Rachelle Pretz, PT, DPT1, Cora Brown, MD2, William B. Hughes, MD3 and Eric L. Altschuler, MD, PhD1,2
From the 1Department of Physical Medicine and Rehabilitation, Temple University Hospital, 2Department of Physical Medicine and Rehabilitation, Lewis Katz School of Medicine at Temple University and 3Temple University Hospital Burn Center, Philadelphia, PA, USA
OBJECTIVE: Injury to the foot and ankle without involvement of the knee, requiring a patient to become non-weight-bearing or even needing amputation, is a common problem resulting from diverse causes, including diabetic foot ulcers and trauma. The patellar tendon bearing orthosis may be a good option for patients who would functionally deteriorate, attempting to live their lives without the use of a leg. This brace was introduced 58 years ago; however, it is under-utilized clinically and under-represented in the literature.
CASE REPORT: A 25-year-old man with severe electrical burn injuries resulting in an unstable ankle who, through the use of patellar tendon bearing orthosis and therapeutic rehabilitation, was able to walk at a supervision level without additional assistive devices.
CONCLUSION: The patellar tendon bearing orthosis is recommended, not only for other burn patients who are unable to weight-bear through their ankle-foot complex, but for other patients, such as trauma patients, to allow for ambulation.
Key words: patellar tendon bearing orthosis; electrical injury; burn injury; non-weight-bearing.
J Rehabil Med 2016; 48: 00–00
Correspondence address: Rachelle Pretz, Department of Physical Medicine and Rehabilitation, Temple University Hospital, Philadelphia, PA, USA. E-mail: rachelle.pretz@tuhs.temple.edu or Eric L. Altschuler, Department of Physical Medicine and Rehabilitation, Lewis Katz School of Medicine at Temple University, 3401 N. Broad Street, Philadelphia, PA 19140, USA. E-mail: eric.altschuler@temple.edu
Accepted Apr 21, 2016; Epub ahead of print Jun 1, 2016
INTRODUCTION
Complications of third-degree burns are numerous, ranging from hypertrophic scar, contracture formation, infection, electrolyte imbalances to tissue loss. Extensive tissue and muscle loss around the weight-bearing joints of the lower limbs, such as the foot-ankle complex, can lead to immobility in patients with deep tissue burns. To mitigate this challenge, the patellar tendon bearing (PTB) orthosis was designed to offload the foot-ankle joint and to shift weight-bearing onto the knee joint. The PTB orthosis has been studied in diabetic patients with tissue loss of the lower limbs (1). A review of the literature on burns reveals that PTB orthosis has been used to treat one paediatric patient with equinovarus deformities post-thermal injury (2). We describe here the first case of a patient who was unable to bear weight through the foot-ankle complex due to a fibulectomy resulting from a severe circumferential third-degree burn, but who could ambulate successfully with the use of PTB orthosis and make progress in his daily rehabilitative programme.
CASE REPORT
We treated a 26-year-old man who sustained a severe high voltage electrical injury with 70% total body surface thermal burns of second- and third-degree level of injury when he came into contact with an electrical transformer. Prior to injury the patient had had normal independent functional and vocational levels.
Physical examination revealed second- and third-degree burns over the right side of the face, anterior chest, trunk, abdomen, groin (including the scrotum), bilateral upper limbs, anterior thighs and ankles. Computed tomography (CT) scan of the spine revealed a T12 superior endplate fracture, but no fracture of cervical and lumbar spines, requiring a thoracolumbosacral orthosis (TLSO) brace wear for approximately 12 weeks when the patient was out of bed. Hospital course included multiple escharotomies and skin grafts to the left ankle and exploratory laparotomy due to abdominal compartment syndrome. He was initially intubated for airway protection, then extubated.
The patient’s left ankle sustained a severe circumferential third-degree burn (Fig. 1A) necessitating a fibulectomy (Fig. 1B); multiple wound debridement procedures, dermal template placement and skin grafting.
