Ada Tang, PhD1, Janice J. Eng, PhD2, Andrei V, Krassioukov, PhD3, Teresa S.M. Tsang, MD4 and Teresa Liu-Ambrose, PhD5
From the 1McMaster University School of Rehabilitation Science, Hamilton, 2Department of Physical Therapy, 3Faculty of Medicine, Division of Physical Medicine and Rehabilitation, International Collaboration on Repair Discoveries,
4Faculty of Medicine, Division of Cardiology, 5Department of Physical Therapy, Vancouver Coastal Health, Djavad Mowafaghian Centre for Brain Health, University of British Columbia, Vancouver Coastal Health, Vancouver, Canada
OBJECTIVE: To determine the effects of high versus low-intensity exercise on cognitive function following stroke.
DESIGN: Secondary analysis from a randomized controlled trial with blinded assessors.
SUBJECTS: 50–80 years old, living in the community, > 1 year post-stroke.
METHODS: Participants were randomized into a high-intensity Aerobic Exercise or low-intensity non-aerobic Balance/Flexibility program. Both programs were 6 months long, with 3 60-min sessions/week. Verbal item and working memory, selective attention and conflict resolution, set shifting were assessed before and after the program.
RESULTS: Forty-seven participants completed the study (22/25 in Aerobic Exercise group, 25/25 in Balance/Flexibility group). There was an improvement in verbal item memory in both groups (time effect p = 0.04), and no between-group differences in improvement in the other outcomes (p > 0.27). There was no association between pre-exercise cognitive function and post-exercise improvement.
CONCLUSIONS: In contrast to a small body of previous research suggesting positive benefits of exercise on cognition post-stroke, the current study found that 6 months of high or low intensity exercise was not effective in improving cognitive function, specifically executive functions. Further research in this area is warranted to establish the effectiveness of post-stroke exercise programs on cognition, and examine the mechanisms that underlie these changes.
Key words: stroke; exercise; cognition.
J Rehabil Med 2016; 48: 841–846
Correspondence address: Ada Tang, PT, PhD, McMaster University, School of Rehabilitation Science, 1400 Main Street West, Hamilton Ontario, Canada L8S 1C7. E-mail: atang@mcmaster.ca
Accepted Sep 14, 2016; Epub ahead of print Oct 26, 2016
INTRODUCTION
Exercise and physical activity may potentially have positive benefit on cognitive function. Observational studies have suggested there may be an interplay between motor and cognitive processes, as balance ability and functional ambulatory capacity were positively associated with processing speed, response inhibition and working memory in older adults (1) and the Timed Up and Go test, a measure of functional walking and balance, was an independent predictor cognitive decline after first ischemic stroke (2). In prospective trials, resistance training contributed to improved executive functions in older adults (3), and aerobic training led to increased hippocampal volume and improved verbal memory and learning (4), and spatial memory (5).
There are some inconsistent findings however. While earlier reviews had suggested a selective benefit of aerobic training (6) or combined aerobic and resistance training on improved executive control (7), a recent Cochrane review (12 studies, 754 participants) found no benefit of aerobic exercise on any cognitive domain (8). A meta-regression of 37 studies involving 1,306 participants of all age groups also did not reveal a relationship between gains in aerobic fitness and changes in cognition (9).
It is not clear where these findings involving the general population translate to individuals with stroke, where two-thirds of cases have impairment in < 1 cognitive domain, and one-third have impaired executive function (10). Post-stroke exercise programs, while known to improve physical outcomes, have equivocal effects on cognition (11). Preliminary findings have been inconsistent, and direct between-study comparisons have been challenging due to the broad range of protocols, training modalities, and outcomes used. Ploughman and colleagues (12) found no effect of a single 20-minute bout of moderate intensity treadmill exercise on simple tests of cognition (Trail Making Test, Digit Symbol Substitution, or Paced Auditory Serial Addition Tests), hypothesizing that exercise intensity and duration, and complexity of cognitive tests were likely insufficient for changes to be observed. In single-group studies, 6 months of community exercise resulted in global improvements in cognitive function (Montreal Cognitive Assessment, MoCA) (n = 41) (13), verbal memory (Rey Auditory Verbal Learning Test) and cognitive flexibility during dual-task activities (Walking While Talking), but not working memory (Digit Span Backward Test) or task switching (Trail Making Test Part B) (n = 11) (14). Twelve weeks of combined aerobic and resistance training resulted in improved working memory (Digit Span Backwards) but not attention and executive function (Flanker Test) (n = 9) (15). These studies have generally utilized moderate training intensity (~50% VO2peak (13, 15)). Only one randomized trial (n = 38) has been conducted to date, where 8 weeks of intensive aerobic cycling (at 70% maximum heart rate) had greater effect than stretching on attention and conditional motor learning, but not selective attention and conflict resolution (Stroop Test), or working memory and task switching (Trail Making) (16). No previous study has examined a dose-response relationship with physical exercise on cognition after stroke.
