
From the 1Spinal Cord Injury Centre of Western Denmark, Department of Neurology, Regional Hospital of Viborg, Viborg, 2Clinic for Spinal Cord Injuries, Rigshospitalet, University of Copenhagen, Copenhagen, Denmark, 3Department of Clinical Medicine, University of Bergen, Bergen, Norway, 4The Autonomic Unit, National Hospital for Neurology and Neurosurgery, Queen Square, University College London, UK, 5Hammel Neurorehabilitation and Research Centre, Hammel, 6Department of Neurology, Aarhus University Hospital, Aarhus 7Danish Pain Research Center, Department of Clinical Medicine, Aarhus University, Aarhus, Denmark
Objective: To evaluate recreational and medical cannabis use in individuals with traumatic spinal cord injury, including reasons and predictors for use, perceived benefits and negative consequences.
Design: Cross-sectional survey in Denmark.
Methods: A 35-item questionnaire was sent to 1,101 patients with spinal cord injury who had been in contact with a rehabilitation centre between 1990 and 2012.
Results: A total of 537 participants completed the questionnaire. Of these, 36% had tried cannabis at least once and 9% were current users. Of current users, 79% had started to use cannabis before their spinal cord injury. The main reason for use was pleasure, but 65% used cannabis partly for spinal cord injury-related consequences and 59% reported at least good effect on pain and spasticity. Negative consequences of use were primarily inertia and feeling quiet/subdued. Lower age, living in rural areas/larger cities, tobacco-smoking, high alcohol intake and higher muscle stiffness were significantly associated with cannabis use. Those who had never tried cannabis reported that they would mainly use cannabis to alleviate pain and spasticity if it were legalized.
Conclusion: Cannabis use is more frequent among individuals with spinal cord injury in Denmark than among the general population. High muscle stiffness and various demographic characteristics (lower age, living in rural areas/larger cities, tobacco-smoking and high alcohol intake) were associated with cannabis use. Most participants had started using cannabis before their spinal cord injury. There was considerable overlap between recreational and disability-related use.
Key words: spinal cord injury; traumatic; pain; spasticity; cannabis; survey.
Accepted Nov 16, 2016; Epub ahead of print Jan 18, 2017
J Rehabil Med 2017; 49: 152–160
Correspondence address: Sven R. Andresen, Spinal Cord Injury Centre of Western Denmark, Department of Neurology, Regional Hospital of Viborg, Heibergs Allé 4, DK-8800 Viborg, Denmark. E-mail: sven.robert.andresen@midt.rm.dk
Pain and spasticity are common sequelae of spinal cord injury (SCI), with approximately 80% of individuals with SCI reporting pain and 70% reporting spasticity. Both conditions are often insufficiently treated and have a negative impact on patients’ quality of life (1–3).
Cannabis is widely used for psychoactive and medical purposes because of its content of bioactive cannabinoids. The cannabinoid system plays a role in inhibiting synaptic transmission and controlling synaptic plasticity in pain and motor pathways through activation of the G-protein-coupled cannabinoid receptors CB1 and CB2. The 2 best-studied constituents of cannabis are Δ9-Tetrahydrocannabinol (THC), which binds preferentially at CB1 receptors and has high psychoactive effects and abuse potential, and cannabidiol (CBD), which has limited psychoactive effects (4). Individuals with SCI have, in several studies, reported that cannabis use relieves their pain and spasticity (5, 6), but our knowledge of the extent and characteristics of cannabis use in the SCI population in Denmark is inadequate.
A number of studies in the general population and specific disease populations have found that anxiety, stress, pain, depression, nausea, appetite stimulation, sleep improvement, alleviation of muscle spasms, spasticity, facilitation of pleasure and partying are commonly given as reasons for using cannabis (7–10). Cannabis users more often smoked and drank alcohol than non-users and had more often tried cannabis in early adolescence, were younger, more often males and had lower income and lower socioeconomic status than non-users (11, 12). In individuals with HIV, lower income, tobacco smoking, ecstasy use and living in a rural areas were associated with cannabis use (9), while in a study of multiple sclerosis, tobacco-smoking, greater disability according to patients’ self-evaluation (especially in the lower limbs), and marriage or being in a stable relationship were associated with cannabis use (7).
The main aim of the current study was to evaluate the use of recreational and medical cannabis in a nationwide population with traumatic SCI in Denmark, including predictors and reasons for use, benefits and negative consequences. A secondary aim of this cross-sectional survey in Denmark was to determine the prevalence, severity and impact of pain and spasticity in this population. These results were reported earlier in another article by Andresen et al. (13).