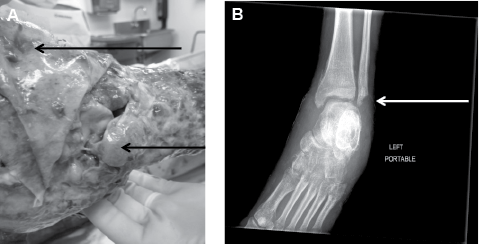
Fig. 1. Left ankle. (A) After debridement. Top arrow: distal foot. Bottom arrow: lateral malleolus. Lateral ligament destruction is evident. (B) Left ankle radiograph fibulectomy (arrow).
Neuromuscular examination revealed bilateral hands with flexion contractures at the proximal and distal interphalangeal joints. Active range of motion (ROM) of bilateral elbows was normal. Active and passive ROM of bilateral shoulders was limited to 100° scaption secondary to scarring. Active ROM of the lower limbs was notable for bilateral hip flexion deficits secondary to pain from open gluteal wounds. Bilateral knee active ROM was normal. The patient had right ankle passive dorsiflexin to neutral. The left ankle was in a plantar flexion deformity with passive range of motion limited by pain to 15 degrees from neutral. There was no equinovarus deformity. Sensory examination revealed decreased sensation to light touch and pin prick in all dermatomal distributions of the upper and lower limbs.
Motor examination was performed using manual muscle testing and grading on the Medical Research Council scale. Bilateral upper limbs showed 3/5 shoulder abduction, elbow flexion and extension in the available range. Bilateral wrist extension was 0/5, and finger abduction and adduction in all fingers 1/5. Motor examination of bilateral lower limbs showed 4/5 hip flexion, hip extension, knee extension, knee flexion, and 0/5 ankle dorsiflexion and plantarflexion at the ankles. The patient was wearing a custom fabricated PTB orthosis on the left and a platform shoe on the right. The patient was normally alert and oriented with normal mentation.
The patient’s goal from therapy was to walk independently and decrease the burden of care on his family. Because of his burns the patient had impairments to his body structures, including decreased skin integrity, peripheral nervous system damage, and decreased ankle stability, all of which affected his ability to ambulate. Inability to ambulate independently meant increased burden of care in getting food for himself, dressing, toileting and other aspects of self-care. His ability to walk was also impacted by personal factors, including his assertiveness in having nurses walk with him and overall daily motivation to get out of bed. Environmental factors also impacted his ambulation; the brace had to be fabricated and adjusted and therefore was not available as soon as it was deemed unsafe to weight-bear through his left foot. The patient’s level of disability is summarized in Fig. 2 using the International Classification of Functioning, Disability and Health (ICF).
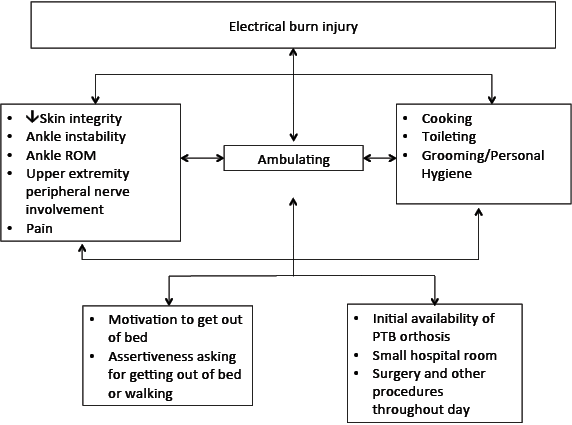
Fig. 2. Level of disability using the International Classification of Functioning, Disability and Health (ICF).
Initially, the patient was at a dependent level functionally, requiring an overhead lift for transfers out of bed and 2-person assistance for mobility in bed. The patient was limited to walking 5 feet, with the maximum assistance of 2 therapists because of instability and severe pain (10/10 on a standard 0–10 visual analogue scale) when weight-bearing through the foot and ankle. Orthopaedic surgery made the patient non-weight-bearing through the left ankle 1 month after hospitalization and it was decided that the ankle would need to be surgically fused once there was skin closure of the wounds. At this time it was determined to initiate the PTB orthosis. The patient’s functional status slowly improved throughout his hospitalization. Four months after injury he was able to ambulate 30 feet with a right platform shoe (Fig. 3A) and a left PTB orthosis (Fig. 3B, C) at a supervision level with (Video 1 (front view)1, Video 2 (lateral view)1) without an assistive device. The patient demonstrated fair dynamic and static standing balance. For sit-to-stand the patient was at a minimal assistance to supervision level. He remained at maximal assistance with upper and lower extremity dressing, including donning and doffing the PTB orthosis and right platform shoe. He was modified independent with feeding and grooming using a right-hand universal cuff and adaptive or modified instruments.
