
From the 1Karolinska Institutet, Department of Neurobiology, Care Sciences and Society, Sweden, 2University of the Western Cape, Physiotherapy Department, South Africa, 3Stockholms Sjukhem Foundation, 4Rehab Station Stockholm, Research and Development Unit, 5REMEO Clinic, Stockholm, Sweden, 6Karolinska University Hospital, Solna, 7Spinalis Foundation, Stockholm and 8Academic Primary Healthcare Centre, Stockholm County Council, Stockholm, Sweden
Objectives: To update the incidence rate, aetiology and injury characteristics of acutely-injured adults with traumatic spinal cord injury in Stockholm, Sweden, using international standards of reporting.
Study design: Prospective, (regional) population-based observation.
Subjects: Forty-nine consecutively enrolled individuals.
Methods: A surveillance system of newly-injured adults with traumatic spinal cord injury was implemented for an 18-month period. The International Spinal Cord Injury Core Data Set was used to collect data on those who survived the first 7 days post-injury.
Results: After an 18-month period, 49 incident cases were registered, of whom 45 were included in this study. The crude incidence rate was 19.0 per million, consisting mainly of men (60%), and the mean age of the cohort was 55 years (median 58). Causes of injury were almost exclusively limited to falls and transport-related events, accounting for 58% and 40% of cases, respectively. The incidence has remained stable when compared with the previous study; however, significant differences exist for injury
aetiology (p = 0.004) and impairment level (p = 0.01) in that more fall- and transport-related spinal cord injury occurred, and a larger proportion of persons was left with resultant tetraplegia, in the current study, compared with more sport-related injuries and those left with paraplegia in the previous study.
Conclusion: The incidence rate appeared to remain stable in Stockholm, Sweden. However, significant changes in injury aetiology and impairment-level post injury were found, compared with the previous study. There remains a need for developing fall-related prevention strategies in rehabilitation settings as well as in population-based programmes.
Key words: traumatic spinal cord injury; epidemiology; injury prevention; population-based cohort; core data set; incidence; aetiology; Stockholm.
Accepted Feb 23, 2017; Epub ahead of print Apr 26, 2017
J Rehabil Med 2017; 49: 00–00
Correspondence address: Conran Joseph, Karolinska Institutet, Department of Neurobiology, Care Sciences and Society (NVS), Division of Physiotherapy, 23100, SE-141 83 Huddinge, Sweden. E-mail: conran.joseph@ki.se and conran.joseph@gmail.com
The global incidence of traumatic spinal cord injury (TSCI) appears to remain relatively stable (1–3) despite aggressive efforts to curb its occurrence. Based on data from 2011, incidence rates worldwide and for Western Europe were estimated at 23 and 16 per million persons, respectively (1). Failure to reduce the incidence of TSCI may lead to an increase in its prevalence, contingent on a gradually increased life expectancy in this group, causing a potential shift in focus concerning the needs of the group ageing with injury. Limited reports of countries updating the epidemiological figures of TSCI are available, information that is necessary for developing targeted prevention strategies and informing rehabilitation services.
A centre of excellence for spinal cord injury (SCI) has recently been initiated in Sweden, with the long-term focus on establishing a more centralized approach that targets, among others, prevention, the coordination of skills and expertise, the delivery of gold-standard care, and the assessment of cost-effective care pathways. An earlier study on the epidemiology of TSCI in Stockholm, Sweden, approximately 2 decades ago, found the leading cause of injury to be transport accidents, and paraplegia the most common level of injury (4). More recently, the first prospective epidemiological study performed approximately 10 years ago (also referred to as the previous study) on TSCI in Stockholm, Sweden reported an annual crude incidence rate of 19.5 per million persons, males to be at greater risk, and falls as the leading cause of injury (5). Given the change in leading causes of injury between the 2 reports, an update on the previous prospective study is warranted in order to inform prevention programmes under the auspices of the centre of excellence. Moreover, another motivation for this study was the implementation of the International Spinal Cord Injury Core Data Set, as recommended by the International Spinal Cord Society (6), for standardizing the reporting of essential patient characteristics needed for worldwide comparison. These standards were, however, not fully implemented in the previous epidemiological study (5).
The aim of this study was to prospectively update the epidemiological figures, including incidence, aetiology and injury characteristics, of acutely-injured adult survivors of TSCI in the greater Stockholm area. A secondary aim was to compare the results with the previous study that collected data during 2006–07 (5).