This was an anonymous nationwide questionnaire study. Entry criteria were: age 18 years or over, acquired traumatic SCI and contact with one of the two SCI rehabilitation centres in Denmark (Spinal Cord Injury Centre of Western Denmark in Viborg or Clinic for Spinal Cord Injuries in Hornbaek) from 1990 to 2012.The questionnaire was sent by post in January–April 2015. Participants had the option to complete either a web-based questionnaire (via survey-xact.dk) or a paper-based questionnaire. Cannabis consumption is illegal in Denmark, therefore all replies were anonymous and no reminders were sent out to non-responders.
Questionnaire data included demographic variables (age, sex, marital status, education level, region of residence and population density), labour force information (occupation, labour market affiliation, income) and lifestyle behaviours and habits (alcohol consumption, tobacco-smoking) (14). Information about the participants’ spinal cord injuries included cause, year of injury, whether the participant was tetraplegic (arms, body and legs affected) or paraplegic (body and legs affected), had a complete (no sensation or voluntary muscular function below injury level) or incomplete (some sensation and muscular function below the injury level) injury (15) and to what level daily life was limited due to the SCI (“not at all”, “little”, “moderate” and “much”).
Participants were asked if they had experienced continuous or daily recurring pain for more than 3 months. If participants answered “yes” they were considered to have chronic pain and they were asked to complete the International SCI Pain Basic Data Set (16), which includes rating mean pain intensity over the past 7 days on a 0–10 numeric rating scale (NRS). Pain treatment was recorded. Participants were also asked if they had experienced spasticity (muscle stiffness or spasms). Intensity of muscle stiffness was rated on an NRS (0–10) and the Penn Spasm Frequency Scale (17) was completed. Spasticity treatment was determined using a list of treatment options. Quality of life was assessed using the International SCI Quality of Life Basic Data Set (18), whereby participants estimated how satisfied they had been with their life situation and physical and mental health in the past week using an NRS (0–10). Participants also rated sleep disturbances during the past week on an NRS (0–10).
Participants were asked if they had tried cannabis at any time in their lives. If not, they were asked if they would try it if it were legal and for what reason. Those who had tried or used cannabis one or more times were asked about their age of debut. They were also asked if they had tried it before and/or after their SCI, how many times they had tried or used it, in what form and the reason for using cannabis. Participants who had used cannabis within the last 2 years were defined as “current” cannabis users and were given further questions about frequency, quantity, cause and effect of their cannabis consumption, as well as the extent of negative consequences (9).
Data were described as mean (SD) or median (range) or frequency and percentages. Normality was checked using histograms and quantile-quantile (Q-Q) plots. Numerical data were analysed using unpaired t-test or Mann-Whitney U test. Categorical variables were analysed using χ2 test or Fisher’s exact test. Variables in the univariate analyses with associations with current cannabis that had a p-value < 0.05 were included in a logistic regression model. A p-value < 0.05 was considered statistically significant. The level of missing data for different variables was less than 2.4%, and this was shown in the results tables. Missing data were not replaced. Statistical analysis was performed using STATA release 12 (StataCorp, College Station, TX, USA).
The authors certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research. The study was approved by the Danish Data Protection Agency, Copenhagen, Denmark (no. 1-16-02-210-14) and Danish Health and Medicines Authority, Copenhagen, Denmark (no. 3-3013-621/1).
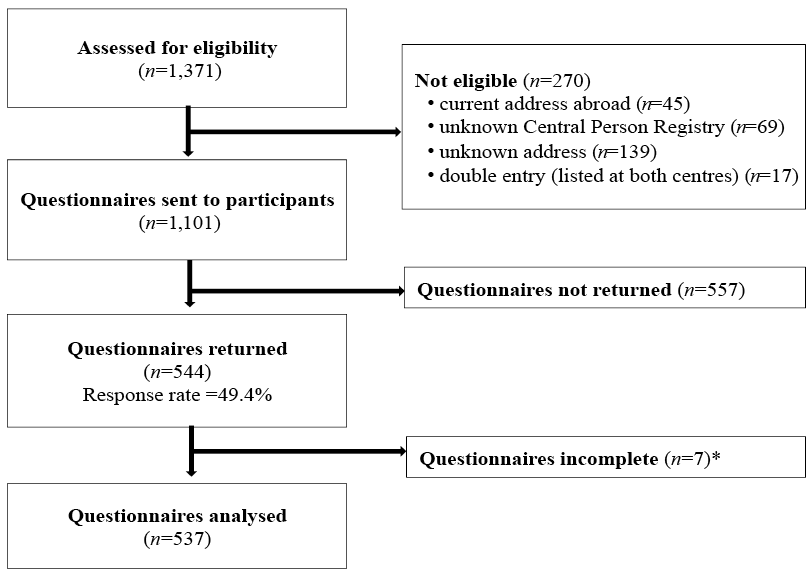
In the period 1990–2012, 1,371 individuals aged 18 years or over with an acquired traumatic SCI had been in contact with at least one of the two rehabilitation centres in Denmark. A total of 1,101 individuals were sent the questionnaire (Fig. 1). The response rate was 49.4% (544 individuals), of whom 196 responded via the web-based and 348 via the paper-based questionnaire. Of the returned questionnaires, 7 were incomplete with no information on cannabis use, and were therefore excluded. Consequently, questionnaires from 537 individuals were included and analysed (Fig. 1).