The purpose of this study was to compare the effects of 6 months of high- and low-intensity community exercise for individuals with stroke verbal item and working memory, set shifting, and selective attention and conflict resolution. We hypothesized that high-intensity training lead to greater improvements than lower-intensity exercise.
METHODS
This study reports secondary findings from a prospective single-blind randomized controlled trial. The study was approved by the University of British Columbia Clinical Research Ethics Board in May 2010, with recruitment taking place from May to October 2010, and data collection taking place from October 2010 to April 2011. All participants provided informed written consent. Details of the main study are described elsewhere (17). In brief, this trial aimed to examine the effects of high and low-intensity exercise on cardiovascular outcomes in people living in the community with stroke. All assessments and exercise classes took place in multi-purpose spaces in a research facility. To minimize the risk of contamination, the exercise classes took place in different spaces within the facility and at different times of the day so that participants had little opportunity to interact.
Clinical Trial Registration; http://www.clinicaltrials.gov. Unique identifier: NCT01189045.
Eligibility criteria
Participants 50–80 years old were eligible if they were > 1 year post-stroke, able to walk ≥ 5 m, and free from stroke from aneurysm, tumor, or infection or significant health conditions that would preclude participation in exercise (presence of cardiovascular abnormalities, pacemaker, serious musculoskeletal or other conditions). Participants were initially assessed for eligibility via telephone screening, and subsequently underwent further screening during an in-person assessment.
Participants
Participant characteristics were recorded, as well as details of stroke (time post-event, type, location, limbs affected). Severity of stroke and motor recovery were assessed using the National Institutes of Health Stroke Scale (18) and the Chedoke-McMaster Stroke Assessment (19), respectively. The MoCA (20, 21) and Center for Epidemiologic Studies – Depression Scale (22) were used to characterize baseline cognitive function and presence of depressive symptoms. Aerobic capacity was measured using a graded maximal exercise cycle ergometry test for breath-by-breath gas exchange (ParvoMedics, Sandy UT, Excalibur, Lode Medical Technology, Groningen NL) (17), walking ability was assessed using 5-m self-selected gait speed and the 6-Minute Walk Test (6MWT) (23), and functional balance was evaluated using the Berg Balance Scale (24). Participant characteristics are presented in Table I.
|
Table I. Baseline characteristics |
|||
|
Aerobic exercise n = 25 |
Balance and flexibility n = 25 |
p-value for group differences |
|
|
Age, years, median (IQR) |
66 (62–71) |
64 (62–75) |
0.95 |
|
Men/Women, n (%) |
14 (56)/11 (44) |
15 (60)/10 (40) |
0.77 |
|
Type, n (%) Lacunar/Ischemic/Hemorrhagic/Unknown |
3 (12)/7 (28)/9 (36)/6 (24) |
4 (16)/12 (48)/7 (28)/2 (8) |
0.72 |
|
Location, n (%) Cortical/Subcortical/Brainstem/Unknown |
4 (16)/7 (28)/5 (20)/9 (36) |
6 (24)/7 (28)/9 (36)/3 (12) |
0.07 |
|
Limbs affected, R /L/Bilateral, n (%) |
10 (40)/15 (60)/0 (0) |
8 (32)/16 (64)/1 (4) |
0.53 |
|
Time post-stroke, years, median (IQR) |
3.5 (2.2–6.7) |
2.3 (1.8–5.1) |
0.48 |
|
National Institutes of Health Stroke Scale |
1 (0–4) |
0 (0–2) |
0.27 |
|
Center for Epidemiologic Studies – Depression scale, median (IQR) |
4 (1–7) |
6 (3–10) |
0.08 |
|
Montreal Cognitive Assessment, median (IQR) |
26 (23–28) |
25 (21–27) |
0.42 |
|
Chedoke-McMaster Stroke Assessment, median (IQR) Upper limb Lower limb |
14 (6–14) 13 (11–14) |
13 (12–14) 12 (11–14) |
0.86 0.49 |
|
Gait aids used, None/Cane/Walker, n (%) |
13 (52)/10 (40)/2 (8) |
17 (68)/5 (20)/3 (12) |
0.21 |
|
Aerobic capacity, mlkg-1min-1, median (IQR) |
14.0 (12.9–19.8) |
16.2 (11.5–22.0) |
0.62 |
|
6-Minute Walk Test distance, m, median (IQR) |
287 (179–383) |
301 (226–446) |
0.38 |
|
Gait speed, m/s, median (IQR) |
0.92 (0.48–1.25) |
0.96 (0.71–1.17) |
0.64 |
|
Berg Balance Scale score, median (IQR) |
50 (48–54) |
51 (44–56) |
0.95 |
|
IQR: interquartile range. |
|||
Cognition and executive function outcome measures
Participants were assessed within one month before and after the program by trained assessors, all with backgrounds in kinesiology or physiotherapy. Assessors were not involved in the interventions, and thus were unaware of participants’ group allocation.
