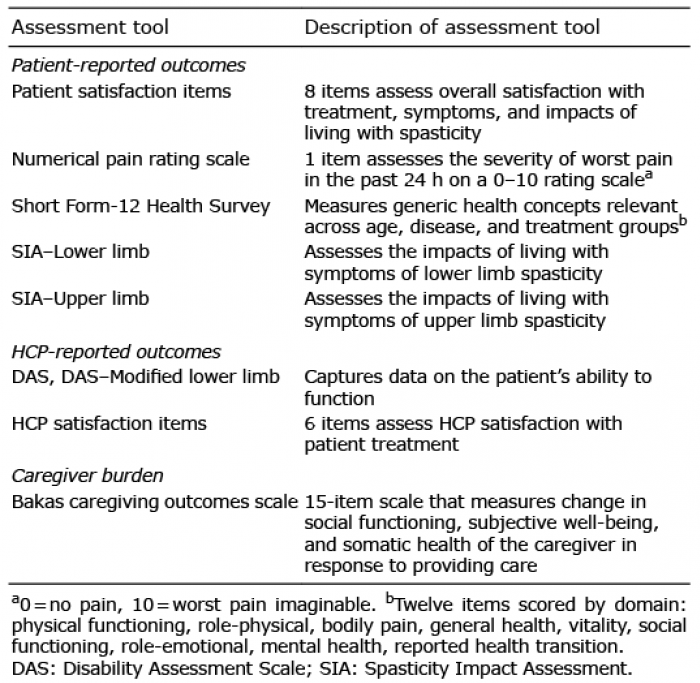 Click to show fullsize
Click to show fullsize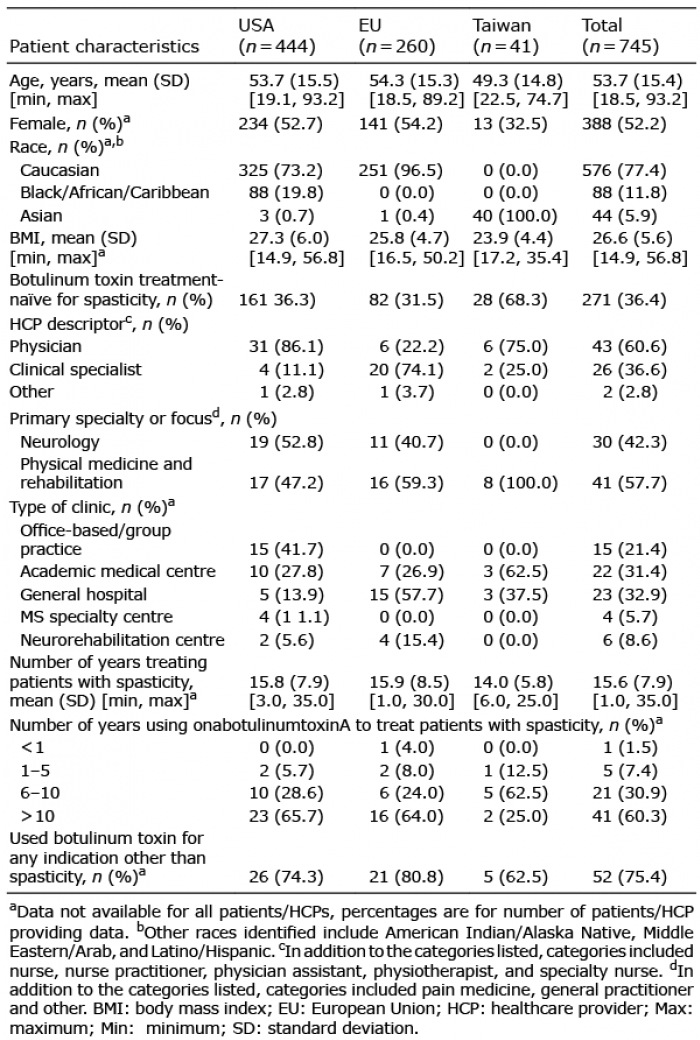 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize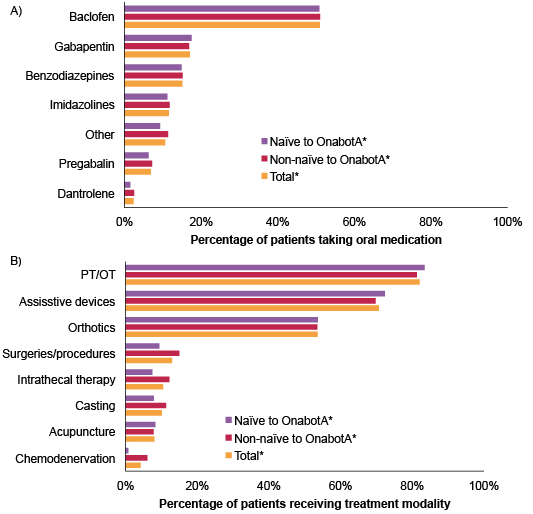 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize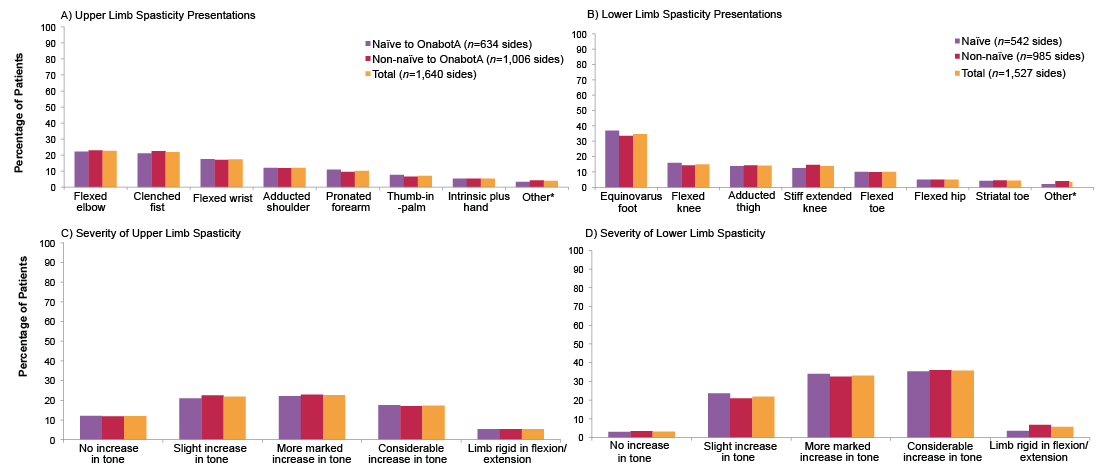 Click to show fullsize
Click to show fullsize