Fig. 1. Study flow chart. *No information on cannabis use.
Demographic variables and clinical characteristics of study subjects are shown in Table I. Mean age was 54.6 years (SD 14.6), age range 18–88 years; 77% were men, and the majority did not live with any children, but were either married or in cohabiting relationship (41%) or alone (35%). The majority lived in small- to-medium-sized cities, and 41% stated that they had at least a short post-secondary education. The majority of participants were non-smokers and their alcohol consumption was within the guidelines set by the Danish Health and Medicines Authority (14 units/week for men and 7 units/week for women). The mean time since injury was 18.2 (SD 12.8) years; 46% of responders were tetraplegic, and 68% had an incomplete injury. The most common causes of injury were transportation (41%) and falls (30%) (Table I). A total of 412 participants (77%) reported that their SCI had at least a moderate impact on their everyday life (Table I). A total of 390 (73%) participants reported chronic pain, in whom the mean intensity (NRS, 0–10) was 5.6 (SD 2.3) and 259 (67%) received treatment for pain. Spasticity was reported by 378 (71%) and 46% of these received treatment for spasticity (Table I).
Thirty-six percent (195 of 537) of all participants had tried cannabis at least once. Of these, 75% (147 of 195) were former cannabis users and 25% (48 of 195) current cannabis users (Table I). To be able to compare our data with available data on the general Danish population the group was subdivided by age. Of the 140 participants under the age of 45 years, 75 (53.6%) had tried cannabis at least once, in contrast to 120 (30.2%) of the 397 participants who were 45 years or older. The mean age for trying cannabis for the first time was 20.4 (SD 9.1), range 8–72 years. Comparing current with former cannabis users, there was no difference (p = 0.76). Of the 195 participants who had tried cannabis, 52% had used it before, 20% after, and 28% both before and after their SCI. In the latter group, 53% reported that their consumption had decreased, 15% that it had increased, and 32% that it was unchanged after their SCI. Of the 48 current cannabis users, 10 (21%) had tried cannabis after their SCI only.
Among participants who had tried cannabis (n=195), 174 (89%) stated that they had tried it for pleasure, 42 (22%) for medicinal use in relation to their SCI (such as pain and spasticity), 8 (4%) for other medical reasons (depression, anxiety, stress, anorexia), and 17 (9%) gave other reasons (sleep, sex, partying and curiosity). Among the 147 former cannabis users, 38 (26%) had tried it more than 20 times, 17 (18%) 11–20 times, and 90 (62%) 10 times or less. Former cannabis users most often used hashish, whereas current users also consume a variety of other forms of cannabis, which may contain more THC, such as skunk (Fig. 2). Medical cannabis (sativex or dronabinol) was not commonly used (4 current and 3 former cannabis users). Of the 342 participants who had never tried cannabis, 69 (20%) responded that they would try it if it were legal and they reported pain, spasticity and sleep disturbance as the most common reasons (Fig. 3a).
Fig. 2. Type of cannabis used by current (have used cannabis within the past 2 years, n = 48) and former (have not used cannabis within the past 2 years, n = 147) cannabis users *p <0.05; **p <0.01.
Fig. 3. (A) Reasons why participants who had never tried cannabis would try it if cannabis were legal (n = 69). (B) Reasons for cannabis use as well as experienced effect among current cannabis users (n = 48). *Other reasons included: (a) headache, sex problems, constipation, as treatment, and “would like to try”; (b) headache, sex problems, constipation, habit, relaxing, enjoyable, and boredom.