The Verbal Digit Span (25), Trail Making Part B (26, 27), and Stroop Tests (28) were used to evaluate the effects of exercise on cognitive function. These were selected based on the prevalence of memory impairment, and difficulties with executive functions commonly observed after stroke. These outcome measures have also been used in previous single-group (12, 14, 15) and randomized controlled (16) exercise studies involving individuals with stroke. Working memory was measured with the Verbal Digit Span Test (25), where random number sequences of increasing length were presented verbally to the participant, who then relayed the numbers back to the examiner either in forward or reverse order. One point was scored for each correct sequence relayed (maximum score 14). Higher scores indicate better performance. The Verbal Digit Span Backwards Test has been shown to have adequate internal consistency and moderate test-retest reliability in healthy adults across the lifespan (29) and concurrent validity with the Executive Function Performance Test in people with stroke (30). Set shifting was assessed using the Trail-Making Test Part B (26, 27), where participants traced a line alternating between encircled numbers and letters (i.e. 1-A-2-B-3-C etc.). The test was timed (maximum 300 s), where shorter times indicate better cognitive flexibility. The Trail-Making Test Part B has good test-retest reliability in people with stroke (31, 32). The Color-Word Stroop test is a reliable test of selective attention and conflict resolution (28), whereby the participant identifies the ink color of words presented in incongruent colored inks (e.g. the word blue printed in red ink). The time (in sec) required to complete the test was recorded. Shorter times indicate better performance.
Interventions
Participants were randomized into one of two 6-month intervention programs of either high or low intensity exercise (17). In brief, participants in the high-intensity Aerobic Exercise (AE) training program were provided with an individualized exercise program that was performed 3 times/week in 60-min exercise classes. Exercise intensity progressed in intensity from 40 to 80% of heart rate reserve. Activities in the low-intensity Balance and Flexibility (BF) program were also performed 3 times/week for 60 min/session, but intensity remained below 40% heart rate reserve.
Participants were stratified based on age (65 years old) and 6-Minute Walk Test distance (300 m). Randomization was performed using a 1:1 allocation sequence and permuted block sizes of 2 or 4. Groups were held at different times of the day to minimize the risk of contamination.
Statistical analyses
The sample size for the larger trial was based on an expected 10% change in aerobic capacity (33) and determined to be n = 24 per group (two-tailed type I error 0.05; type II error 90%; SD 3).
Descriptive statistics were performed for all participant characteristics, and groups were compared at baseline using Mann-Whitney U tests and chi-square analyses. Mann-Whitney U tests were used to compare change scores between the groups, and Wilcoxon Signed Rank Tests were used to determine if there were changes in time across both groups. Effect sizes were calculated and defined as small: 0.1, medium: 0.3 and large: 0.5 (34). Further, we sought to determine if baseline (pre-exercise) cognitive function was associated with the degree of improvement following the exercise program. As such, bivariate correlational analyses were performed to examine if there were associations between baseline global cognitive functional level (MoCA score) and post-program changes in cognitive outcomes. Statistical Package for the Social Sciences (Version 20.0, Chicago IL) was used, with a significance level of p < 0.05.