All acutely-injured adults with TSCI in the greater Stockholm area, Sweden were prospectively included in this population-based cohort study. This study forms part of a larger project that evaluates the epidemiology, clinical pathways, processes of care and outcomes following acute TSCI among adults. Advantageously, the prospective, population-based methodology allows findings to hold relevance to the entire source population (7). The surveillance of incident cases was for an 18-month period that started on 1 May 2014 and ended on 31 October 2015. The Regional Board of Ethics in Stockholm approved the project prior to the start of data collection (dnr: 2014/137-31/1), whilst all other institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research. For secondary analysis purposes, a de-identified data-set is available from the authors upon request.
The registration of newly-injured persons with TSCI through a surveillance system was implemented in the greater Stockholm area, Sweden. The population size, for adults only, at the end of year 2014 was 1,722,173, after subtracting children under the age of 18 years. The healthcare pathway for the newly-injured and those living with TSCI is organized systematically in Stockholm, Sweden. Within the region, there are level 1 trauma units providing immediate and comprehensive intensive care, one spinal injury unit (providing post-acute/primary rehabilitation), 3 active rehabilitation units, and one outpatient clinic delivering lifelong follow-up care. Newly-injured patients satisfying the following criteria used in another population-based study (8) were asked to participate in this study: (i) abnormal imaging, such as with magnetic resonance imaging scan or multi-slice computerized tomography scan, confirming an acute TSCI or cauda equina lesion; (ii) the injury must result in persisting impairment (i.e. not just a concussion) after emergence from neurogenic shock, which generally occurs within the first 24–72 h after injury; (iii) age 18 years or older; (iv) surviving at least 7 days post-trauma; (v) admittance to the spinal injury unit; and (vi) legitimately residing in Stockholm, Sweden. The inclusion criteria of participant selection between the current and previous prospective epidemiological study were similar in order to aid comparison. The only difference was the duration of the study period, with the current study recruiting newly-injured persons for 18 months.
An important objective of this project was the implementation of the International Core Data Set for SCI in the acute healthcare context. The variables of the core data set cover aspects of the injury event, extent of the injury including neurological severity, and hospitalization (6). The assessment of neurological severity was performed by 2 attending physicians, also co-authors (VS and KT), on both admission to and discharge from the spinal injury unit (acute care), with the neurological characteristics of this cohort reflecting baseline data, i.e. admission to the spinal injury unit. All evaluations were done in accordance with the International Standards for Neurological Classification of Spinal Cord Injury (9, 10). In addition to the use of the core data set variables, certain variables, of the core set, were more precisely operationalized, and 2 more data elements were included. It is known that falls is the leading cause of TSCI in Sweden, therefore in order to learn more about the nature of falls, a variable capturing the height of falls (either: same level or < 1 m; 1–3 m; > 3 m) was included. Furthermore, in order to assess the timing of spinal decompression as a measure of good practice, according to acute clinical guidelines (11), we included date of spinal surgery. Concerning enrolment of participants, information about the project was provided and consent was sought once active inpatient rehabilitation commenced. In rare cases, eligible participants with very mild injuries were asked for consent whilst at the primary rehabilitation unit because they typically did not require active inpatient rehabilitation. Once consent was provided, the first (CJ) and one co-author (VS) screened the electronic medical records to retrieve the variables of interest.
Participants’ characteristics were analysed descriptively. Continuous variables were expressed as both mean with standard deviation and median with range, as recommended for the reporting of core data (12). Categorical variables were expressed as number of cases (n) and percentages. The denominator, population at risk at the start of the study and expressed as person-time, for the incidence calculation was based on the end of 2014 population figure, which was then multiplied by 1.5 (1,722,173 × 1.5 = 2,583,260), accounting for the 18-month surveillance period. Furthermore, the incidence rates with 95% confidence intervals (CI) were calculated using the Poisson distribution. The incidence rate difference was calculated to determine if statistically significant changes were noted between data from 2006–2007 and the current study. To assess associations between socio-demographic and injury characteristics, and between similarly operationalized data variables in the current and previous study, Fischer’s exact test was used because of small subgroups.