The wearing schedule for the brace was that it be used for all times that the patient was out of bed, or approximately 8 h each day, with most of that time being spent in a chair. Pain when using the PTB orthosis was 3–8/10 (VAS scale).
The PTB orthosis (Fig. 3B, C) was custom-made (Bo Powers, Lawall Prosthetics and Orthotics, Philadelphia, PA) with a moulded socket, metal joints, double adjustable ankle joints, a shoe with steel shank and a T-strap, and a proximal pull strip holding the anterior shell to the patella.

Fig. 3. Lower extremity braces. (A) Right lower extremity platform shoe. (B) Front view left lower extremity patellar tendon bearing (PTB) orthoses. (C) Lateral view left lower extremity PTB orthoses.
Throughout the patient’s treatment the skin integrity of the left knee was monitored. The skin of the knee, which contacted the brace, was intact, non-burned skin, at initiation of the PTB orthosis. The skin was protected with a cotton prosthesis sock while the brace was being worn. The brace was worn only while the patient was out of bed. A caregiver donned the brace for the patient every morning; skin integrity was checked prior to therapy and during wound care. There was no skin breakdown during the described treatment time.
DISCUSSION
We describe here the case of a patient with a very severe electrical burn injury, non-weight-bearing on his ankle, who was able to walk with a PTB orthosis without other assistive device. The PTB orthosis was introduced in 1958 (3), but it is used rather rarely now. There are only a few published reports on the brace (1, 2, 4–7), typically reporting great benefit, but for specialized uses (1, 4, 5) and only one of the papers (6) has been cited even a few times. The case described here is an exemplar of how the PTB orthosis could be of great and common use potentially for many thousands of patients with injuries due to natural disasters, war or other traumas. In the acute care phase of hospitalization, specialized teams are present for a short time (8) and an ankle or foot can be operated on or set and casted, then the patient can walk independently, with the PTB orthosis allowing the foot and ankle to remain non-weight-bearing, with the orthosis being discarded when no longer needed. Improvements in materials, scanning technology, manufacturing techniques, 3-D printing, and supply chain fulfilment and delivery mechanisms over the past 6 decades should permit custom PTB orthoses to be available when needed. The ability to ambulate is of great functional benefit and prevents secondary complications, such as decubitus ulcers. These advantages should vastly offset the cost of what, in some cases, will be a possibly disposable orthotic. In addition, the psychological benefits of being able to walk independently are immeasurable.
With an intact knee a patient can use a PTB in lieu of strict offloading through the foot. The PTB orthosis gives patients the ability to have more normalized gait, bear weight through the long bones of the affected leg, and decrease the amount of assist needed by the upper extremities and contralateral leg, which could result in overuse injuries. Another orthosis that would unload weight-bearing on the foot and ankle is a Charcot Restraint Orthotic Walker (CROW) boot, although the effect is not significant as with a PTB orthosis.
Limitations of the PTB orthosis also need to be considered. Skin integrity of the weight-bearing surface (patellar tendon) needs to be closely monitored for tears, abrasions, and irritation. Equinus deformity of the involved leg will necessitate more lift or platform to the contralateral leg. Also, some skill is needed to don the PTB brace, to ensure that the patient is only putting weight through their patellar tendon.
Future research should identify more populations in a variety of healthcare systems that may benefit from a PTB orthosis.
In conclusion, the utilization of the PTB orthosis has been described in several clinical settings, but reports of its use are limited in treating burn patients who are unable to bear weight via the foot-ankle complex due to high-degree burns. The case reported here shows that the PTB orthosis could be an excellent bridging therapy to assist burn patients in ambulating independently while waiting for definitive surgical management of the ankle. Our case suggests that the PTB orthosis may also be useful in other trauma and disaster situations.
Conflicts of interest. The authors report no financial or other conflicts.

1http://www.medicaljournals.se/jrm/content/?doi =10.2340/16501977-2114
REFERENCES
1http://www.medicaljournals.se/jrm/content/?doi =10.2340/16501977-2114