Further details were obtained for the 48 current cannabis users, i.e. the participants who had used cannabis within the past 2 years. Thirty-one (65%) were under 45 years old. Twenty-two percent of the participants under 45 years of age and 4% of participants 45 years of age or older were current cannabis users. The mean age of current users under 45 years of age was 34.9 (SD 7.2) years. Among the 48 current users, 14 (29%) reported daily use, 12 (25%) used at least once per week, 7 (15%) at least once per month, 10 (21%) at least once per year, and 5 (10%) less than once per year. Thirty-eight (79%) participants had tried cannabis more than 20 times, 3 (6%) between 11 and 20 times and 7 (15%) l0 times or less. Among current cannabis users, 39 (81%) stated they had tried it for pleasure, 31 (65%) for medicinal use in relation to their SCI, 7 (15%) for other medical reasons, and 7 (15%) gave other reasons. Ten percent (5/48) of current cannabis users reported their use of cannabis for no other reason than for the secondary complications due to their SCI. Of the 31 participants who also used it for medical reasons in relation to their SCI, 8 had started using cannabis after their SCI. Among the 26 participants who knew their level of consumption of cannabis, the mean intake in the previous 4 weeks was 13.8 (SD 25.1) g and the mean costs during the same period was 514.4 (SD 868.9) DKK (approximately 69 (SD 116.5) Euro). The most frequently reported reasons for using cannabis were pleasure, followed by pain, partying and spasticity (Fig. 3b). Most participants reported a good to very good effect (Fig. 3b). For pain (29/48), 10 (35%) had a good and 7 (24%) a very good effect, and for spasticity (22/48), 7 (32%) had a good and 6 (27%) a very good effect. The 4 individuals who used medical cannabis (dronabinol and sativex) reported none or some effect on pain and spasticity. Of current cannabis users 8.3 % (4 of 48) used medical cannabis. Current cannabis users took paracetamol less often than participants who were not current cannabis users (p = 0.030), while there was no significant difference between current and not-current cannabis users in terms of other treatments for pain or spasticity (p > 0.05).
Negative consequences of cannabis use included inertia, feeling quiet/subdued, absentmindedness and risky behaviour, which were most often rated as slightly to moderately serious (Fig. 4).
Fig. 4. Negative consequences of cannabis use and the seriousness of these consequences reported by current cannabis users (n = 48). *Other consequences included loss of mobility, fines and insecure transfer (e.g. from wheelchair to bed).
Significant variables identified through the univariate analyses in Table I were examined further using a logistic regression model. The overall model was significant (p < 0.001) with an overall classification accuracy of 93%. Lower age, a city population of 5,000–19,999 and > 100,000, tobacco-smoking, alcohol consumption exceeding recommended units per week, and higher muscle stiffness scores were significantly associated with cannabis use (Table II).
Table II. Demographic and clinical characteristics associated with cannabis use. Variables in logistic regression model
This nationwide questionnaire study of 537 individuals with SCI found that 36% had tried cannabis at least once. Forty-eight participants (9%) had used cannabis within the past 2 years and were considered current users, which is lower than found in 2 previous studies in other disease populations. Harris et al. (9), a cross-sectional survey in Canada of 256 patients, found that 38.5% of participants with HIV/AIDS were current cannabis users, which was a 3.5-fold higher prevalence than in the general Canadian population. In a multiple sclerosis study in the UK (7), 18% of 254 responders were current cannabis users. Medical use of Cannabis is legal in Canada, but not in the UK or Denmark, which may influence the number of individuals using cannabis.
The Danish Health and Medicines Authority provides national data for the use of cannabis in individuals under 45 years of age (n = 5,748 in the year 2010)(19). In our study, 54% (75/140) of participants under 45 years of age had tried cannabis at least once, and 22% (31/140) had used cannabis within the past 2 years compared with the general Danish population, of whom 41.5% of individuals under the age of 45 years had tried cannabis at least once and 8.9% had used cannabis within the past year, and 78% of current users were between 16 and 24 years of age (19). Comparing our study population (n = 140) with the Danish general population (n = 5,748) under the age of 45 years, suggests that our population used cannabis more often than the Danish general population. A possible reason for the higher use among individuals with SCI may be that cannabis use increases risky behaviour and users therefore have a greater risk of accidents and thus SCI. This may be supported by the fact that 38 of the 48 current cannabis users started their cannabis use before their SCI. Increased incidences of accidents were seen in the USA when cannabis was legalized and became more accessible to a larger population (20). Another possible explanation is that persons using cannabis are risk prone, i.e. are more likely to drink alcohol, use cannabis and engage in activities with a risk of accidents (21). It is also possible that living with SCI and the consequent secondary complications may lead to increased cannabis use, since 31 of the 48 current users reported that they used cannabis partly for relief of secondary complications due to their SCI, although only 8 of these had started using cannabis after their injury.