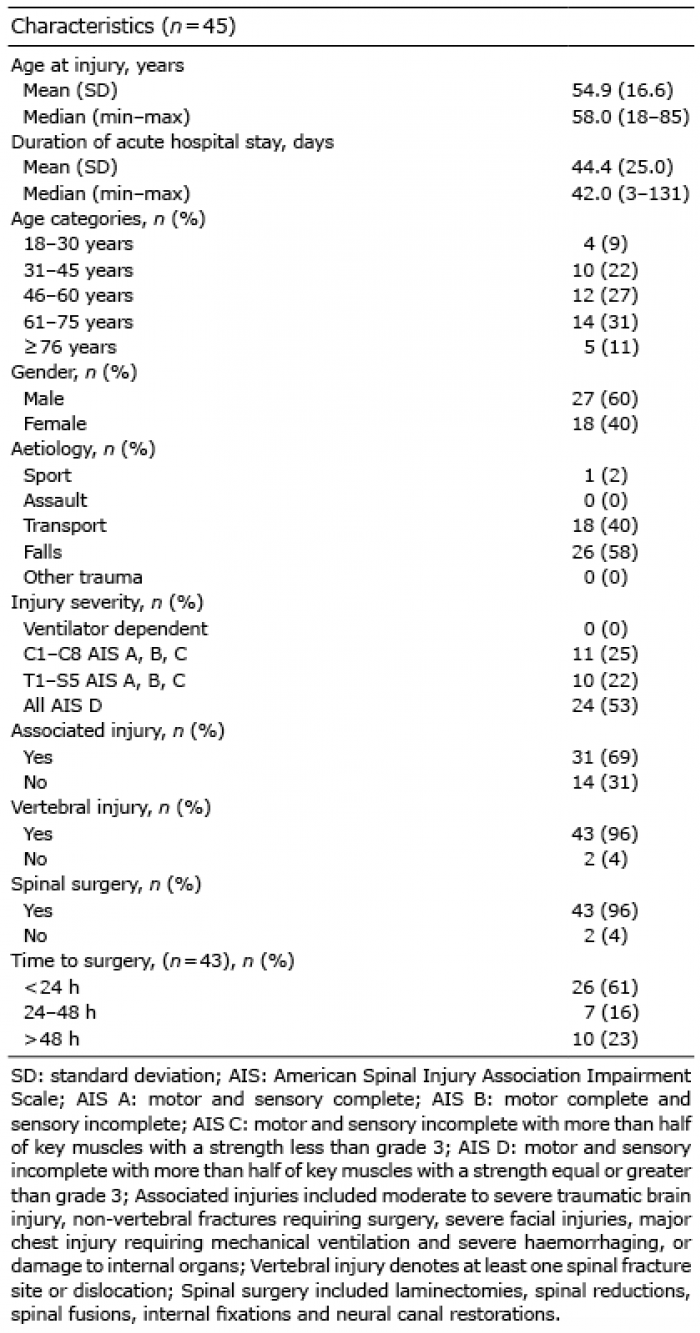
The 18-month observation period yielded 49 TSCI incident cases in the greater Stockholm area, of which 45 consented to participate in the study. The remaining 4 eligible incident cases were excluded for the following reasons: 2 declined consent; 1 died after 7 days, but consent was not yet sought and; 1 was not part of the chain of care following admission to the spinal injury unit and therefore could not be reached. As seen in Table I, the cohort was mostly male (27/45; 60%). The mean and median age of the group were 55 and 58 years, respectively, with the highest proportion of injuries occurring in the 61–75 years age group. For the first year, most injuries occurred during the summer, with 42% (11/26) of cases happening from 1 June 2014 to 31 August 2014, and during weekends. The latter finding remained consistent for the subsequent 6 months of surveillance, with 28 of the total 45 injuries happening between Friday and Sunday inclusive. Concerning additional events in TSCI, 69% of cases presented at least 1 associated injury and all but 2 had a vertebral injury.
Table I. Participant characteristics
All vertebral injuries were surgically decompressed and stabilized, with the majority (61%) of the procedures performed within the initial 24 h of injury.
The annual crude incidence rate was 19.0 (49/2 583 260) (95% CI: 14.0–25.1) per million persons. The gender-specific incidence rates were 23.6 (95% CI: 15.9–33.7) and 14.5 (95% CI: 8.7–22.6) per million males and females, respectively, with a non-significant rate difference of 9.1 (95%CI: –1.6–19.8; p = 0.09).