RESULTS
The flow of participants through the study is presented in the Fig. 1. Fifty participants were randomly allocated to the intervention groups. Characteristics and pre-training scores cognitive outcomes for the 50 participants who enrolled in the study are presented in Table I and II, respectively. There were no differences between the groups.
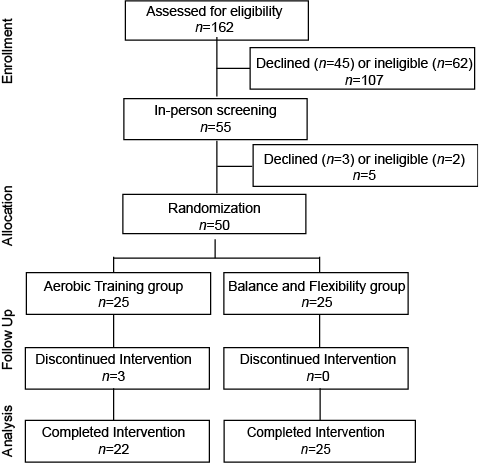
Fig. 1. CONSORT diagram depicting participant flow through the study.
|
Table II. Baseline scores for cognitive measures |
||||||
|
Aerobic Exercise |
|
Balance and Flexibility |
p-valuea |
|||
|
n |
Median (IQR) |
n |
Median (IQR) |
|||
|
Verbal Digit Span Test, n digits |
||||||
|
Forward |
25 |
8 (5–10) |
25 |
7 (5–10) |
0.80 |
|
|
Backward |
25 |
3 (2–6) |
25 |
2 (2–4) |
0.72 |
|
|
Trail Making Test B, s |
22 |
127.2 (90–178) |
25 |
161.0 (95–249) |
0.41 |
|
|
Color–Word Stroop Test, s |
22 |
111.7 (101–143) |
24 |
131.7 (110–188) |
0.19 |
|
|
aSignificance between groups. IQR: interquartile range. |
||||||
Class attendance rates were 81.4% and 80% for the BF and AE group, respectively, and intensity targets for both groups were achieved (exercise heart rate < 16.8% heart rate reserve throughout the BF program, while participants in the AE group progressed to 58.1% heart rate reserve by the end of the intervention).
Three of the 50 participants were lost to follow-up for reasons unrelated to the intervention. These were deemed cases missing completely at random, thus complete-case analyses were performed from 47 participants who completed the main study (22 of 25 in the AE group, 25 of 25 in the BF group). Of these, 11 (44%) participants in the AE group and 14 (56%) participants in the BF group had baseline MoCA scores < 26. Pre- and post-program changes in cognitive outcomes are presented in Table III. Data were missing for 3% of the cognitive data due to significant aphasia (n = 4) and difficulty understanding test instructions (n = 1). For missing post-training data points, baseline scores were carried forward (n = 2 for Stroop test). For those with missing pre-training data points, these participants were excluded from the analysis.
|
Table III. Changes in working memory, set shifting, selective attention and conflict resolution |
|||||||||||
|
Aerobic Exercise |
Balance and Flexibility |
p-values |
Effect size |
||||||||
|
n |
Baseline Median (IQR) |
Post Median (IQR) |
n |
Baseline Median (IQR) |
Post Median (IQR) |
Differences over timea |
Differences in change scores by groupb |
||||
|
Verbal Digit Span Test, n digits |
|||||||||||
|
Forward |
22 |
8 (5–9) |
8 (6–9) |
25 |
7 (5–10) |
7 (7–9) |
0.04 |
0.49 |
–0.10 |
||
|
Backward |
22 |
3 (0–6) |
2.5 (1–5) |
25 |
2 (2–4) |
3 (2–4) |
0.91 |
0.18 |
–0.20 |
||
|
Trail Making Test B, s |
19 |
128.9 (90–179) |
131.6 (96–179) |
25 |
161.0 (95–249) |
163.5 (95–243) |
0.54 |
0.68 |
–0.06 |
||
|
Color-Word Stroop Test, s |
20 |
108.5 (100–144) |
122.0 (97–141) |
24 |
131.7 (110–188) |
141 (106–193) |
0.98 |
0.38 |
–0.13 |
||
|
aWilcoxon Signed Rank test, bMann-Whitney U test. IQR: interquartile range. |
|||||||||||
Both groups improved in the Verbal Digit Span Forward Test (p = 0.04), but there were no differences in change scores between groups in any outcome (all p > 0.18). Upon inspection of the data of the Color-Word Stroop Test, two participants were identified as outliers (> 2 standard deviations from mean). These participants were removed for secondary analyses, but there were no changes in the study results. Complete case analyses yielded similar results (all p > 0.18).
