Anupam Datta Gupta, FAFRM1 and David Wilson, PhD2
From the 1Rehabilitation Medicine and 2Division of Medicine, University of Adelaide, Queen Elizabeth Hospital, Woodville South, Australia
OBJECTIVE: To review the diagnosis of patients transferred to rehabilitation unit.
DESIGN: Case series.
SUBJECTS: Five patients with functional decline were transferred from an acute care setting in a tertiary hospital to the rehabilitation unit.
METHODS: Full clinical evaluation and clinical reasoning were applied in addition to multidisciplinary care. Functional outcome and discharge destination were noted in each case.
RESULTS: All patients had a new diagnosis that evolved during their stay in the rehabilitation unit in addition to their existing conditions. The new diagnosis helped to direct their future treatment programme. Four patients had good outcomes; they gained significant functional independence and were discharged home. One patient had an adverse outcome.
CONCLUSION: In addition to multidisciplinary care, it is important to review the medical diagnosis in the rehabilitation unit. Diagnostic errors can have profound effect on the lives of patients with already existing impairments. Rehabilitation physicians should avoid making assumptions or diagnostic biases, and reapply clinical reasoning especially in the care of individuals with functional decline in rehabilitation.
Key words: diagnostic error; biases; disability; rehabilitation.
J Rehabil Med 2016; 48: 00–00
Correspondence address: Anupam Datta Gupta, Department of Rehabilitation Medicine, Queen Elizabeth Hospital, 28 Woodville Road, Woodville South, South Australia-5011. E-mail: adattagupta86@gmail.com
Accepted Feb 10, 2016; Epub ahead of print Mar 22, 2016.
INTRODUCTION
Medical diagnostic error (failure or delay in diagnosis and wrong diagnosis) is estimated to be as high as 10–15% (1). Most research on diagnostic error has been performed in acute and primary care, with very little research in rehabilitation. Many patients with functional impairments are referred to the rehabilitation unit, and the prevalence of disability is increasing. The change of focus in rehabilitation is on therapy and restoration of function. By the time a patient is seen in rehabilitation, there exists the dangerous and implicit assumption that the diagnosis has already been correctly and comprehensively made. According to Wade rehabilitation diagnosis is perceived to be simple and unimportant (2).
The current study examined this situation in a convenient sample of 5 rehabilitation patients. New findings were identified during their stay as inpatients, potentially confounding the rehabilitation process. No assumptions were made about the diagnosis, and clinical and diagnostic reasoning were applied anew. Although the prima facie evidence suggested that the diagnoses of these patients made in the acute setting were correct, new findings during their stay in rehabilitation led to new diagnoses. If this had not occurred, the new pathology had the potential to profoundly affect patient safety, wellbeing, functioning and quality of life. We describe the case series and discuss the possible diagnostic assumptions and biases and how one might prevent them together with possible implications for rehabilitative medicine.
METHODS
Our study was approved by the hospital committee as a quality improvement activity. All patients provided their consent.
The patients were transferred from acute care units of a tertiary hospital to the rehabilitation hospital between 2011 to 2013.
CASE REPORTS
Case 1
A 66-year-old woman, who had post-polio paralysis of her right arm, and used to manage her own tailoring business, presented with right arm pain, neck pain and occasional headaches. She reported difficulty in carrying out activities of daily living and had had to stop driving. Initially a diagnosis of post-polio syndrome was made. Her symptoms persisted and later she developed mild hyperreflexia of the lower limbs. Cervical spinal X-rays showed mild subluxation around the atlantoaxial joint. A magnetic resonance imaging (MRI) revealed herniation of the brain through the foramen magnum and the patient was referred to neurosurgery.
Case 2
A 32-year-old women with cerebral palsy and torticollis was admitted with significant decline in mobility over a period of 1 month. She was living with her mother and was independent in her functions and mobility (both indoors and outdoors). Initially the decline was thought to be a natural progression of her underlying condition. An initial computed tomography (CT) scan of her brain revealed nothing of consequence. The patient had a history of good pre-morbid functioning until that period. In view of her recent functional decline, we decided to investigate with an MRI under neuroleptics, which revealed cervical cord changes secondary to C4/C5 cervical disc prolapse. The patient was referred to neurosurgery.
Case 3
A 76-year-old man with ankylosing spondylitis (AS) collapsed and fell at home and was brought to the emergency department. He was diagnosed with a ruptured abdominal aortic aneurysm. Following surgery, he was referred to our rehabilitation unit. He also reported having back pain (dorsal) since the fall, which was not associated with neurological signs. Thoracic X-rays conducted during rehabilitation revealed a 3-column fracture of T6. The patient was referred urgently to the orthopaedic unit.