The aetiologies of injury were almost exclusively limited to falls and transport-related events, which accounted for 58% and 40% of injuries, respectively. Only one sport-related injury was recorded. When categorizing falls (Fig. 1) as either same level (including those under 1 m) vs higher than 3 m in the under and ≥ 60 years of age categories, we found 8 of the 10 falls in the younger age group to be from higher heights, whereas 12 of 14 falls in the older age group were from same (low) level surfaces (p = 0.02). Only one fall happened from a height between 1 and 3 m.
Fig. 1. Categorization of falls for those under and over 60 years of age.
The transport-related injuries involved a motorcycle on 9 (50%) occasions, bicycle on 7 (39%) and a motor vehicle on 1 (one case unknown). At baseline, resultant tetraplegia were confirmed in 32 of the 45 subjects, with 23 at C1–C4 (5 complete injuries) and the remaining 9 at C5–C8 (2 complete injuries). All except one of the 13 with paraplegia (6 complete injuries) had injuries in the thoracic region.
As seen in Table II, no difference in incidence rate was found between the current and previous prospective study. In the current update, the mean age at injury onset was almost 7 years older, and the cohort consisted of a higher proportion of females, compared with the previous study. A significant difference (p = 0.004) was found for the distribution of cases across aetiologies of injury, with a higher proportion of transport- and fall-related injuries in the current update. Furthermore, a significantly (p = 0.01) higher proportion of injured individuals were tetraplegic in the current study, compared with the majority being paraplegic in the previous study.
Table II. Comparison of 2006–2007 and 2014–2015 study results
Regular updates on epidemiological figures are important for noticing differences in the frequency and distribution of incident cases and determinants of injury between observation periods. The main findings revealed that the incidence remained the same for the last decade; however, significant differences were found for differences in the distribution of cases across aetiological categories and impairment level. Knowledge gained from such endeavours could be used to better target preventive strategies aimed at curbing TSCI, and plays an important role in the planning of resources for future rehabilitation. The prevention of TSCI remains a top priority in Sweden due to the impact it has on functioning and quality of life of survivors (13–15).
The annual incidence rate estimate in the current study was 19.0 per million persons, which is in line with the previous study conducted in 2006–2007 (4). This updated figure is slightly higher than the mean of 16 incident cases per million for Western Europe (1) but lower than the figures of 26.3, 25.1 and 33.5 per million in Norway (16), Finland (17) and Iceland (18), respectively. Furthermore, in line with most reports of this kind, the incidence was higher for males than females (19).
In this study, the causes of injury were almost exclusively limited to falls and transport-related events. Compared with the previous study (5), we noted a significant difference in the proportion of injuries across the different aetiological categories, with only 1 sport-related injury in the current study. Moreover, an increase in falls was noted between the 2 studies, with a noteworthy increase (24%) in the “high falls” category. We further noted a significant difference in height of falls when categorizing those under and over the age of 60 years. Low falls, 12 out of the 14, prevailed in those over 60 years of age, whereas high falls, 8 out of 10, were most common in those under 60 years of age. Possible explanations for the noted increase in high falls could be related to intentional self-harm attempts or poor judgment caused by substance abuse. These aforementioned reasons have previously been reported for TSCI cases in Sweden and other settings (4, 5, 20, 21); however, the accuracy of these should be further investigated in the context.
A similar prevalence of low falls in those over 60 years was reported in a recent Swiss-based study (19). The authors of the latter study considered primary preventive strategies for this emerging “at risk” group by adopting Haddon’s matrix (22) (a framework to conceptualize strategies) to consider conditions around the pre-event and event that could be altered in order to reduce the risk of injury. Considering “same level to < 1 m” falls in the elderly, they argued that since ageing is associated with balance issues, the preventative strategy for the host, i.e. the individual, could be strength and balance training programmes, whereas the removal of excessive loose carpets could be used as strategy for addressing the “vehicle” (energy transfer responsible for the fall) by reducing the possibility of tripping (19). Fall prevention is further considered an important area of rehabilitation considering the high incidence of falls among those with existing SCI. A recent Scandinavian-based study indicated that the majority (64%) of TSCI survivors fell within a 1-year period, with many of the falls resulting in injury (23). Haddon’s matrix further has the potential of serving as a valuable framework when considering preventive strategies for different sub-groups prone to TSCI (22).