In our study, pleasure, followed closely by pain, partying and spasticity, were the most frequent reasons for cannabis use. Thirty-one (65%) of current cannabis users, corresponding to 5.8% of the whole sample, reported that they used cannabis partly to relieve SCI-related symptoms, while 81% reported that they had tried it for pleasure. Ten percent used it exclusively for SCI-related symptoms. In comparison, for individuals with HIV/AIDS, 22% of cannabis users and 8.4% of a total study population of 226 reported medicinal cannabis use (9). However, 81% of all cannabis users reported medically related symptoms as reasons for use in addition to recreational use, which was reported by 98%, Only 2.3% of current users reported medicinal use only (9). Thus, in both populations there is considerable overlap between medical and recreational cannabis use. In studies of multiple sclerosis, 18% (46/254) of the total population reported current use of cannabis (7), and 12% (31/254) and 10% (43/420) reported using cannabis to relieve disease-associated symptoms (7, 10). The slightly higher percentage of current users among individuals with multiple sclerosis may partly be because this population is more aware of cannabis being potentially useful to alleviate their symptoms (10).
Among those who had never tried cannabis, 20% reported that they would try cannabis if it was legal, and the majority of these would use cannabis for their pain, spasticity and sleep disturbance. A previous study of multiple sclerosis (n = 254) in UK found that over 70% of individuals who had never used cannabis would try it if it were available on prescription (7). The same reasons were also commonly reported by current users, although in this group, pleasure and partying were other common reasons. Most current users reported at least some effect on pain, spasticity and sleep disturbance. Less effect was reported by the 4 participants who used medical cannabis. The effect of marijuana on pain and spasticity following SCI was suggested already in 1974 (22), and in a more recent questionnaire study from the US, marijuana was reported as an alternative pain treatment by 32% and, of all treatments, was rated as the one that gave the greatest pain relief (5). Other studies have reported the use of cannabis in pain and spasticity (6, 23). Cannabinoid medications have been developed and are now used in the treatment of pain and spasticity. These include dronabinol and nabilone, which are synthetic THCs, nabiximols (sativex), which is an oromucosally delivered spray containing extracts of the cannabis plant. Two trials failed to find effect of dronabinol or sativex for SCI neuropathic pain (24) (Clinicaltrials.gov, NCT01606202). Except for the use of smoked or inhaled cannabis, which in a few short-term trials has shown efficacy on different neuropathic pain conditions, not including SCI neuropathic pain (25, 26), randomized controlled trials have shown conflicting results for neuropathic pain (27). Recent recommendations from the Neuropathic Pain Special Interest Group of the International Association for the Study of Pain (27) include a weak recommendation against the use of cannabinoids for neuropathic pain, due to negative results, side-effects, issues of misuse and abuse and possible long-term risks of psychosis and cognitive impairment, in particular in susceptible individuals (28, 29), although this is still debated (30). Few studies have examined the effect of medical cannabis on SCI-related spasticity. In a single case trial, there was an effect of delta-9-THC (31), whereas an unpublished trial showed no effect of sativex on SCI-related spasticity (Clinicaltrials.gov, NCT01606202). Also, for spasticity due to multiple sclerosis, the results are conflicting (32). In Denmark, dronabinol and sativex are available for medical use, but with specific requirements for reimbursement, and it is illegal to drive while using medical cannabinoids, which may explain the low number of individuals with SCI using medical cannabis in this study.
The mean age of debut for cannabis use in our population was 20 years, which is consistent with a debut in the Danish general population of 16–24 years (33), but lower than the 23.3 years reported in the study in an HIV/AIDS population from Canada (9).
Participants in the current study reported a mean consumption of cannabis of 13.8 g (SD 25.1 g) per 4 weeks, but the amount of cannabis ranged from 0 to 100 g per 4 weeks. Participants spent between 0 and 3,000 DKK per 4 weeks, with a mean amount of 514.4 DKK (SD 868.9) per 4 weeks. A recent study looking at the correlation between cannabis use and HIV/AIDS showed almost the same consumption of cannabis (18.3 g) and cost (USD 105.15) per month (9), while an earlier study of HIV showed a considerably higher consumption of cannabis, up to a mean of 66 g and USD 243 per month on average (34).