Case 4
A 78-year-old woman, living with her husband, was admitted to the hospital with L1 fracture following a fall. Prior to this, she had been an active individual who used to care for her husband who was unwell. Following conservative management, she was transferred to the rehabilitation unit. During her stay in rehabilitation, she developed weakness in her legs and subsequently developed urinary incontinence. Due to lack of improvements in rehabilitation, it was thought she would need to go into residential care. Clinical examination revealed reduced tone in her lower limb muscles and depressed deep tendon reflexes combined with an extensor plantar response. An MRI was requested and demonstrated that bony fragments from the vertebral fracture were compressing the spinal cord at the L1 level. This explained the unexpected clinical findings.
Case 5
An 81-year-old man, who was previously independent, was transferred to the rehabilitation unit from an acute hospital with right middle cerebral artery ischaemic stroke. His impairments were dysarthria, left facial droop, left hemiplegia, left homonymous hemianopia and poor balance. The patient deteriorated during his stay in the rehabilitation unit, characterized by slurred speech and worsening balance. He was transferred to the neurology unit and underwent further investigation.
RESULTS
Case 1
The patient had a 6-mm descent of her brain through the foramen magnum (Fig. 1) and was diagnosed with Arnold Chiari malformation (type 2). After foramen magnum decompression, she attended 2 weeks of rehabilitation and underwent significant improvement of her symptoms with an overall improvement in her quality of life. Furthermore, she was able to drive her car again and re-start her business.
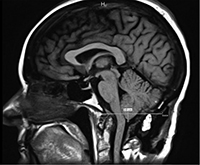
Fig. 1. Cerebellar tonsillar herniation through the foramen magnum; Arnold Chiari malformation.
Case 2
The patient had cervical myelomalacia due to cervical spondylotic myelopathy secondary to C3/C4 disc prolapse (Fig. 2). She was treated with botulinum toxin for torticollis and underwent a successful cervical laminectomy followed by transfer to the rehabilitation ward. She achieved independence in activities of daily living and mobility. She returned home to live with her mother and was able to re-gain her driving license.
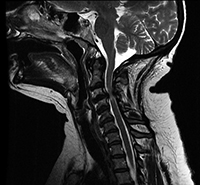
Fig. 2. Cervical myelopathy secondary to C3/C4 cervical disc prolapse.
Case 3
The patient was diagnosed with a Chance fracture and underwent surgical stabilization (Fig. 3) of the thoracic spine. Patients with ankylosing spondylitis (AS) develop osteoporosis and are particularly at risk of unstable fracture from falls. This patient was transferred back to the rehabilitation unit. His pain improved and he was discharged home after gaining full functional independence.

Case 4
With cord changes at L1 level and a combination of upper and lower motor neurone signs, the patient was diagnosed with conus medullaris syndrome. She underwent spinal decompression and internal fixation with pedicular screws (Fig. 4) and was transferred back to the rehabilitation unit. After a period of therapy, she was able to walk with the aid of a walking frame and returned home.
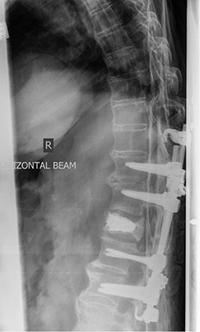
Fig. 4. Spinal decompression and pedicular screw fixation for compression fracture in L1.
Case 5
The new MRI revealed significant interval progression and involvement of the corpus callosum, superior brain stem and right cerebellum with cortical sparing (Fig. 5). Spectroscopy findings were compatible with infiltrative neoplastic process and gliomatosis cerebri was diagnosed. The patient died after 1 week of steady deterioration.
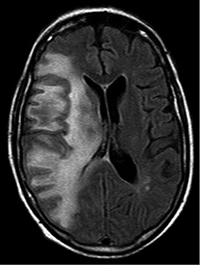
Fig. 5. Gliomatosis cerebri infiltrating the right half of the brain.
DISCUSSION
The diagnosis of these patients did not come with them, rather evolved during their stay in rehabilitation (Table I). The medical profession has been criticized in its treatment of people with disabilities and over medicalizing disability, ignoring the social factors (3). Such a view may influence physicians to put less emphasis on reviewing the diagnosis in rehabilitation. The International Classification of Functioning, Disability and Health (ICF) emphasizes correct diagnosis of the impairments, which may otherwise cause activity limitation and participation restriction (4). A patient with functional impairment needs to be reviewed using critical thinking and full diagnostic clinical reasoning that exhaust and exclude all reasonable possibilities.
