Birgit Prodinger, PhD1,2,3, Jan Reinhardt, PhD1,2,4, Melissa Selb, MSc1,3, Gerold Stucki, MD, MS1,2,3, Tiebin Yan, MD5, Xia Zhang, MD, PhD6,7 and Jianan Li, MD5,6,7
From the 1Swiss Paraplegic Research, Nottwil, 2Department of Health Sciences and Health Policy, University of Lucerne, Lucerne, 3ICF Research Branch, a cooperation partner within the World Health Organization (WHO) Collaborating Centre for the Family of International Classifications in Germany (at Deutsches Institut für Medizinische Dokumentation und Information; DIMDI), Nottwil, Switzerland, 4Institute for Disaster Management and Reconstruction, Sichuan University and Hong Kong Polytechnic University, Chengdu, Sichuan, 5Department of Rehabilitation Medicine, Sun Yat-sen University, 6The First Affiliated Hospital of Nanjing Medical University, Nanjing and 7Chinese Association of Rehabilitation Medicine, Beijing, China
OBJECTIVE: A national, multi-phase, consensus process to develop simple, intuitive descriptions of International Classification of Functioning, Disability and Health (ICF) categories contained in the ICF Generic and Rehabilitation Sets, with the aim of enhancing the utility of the ICF in routine clinical practice, is presented in this study.
METHODS: A multi-stage, national, consensus process was conducted. The consensus process involved 3 expert groups and consisted of a preparatory phase, a consensus conference with consecutive working groups and 3 voting rounds (votes A, B and C), followed by an implementation phase. In the consensus conference, participants first voted on whether they agreed that an initially developed proposal for simple, intuitive descriptions of an ICF category was in fact simple and intuitive.
RESULTS: The consensus conference was held in August 2014 in mainland China. Twenty-one people with a background in physical medicine and rehabilitation participated in the consensus process. Four ICF categories achieved consensus in vote A, 16 in vote B, and 8 in vote C.
Discussion: This process can be seen as part of a larger effort towards the system-wide implementation of the ICF in routine clinical and rehabilitation practice to allow for the regular and comprehensive evaluation of health outcomes most relevant for the monitoring of quality of care.
Key words: International Classification of Functioning, Disability and Health; health information systems, practicing standards; quality management.
J Rehabil Med 2016; 48: 00–00
Correspondence address: Birgit Prodinger, ICF Unit, Swiss Paraplegic Research, Guido A. Zäch Institute, CH-6207 Nottwil, Switzerland. E-mail: birgit.prodinger@paraplegie.ch
Accepted Dec 2, 2015; Epub ahead of print Mar 22, 2016
INTRODUCTION
Quality of care is an essential factor in sustaining and improving current healthcare systems. Variations in quality of care have been described within and between healthcare systems. These variations may be concerned with accessibility to care, but also with the care provided to people with similar conditions. The challenge is how to identify the variations that result in best outcomes (1). It is only through the availability of data on relevant outcomes that quality can be monitored and continuously improved (2). The term “relevant” means that the data captures well the patients’ current and future needs (3). There are at least 3 aspects to be considered. First, outcomes must be specified clearly and framed within operational variables. Secondly, a universal language is needed for reporting relevant outcomes, which can be understood by all stakeholders. Thirdly, the agreed reporting of relevant outcomes must be applied consistently within and between systems to enable comparisons across parts of a specific system as well as between systems. Thus, a minimal set of domains of functioning is required, which capture the essence of what matters to individuals, and yet, are easy to understand and apply in a standardized manner by any stakeholder in the system.
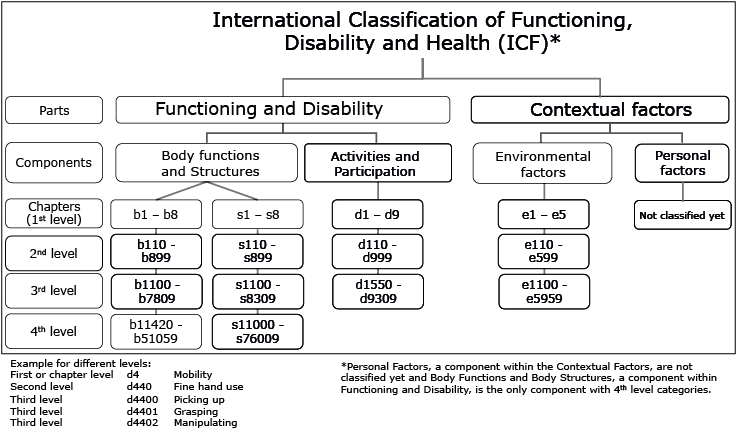
As the foundation for healthcare quality management, the understanding of health based on the components specified by the World Health Organization (WHO) in the International Classification of Functioning, Disability and Health (ICF; 4) has been set out as a requirement (5). These components are: body functions and structures, activities and participation, and their interaction with contextual factors. Within this framework functioning is the operationalization of health. The ICF not only builds upon the bio-psycho-social model of health and disability, but also provides an exhaustive and mutually exclusive set of categories, which are aligned with the conceptual model and serve as reference units for the standardized reporting of functioning. As such, the ICF offers operational variables for the continuous and consistent assessment of outcomes; it constitutes a universally agreed language to be used by diverse stakeholders in the health system and is thus well-suited for system-wide implementation (6).