Current cannabis users took paracetamol less often than participants who were not current cannabis users. This is of interest since paracetamol has been shown to inhibit cellular synaptic space reuptake of anandamide and thus have cannabinoid-like analgesic effects (35, 36). A synergistic interaction effect between cannabinoids and paracetamol has also been suggested (37), which is of interest for future studies.
Inertia, feeling quiet/subdued, absentmindedness and risky behaviour were described by participants as negative consequences and were reported as slightly to moderately serious. Since this was a cross-sectional survey, we were not able to examine the long-term effect. Several studies have shown that there may be an increased risk of developing both psychotic and cognitive dysfunction (4, 25, 38, 39), and both short- and long-term effects and the potential for abuse and addiction (39) should be considered if cannabis were to be offered as treatment for pain or spasticity.
Factors associated with cannabis use in our SCI population were lower age, the number of residents in the city where the participants lived (both smaller and larger cities), tobacco-smoking (both daily and periodically), higher alcohol consumption and higher muscle stiffness score (NRS =7–10). This is in agreement with previous studies (7, 9, 11, 12). Pain and severity of the SCI were not found to predict current cannabis use.
This was a cross-sectional study; therefore it was only possible to examine the causal relation between cannabis use and the consequences of a SCI. The response rate of 49% is relatively low, which could induce the risk of type 1 error. The low response rate may have been due to cannabis use being illegal in Denmark, and to the fact that it was not possible to send out reminders as the response was anonymous.
We were not authorized to access information held in the medical records by the Danish Health and Medicines Authority, therefore it is not known whether our sample population is representative of the whole group who received the questionnaire. However, epidemiological studies suggest that our sample is representative of the population with traumatic SCI in Denmark. A recent Danish epidemiological study for the period 1990–2012 found the median age at injury to be 35 years, with a predominance of men (81.9%) (40). By comparison, our study showed a prevalence of 77% (413/537) was found in men, with a median age at injury of 33 years. Previous studies (Bjørnshave et al. 2015 (n = 691) and Lee et al. 2014 (9.2 per million in Denmark)) have shown that transportation (47%) and falls (26%) are the main causes of SCI in Denmark (40, 41), which is similar to the results of our study. The distribution of tetraplegia (51%) and paraplegia (49%) among individuals with SCI in Denmark (41) is also consistent with our results.
The current study found the prevalence of current cannabis users among persons with traumatic SCI in Denmark to be slightly higher than previously reported in the Danish general population. This may be due to an increased risk of accidents among cannabis users. Most participants started using cannabis before their SCI and used it for recreational purposes, but some also reported some effect on pain and spasticity. Approximately 20% of those who had never tried cannabis stated that, if cannabis use were legal, they would try it in order to alleviate symptoms due to SCI. Cannabis use was associated with lower age, living in rural areas and larger cities, tobacco-smoking, high alcohol intake and higher muscle stiffness. There is currently limited evidence for the use of medical cannabis for SCI-related pain and spasticity, and there are concerns about side-effects and long-term risks. Further research into cannabinoid treatments and the development of cannabinoid drugs with fewer psychological side-effects, such as CB2 receptors agonists, palmitoylethanolamide analogues and endocannabinoid-degrading-enzyme inhibitors, is needed.
This study was supported by the Health Research Fund of Central Denmark Region and the Danish Society of Polio and Accident Victims (PTU). All authors had full access to all data and the corresponding author had final responsibility for the decision to submit for publication.
Conflicts of interest. The authors have no conflicts of interest to declare within the submitted work. NBF has received honoraria from Pfizer and Grünenthal and grants from IMI Europain (EU/EFPIA) outside the submitted work. FWB has received investigator fees from Pfizer and Grünenthal.