The cohort in the current study presented mainly with tetraplegia, which is in contrast to the findings of the previous study consisting mainly of individuals with paraplegia. Although 5 with complete injuries were at the neurological levels C1–C4, none of the individuals were ventilator dependent at discharge from primary rehabilitation. All except for 2 cases had a vertebral injury; that is, either a fracture or dislocation, of which all were surgically decompressed and stabilized. Moreover, in 77% of cases, surgeries were performed within 48 h of injury, as recommended in acute clinical practice guidelines for SCI (11). “Early” surgical management after SCI is not only a hallmark feature of a specialist system approach, but has been associated with superior neurological recovery, shorter length of hospital stay, and reduced healthcare costs (24, 25).
The strength of this study was the use of a similar methodology as the previous prospective epidemiological report, in that it provides a platform to evaluate whether current prevention strategies continue to apply, or if changes in resource allocation are warranted. Moreover, this study, in contrast with the previous study, utilized the International Spinal Cord Injury Core Data Set for the description of the cohort. Concerning noteworthy limitations, only adults (≥18 years) residing in the greater Stockholm area were included in the present and previous studies, leaving a knowledge gap concerning paediatric TSCI and injuries happening in other parts of Sweden. Furthermore, very mild cases of TSCI could have been left undiagnosed, mainly at Level 2 trauma units, and thus influences the accuracy of the incidence estimate. Similarly, the methodological step of excluding cases dying within the first 7 days of injury could have influenced the estimated incidence. This was decided due to: (i) deaths occurring early after trauma are difficult to assess; (ii) difficulty of attributing TSCI as the cause of death if all investigations have not been conducted; (iii) pre-hospital deaths that are often categorized generally without a primary diagnosis given; and (iv) many early deaths occur irrespective of the treatment provided, but typically due to the severity of the injury. Lastly, with falls substantially increasing since the last report, there is a need to investigate circumstances surrounding falls, using Haddon’s matrix, especially high level falls among younger adults.
In conclusion, the incidence rate appeared not to have changed in Stockholm, Sweden, and is in line with other Western European countries. This update revealed a significant change in the distribution of injury aetiologies and level of impairment compared with the previous study, necessitating the adaptation of preventive strategies to better target those at higher risk of injury, and influence the content of and resource allocation for rehabilitation. There is a need to confirm whether the results of this study reflect the nation of Sweden in order to impact national-level policies and action plans.
The authors would like to thank all participants for their involvement in this study. This work was supported by a grant from NeuroFörbundet in Sweden.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize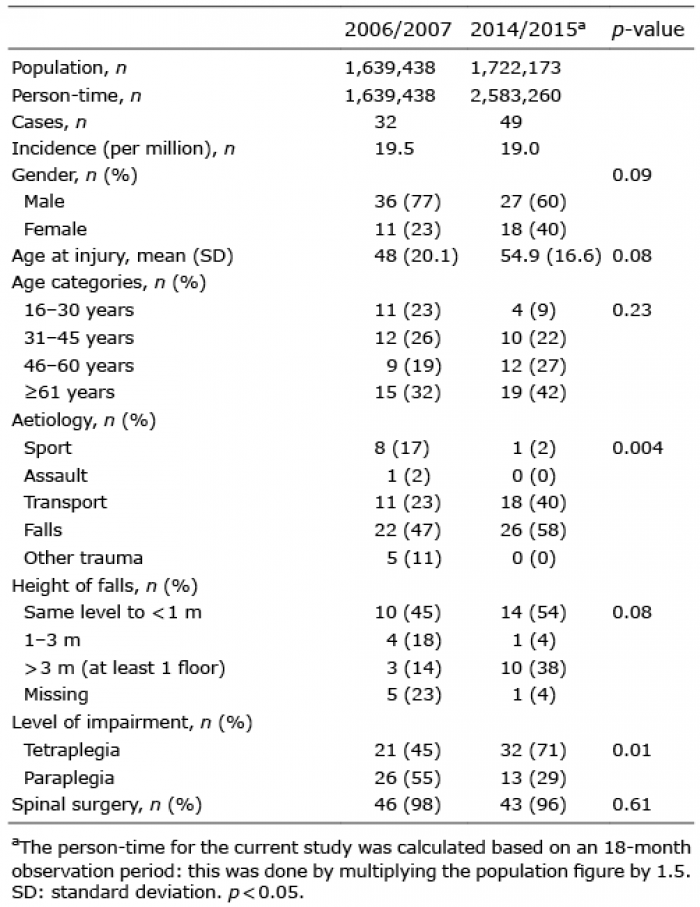 Click to show fullsize
Click to show fullsize