Secondary bivariate correlation analyses were performed to determine whether MoCA score at baseline was associated with changes in cognitive outcomes (Table IV). There may be an inverse relationship between baseline MoCA score and change in Digit Span Forward test, but this was not significant. There was no change in the results when the outlier data from the Color-Word Stroop Test were removed (rho=0.05, p = 0.76).
|
Table IV. Correlation analyses for baseline Montreal Cognitive Assessment (MoCA) score and change in cognitive outcomes |
|||
|
Change in |
Baseline MoCA score |
||
|
n |
rho |
p |
|
|
Verbal Digit Span Test |
|||
|
Forward |
44 |
–0.30 |
0.052 |
|
Backward |
44 |
0.16 |
0.30 |
|
Trail Making Test B |
42 |
0.11 |
0.51 |
|
Color-Word Stroop Test |
44 |
0.15 |
0.32 |
DISCUSSION
Despite early reports suggesting the potential benefits of post-stroke exercise training on cognitive function, we observed improvement in short-term memory across both groups, but not in any of the other measures of cognition (working memory, set shifting, conflict resolution) following high or low intensity exercise among community-dwelling individuals with stroke.
There are several possible explanations for the lack of significant findings. The specific outcomes used in this study were not sufficiently sensitive for detecting changes in this specific subset of the stroke population or that the effects of exercise are more specific to certain cognitive domains than others, as Quaney and colleagues reported improved attention and motor learning following post-stroke exercise, but not executive functions (16). The exercise parameters (frequency, intensity, time, type) used in this study may not have been sufficient to accrue benefits to cognitive function. While training intensity is the most important parameter for improving exercise capacity, its importance for improving cognitive function is not known. Previous research has generally utilized moderate levels of training intensities that were similar to those of the intervention group in the current study, typically ranging from 40% to 70% of heart rate reserve (13) or maximum heart rate (16). It has been postulated that intensive exercise may enhance cognitive performance through increases in cerebral blood flow (15) or bioavailability of neurotrophins (7, 35). We did not observe changes in either the high or low intensity exercise group, suggesting that intensity may not be a mediating factor for cognitive improvement after stroke. Rather, program duration may be a more important factor as meta-analytic data in the older adult population has suggested that fitness programs of > 6 months have the greatest effect on cognitive function (7). While the body of evidence for exercise effects on post-stroke cognition is still relatively young, perhaps longer durations are also needed for this population that commonly presents with cognitive impairment.
The most effective training type is also not well established. Most of the previous research in this area has focused on physical exercise, whether it was aerobic only (16) as was done in the current study, or combined aerobic and resistance training (13–15). The specific mechanisms underlying exercise-related improvements in cognition are unknown, particularly after stroke, but the type of training utilized has been hypothesized as a mediating factor. Aerobic exercise may improve cerebral blood flow and perfusion thereby contributing to better cognitive performance (15), and be associated with enhanced neurotrophin availability that can promote neuroplasticity and recovery following stroke (35). Though not specific to exercise, a meta-analysis of trials using motor or cognitive skills training that also acquired neuroimaging data in healthy young adults found changes in functional brain activity, such as decreased activation of frontoparietal control and dorsal attention networks that suggest lower demands on externally-focused attention, and increased activation of the default network that would typically be observed with low attentional demands and low task difficulty (36). While these neuroimaging data do not necessarily correlate with behavioral changes, these results can provide insight into potential mechanisms underlying the effects of training on function. In animal models, treadmill exercise was associated with increased cortical levels of brain-derived neurotrophic factor (BDNF) (37), and preliminary work in humans has demonstrated that exercise-related improvements in post-stroke cognition are associated with increased serum BDNF levels (38).