 Click to show fullsize
Click to show fullsize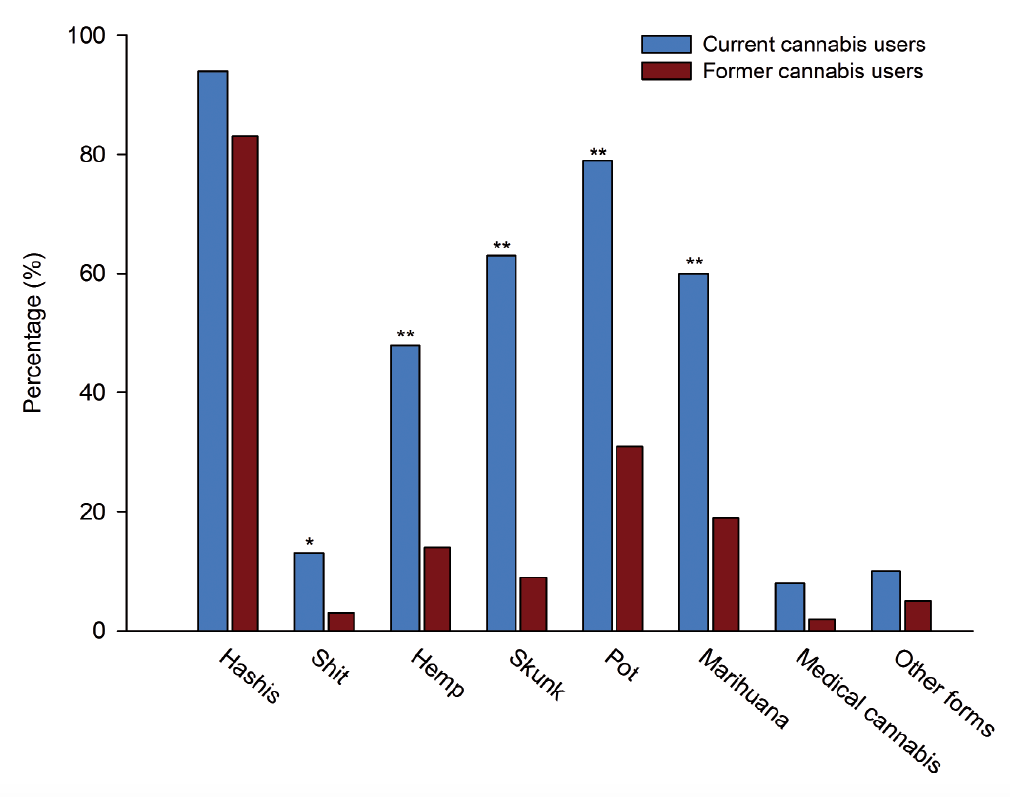 Click to show fullsize
Click to show fullsize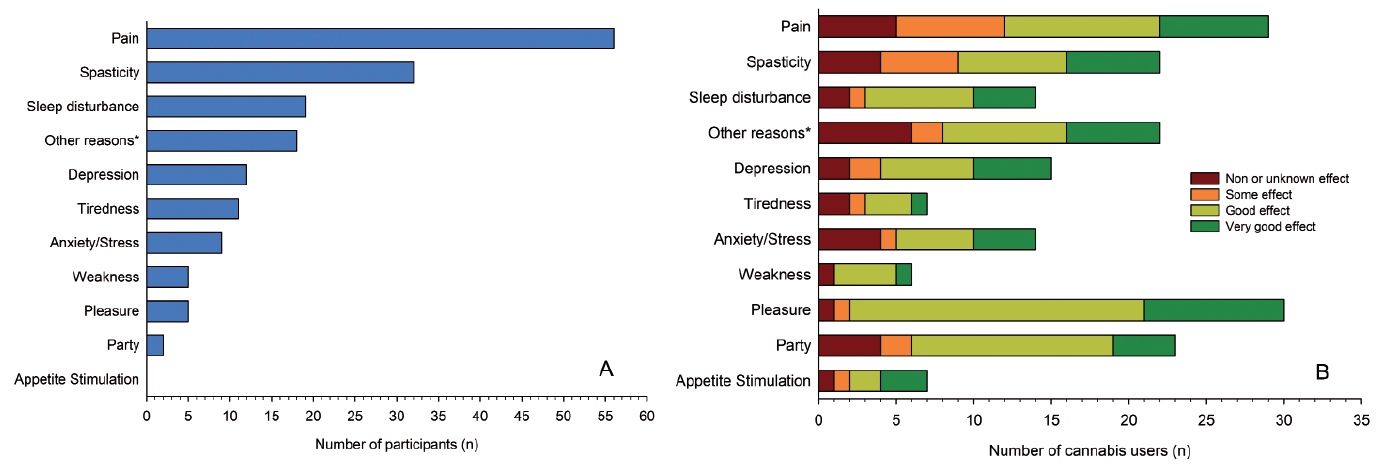 Click to show fullsize