|
Table I. Patients’ demographics, presenting diagnoses, and new diagnoses made in rehabilitation |
||||
|
Patient |
Age, years |
Sex |
Presenting diagnosis |
New diagnosis |
|
1 |
63 |
F |
Post-polio paralysis |
Arnold Chiari malformation |
|
2 |
40 |
F |
Cerebral palsy |
Cervical myelopathy |
|
3 |
71 |
M |
AAA repair and ankylosing spondylitis |
Chance fracture |
|
4 |
65 |
F |
Compression fracture L1 |
Conus medullaris syndrome |
|
5 |
75 |
M |
MCA stroke |
Gliomatosis cerebri |
|
AAA: abdominal aortic aneurysm; MCA: middle cerebral artery. |
||||
Clinical reasoning in rehabilitation patients
Patients with a lack of functional improvement or with new symptoms in the rehabilitation setting should constitute a “red flag” category and need a full diagnostic review. This involves application of the medical model of disabillity in diagnosis. Clinical diagnostic decision-making generates a number of hypotheses on the basis of the clinical presentation and tests them against each other (5). Clinical reasoning is associated with the use of general strategies or heuristics, pattern recognition, patient prototype and the use of semantic qualifiers (opposing descriptors, such as acute vs. chronic, or proximal vs. distal, which are used to compare and contrast the diagnostic possibilities). Clinicians store and recall diseases, conditions or syndromes as “illness scripts” or mini patterns (5). The same medical skills can be the stock in trade for physiatrists and may require collaborative medical care from various specialties (medicine, neurology, surgery, etc.) in addition to multidisciplinary care in rehabilitation.
Diagnostic errors
Physiatrists ought to be aware of potential diagnostic errors, which involve cognitive and system factors. Investigation of how to reduce system factors is beyond the scope of this review, but it is important to remember diagnostic decision-making biases. Such biases (6) include: (i) anchoring, i.e., failure to acknowledge alternative diagnoses and seek appropriate confirmation (e.g. case 1 and case 3); (ii) confirmation bias; a tendency to rely on the evidence that fit with the existing belief or hypothesis and simultaneously ignore the alternative hypotheses (“cognitive cherry-picking”) (e.g. case 2) (7); (iii) convergence; quick focus on a singular diagnosis excluding the alternatives (e.g. case 4); (iv) representativeness; decisions made on the basis of one piece of information undervaluing the base rate; (v) overconfidence (e.g. case 5); (vi) availability bias; when an easily remembered condition comes to mind (e.g. case 1); (vii) hindsight bias; overestimating the probability of a diagnosis when the diagnosis is already known; (viii) sunk cost bias; previous investment (time, effort and training) can have an irrational influence.
Physicians need to be more careful about persons with disability because of our natural tendency to think of functional impairment always as a consequence of the underlying obvious condition (for example, cerebral palsy or stroke) rather than considering new pathology. The example just alluded to could be a thinking error (bias) rather than negligence.
Suggestions
There is evidence that an awareness of bias reduces the likelihood of making it (8). An effective hand-over is important when patients are transferred (7). Using checklists can be useful (9). Consideration of alternatives, reflection on the thinking process (metacognition) (9) and “Partnering with the patient” may lessen the risk of error (10). An awareness of evidence-based medicine can be helpful in reducing bias, because it provides explicit and judicious use of the best evidence in making decisions about patient care (11). Registering diagnostic faults can be very useful for improvement of diagnostic and therapeutic process and should be viewed as a measure of quality improvement.
The 5 patients described here do not comprise a representative sample of patients admitted to rehabilitation following a primary diagnosis. The field of diagnostic error is fairly new, with most of the work done in emergency medicine, internal medicine and family medicine (12). There is no published quantifiable study on general rehabilitation. A prospective study of the prevalence of diagnostic errors (delayed, missed or wrong diagnosis) in patients with functional loss or disability in the rehabilitation unit is in progress in our hospital.
To summarize, impairment, activity limitation and participation restriction are not mutually exclusive constructs; they influence each other. Persons admitted in the rehabilitation units may still have unsolved and/or undiagnosed and/or newer medical issues contributing to their disability. Physiatrists should not be anchored to the mistaken assumption that all problems are related to the existing diagnosis. The best possible outcome of care can be ensured when the medical model of disability in diagnosis supplements the multidisciplinary and social models. The cases mentioned in the paper highlight the fact that reassessment with an open mind to rethink newer diagnostic possibilities is more likely to be beneficial in many individual patients.
ACKNOWLEDGEMENTS
The study was conducted in the Queen Elizabeth Hospital, 28 Woodville Road, South Australia-5011.
Part of this paper was presented as a poster at the International Society of Physical and Rehabilitation Medicine (ISPRM) scientific meeting, Berlin, 19–23 June 2015.
The authors did not receive any financial support for this study.
The authors declare no conflicts of interest.
REFERENCES