Exercise may potentially have differential effects on different domains of cognitive function after stroke. In a recent systematic review of aerobic exercise training parameters on cognitive outcomes in humans with stroke, low–moderate intensity training can improve working memory, and short-term training (8–12 weeks) can improve learning, but little evidence that aerobic training alone was beneficial for executive functions (39). It is possible that aerobic training may result in greater improvement in general function associated with increased alertness and attention whereas higher order cognitive functions, such as executive functions, may require more complex interventions than aerobic training alone. Combination therapies or greater intensities and longer durations may be needed (39), and physical interventions such as exercise may serve as effective complements to dedicated cognitive rehabilitation programs. Future studies may elucidate the mechanisms that underlie cognitive improvements resulting from exercise training, and examine the differential effects of various modes, modalities, and types of training, such as aerobic only vs. combined aerobic and resistance training, or physical only vs. combined physical and cognitive training (40). We observed improvements in the Digit Span Forward Test across the entire cohort, which can carry over to improved short-term memory. Nonetheless, understanding the most effective strategies to optimize other domains of cognitive function after stroke will have important implications for rehabilitation programs, and may provide further evidence-based support for interdisciplinary efforts between physiotherapists, occupational therapists and neuropsychologists.
Arguably, we did not enroll participants who would be unsafe or unable to participate in exercise if they presented with significant cognitive impairment, and thus did not explicitly examine exercise-associated effects on cognition among individuals who presented with impaired function. It is possible that the lack of positive findings may be attributed to including individuals without cognitive impairment who would not necessarily demonstrate a great degree of improvement. While preliminary research has observed improvements in cognitive function following post-stroke exercise, much of these previous studies enrolled participants with stroke with participants normal or near-normal cognitive functioning (study eligibility criterion with Mini-Mental Status Examination score ≥ 23 (15) or higher (12, 14, 16). Results from these studies suggest that the presence of impairment may not be necessary for exercise to have benefit. Nonetheless, future research should focus on examining the effects of exercise interventions in individuals who present with impaired cognition to establish its effects on cognitive function.
There may be additional factors not examined in this study that can explain the lack of significant findings. Stroke-related factors, such as lesion location (left hemisphere stroke), infarct volume and presence of multiple infarcts, are associated with post-stroke dementia (41), and the presence and extent of white matter lesions have been shown to be associated with cognitive impairment (42, 43). The extent of these lesions is indicative of small vessel cerebrovascular disease progression, and individuals with greater lesion load may have less capacity for improved cognitive function following an intervention. Future work may focus on these and other potential mediating factors, including stroke severity, hemisphere affected, time post-event, program-related considerations such as duration, intensity, or type of training, or individual factors such as age, gender, pre-stroke cognitive function, or other baseline characteristics.
Arguably, a key limitation of this study was that it was secondary analysis of data from a randomized trial aimed to examine the effects of high- and low-intensity exercise on cardiovascular, not cognitive, outcomes after stroke. The sample size of the main trial was established to detect changes in the primary outcome, aerobic capacity, and not explicitly to detect changes in cognitive function. It is possible that the current analysis was insufficiently powered to detect changes in selected outcomes of cognition and executive function. Nonetheless, this study is the largest randomized controlled trial to date that has reported on changes in cognitive function following post-stroke exercise. That we did not observe improvements in any of our outcomes contributes to the equivocal findings of the current body of evidence, underscoring the need for ongoing research to establish the effectiveness of exercise interventions on cognitive function after stroke.
Conclusions and implications
No changes in cognitive function were observed following high- and low-intensity exercise after stroke. The jury is still out whether post-stroke exercise interventions have broader effects on health and function beyond physical outcomes alone. This study provides preliminary data that can be used for power calculations for future studies. Given the prevalence of physical and cognitive impairments that persist after stroke, ongoing work is needed to establish the effectiveness of exercise and cognitive function in this population, develop optimal training parameters, and examine underlying mechanisms that mediate change.
ACKNOWLEDGEMENTS
This study is funded by the Vancouver Foundation/Carl and Elsie Halterman Research Fund and the Canadian Institutes of Health Research (CIHR) (MOP-111183). AT was supported by a personnel award from the Heart and Stroke Foundation, Ontario Provincial Office (CS I 7468), the Canadian Institutes of Health Research (MFE-98550) and the Michael Smith Foundation for Health Research (MSFHR) (ST-PDF-03003(11-1)CLIN), and JJE was supported by the CIHR (MSH-63617) and the MSFHR. TLA is a Canada Research Chair in Physical Activity, Mobility, and Cognitive Neuroscience.
The authors declare no conflicts interests.
References