Click to show fullsize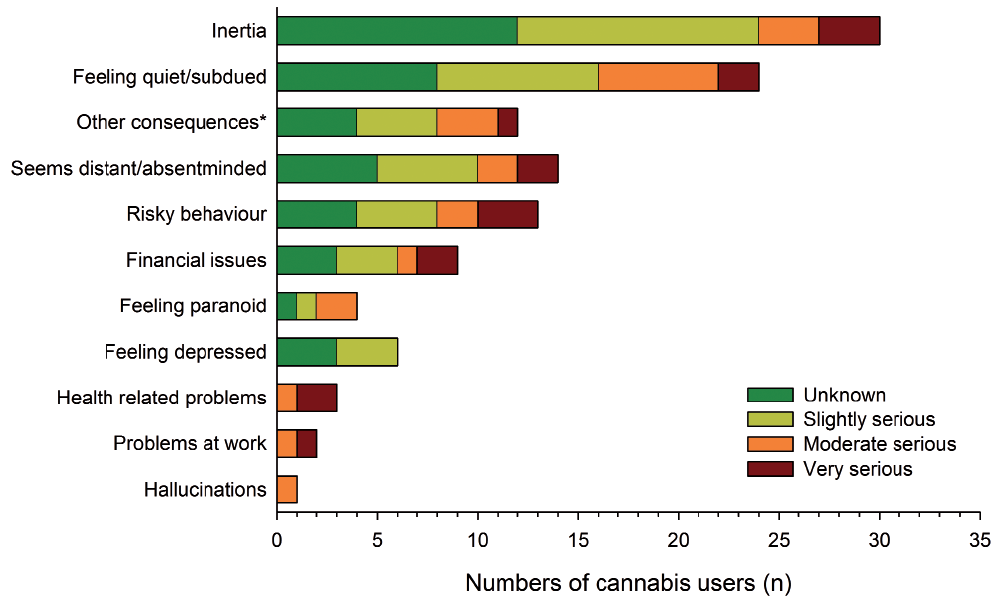 Click to show fullsize
Click to show fullsize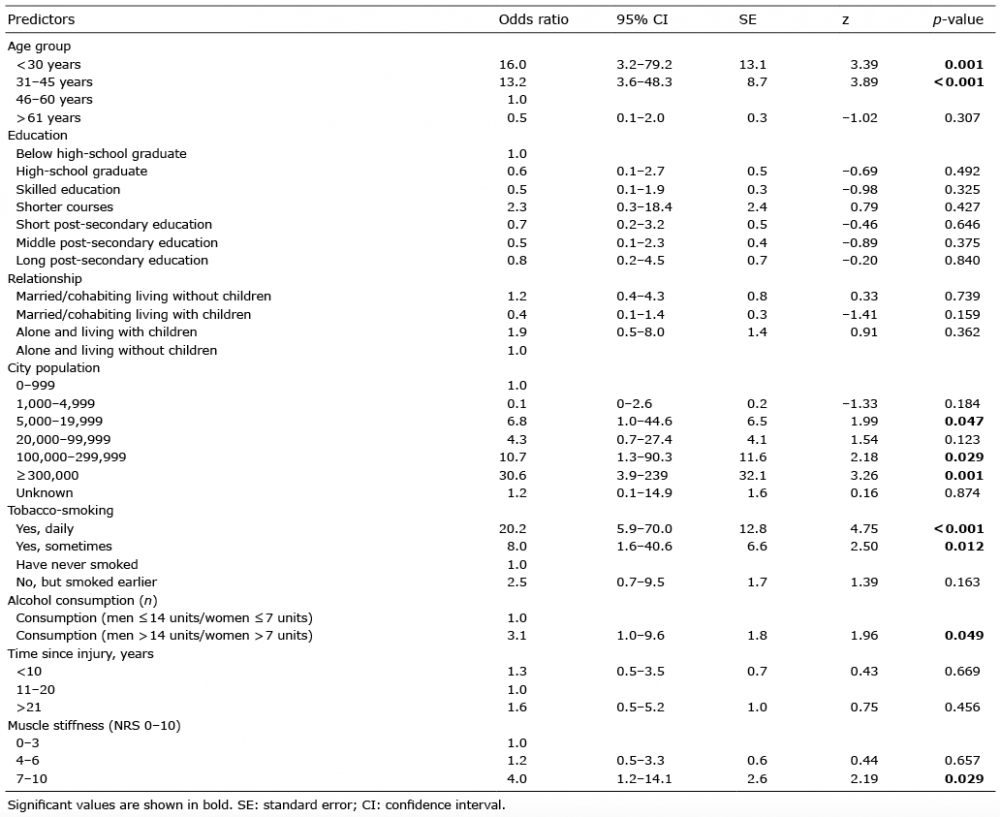 Click to show fullsize
Click to show fullsize