Since the inception of the ICF in 2001, there has been a strong commitment to its implementation in routine practice. More recently, however, the question has been posed as of whether the ICF has become rhetoric on the macro level without having been fully translated into clinical and research practice, including data collection and reporting (7). The utility of the ICF as a practicing standard can be further enhanced by developing tools that are simple to use, do not increase administrative burden, and yet adhere to the standards (8, 9). As an important step in this process, ICF Core Sets have been developed based on an international, multi-phase consensus process. ICF Core Sets are practical tools to enhance the utility of the ICF for routine practice (10). They specify shortlists of ICF categories that are most relevant to be assessed and reported in the context of a particular health condition or setting (11). ICF Core Sets help to capture the variability of a specific health condition, and provide an established set of ICF categories to ensure comparability. More recently, an ICF Generic Set has been developed, which consists of 7 ICF categories that have been found to be most relevant across the general population as well as different clinical populations, contexts, settings and purposes (12). An extended version of this set, the ICF Rehabilitation Set, with 30 ICF categories, can be used in the context of rehabilitation and disability to describe varying levels of functioning across various clinical populations and along the continuum of care (13, 14). These ICF categories are listed in Table I. The ICF Generic and Rehabilitation Set can be applied as minimal standards for assessing functioning in clinical practice and population-based health surveys as well as for monitoring the impact of interventions at the clinical, service, and public health level. This makes the ICF Generic and Rehabilitation Set well suited to be consistently used for the standardized reporting of functioning as a relevant outcome in rehabilitation to enable comparisons within and between health systems.
|
Table I. Categories contained in the International Classification of Functioning, Disability and Health (ICF) Generic and Rehabilitation Set |
|
|
ICF Code |
Label |
|
b130 |
Energy and drive functions (G) |
|
b134 |
Sleep functions |
|
b152 |
Emotional functions (G) |
|
b280 |
Sensation of pain (G) |
|
b455 |
Exercise tolerance functions |
|
b620 |
Urination functions |
|
b640 |
Sexual functions |
|
b710 |
Mobility of joint functions |
|
b730 |
Muscle power functions |
|
d230 |
Carrying out daily routine (G) |
|
d240 |
Handling stress and other psychological demands |
|
d410 |
Changing basic body position |
|
d415 |
Maintaining a body position |
|
d420 |
Transferring oneself |
|
d450 |
Walking (G) |
|
d455 |
Moving around (G) |
|
d465 |
Moving around using equipment |
|
d470 |
Using transportation |
|
d510 |
Washing oneself |
|
d520 |
Caring for body parts |
|
d530 |
Toileting |
|
d540 |
Dressing |
|
d550 |
Eating |
|
d570 |
Looking after one’s health |
|
d640 |
Doing housework |
|
d660 |
Assisting others |
|
d710 |
Basic interpersonal interactions |
|
d770 |
Intimate relationships |
|
d850 |
Remunerative employment (G) |
|
d920 |
Recreation and leisure |
|
(G): ICF Category contained in the ICF Generic Set. |
|
China has taken the lead in implementing the ICF Generic Set system-wide in routine clinical practice (15). The pilot implementation phase revealed some inconsistencies in the understanding of the specified ICF categories. ICF categories are hierarchically ordered with increasing levels of specificity, as illustrated in Fig. 1 and exemplified for ICF category d440 Fine hand use. At each level, varying aspects of an ICF category can be assessed. The further specification of Fine hand use, whether it is, for instance, to pick something up or to grasp or release something, becomes specified only at the third level of the ICF. All ICF categories contained in the Generic and Rehabilitation Set are on the second level. Therefore, there is a need to concretize the different aspects contained in a category being assessed to ensure consistency in applying the ICF Generic and Rehabilitation Set in routine clinical practice. In building upon the lessons learned from the pilot phase of the system-wide implementation of the ICF in China (15, 16), the ICF Research Branch, a cooperation partner within the WHO Collaborating Centre for the Family of International Classifications in Germany, has developed a multi-stage national consensus process in collaboration with the Chinese leadership in rehabilitation, to generate simple, intuitive descriptions of the ICF categories contained in the ICF Generic and Rehabilitation Sets to enhance the utility of the ICF for routine clinical practice. The Chinese leadership in rehabilitation refers to representatives of the president’s cabinet from the 2 main rehabilitation societies, namely the Chinese Association of Rehabilitation Medicine (CARM) and the Chinese Society of Physical Medicine and Rehabilitation. The objective of this paper is to present the results of the consensus process to develop simple, intuitive descriptions of ICF categories to inform the system-wide implementation of the ICF in China.
METHODS
A multi-stage national consensus process was developed to generate simple, intuitive descriptions of categories contained in the ICF Generic and Rehabilitation Set.
Participants
The consensus process involved 3 groups, each with 7 experts. Experts were identified to be representative of the various regions of mainland China and to reflect varying clinical areas of expertise. Furthermore, clinicians nominated for the consensus process were in a leadership role and have shown committed interest in implementing the ICF at their respective sites. For each group, one expert was nominated as the moderator. In addition, an assistant from the project team was assigned to each group. The assistant was responsible for taking notes throughout the process and assisting the moderator with timing. While the moderator had the right to vote throughout the consensus process, the assistant did not. The participants in the consensus group constituted a closed group that remained stable throughout the entire process. National and international observers were welcomed throughout the entire process. The spoken language at the conference was Mandarin Chinese. For international observers, simultaneous English translation was available.
Phases of consensus process
The consensus process consisted of a preparatory phase, the consensus conference, and an implementation phase.
First phase: Preparatory phase
The preparatory phase consisted of developing an initial proposal for simple, intuitive descriptions developed by an international working group. More specifically, the proposed descriptions were developed by 2 researchers with extensive experience with the ICF and rehabilitation practice and then discussed with an international research team consisting of ICF and rehabilitation experts from within and outside China. The following principles were applied: first, the initial proposal for simple, intuitive descriptions needed to be as close as possible to the original definition of the ICF category as described in the ICF. Secondly, considering the third-level ICF category labels and descriptions is important to gain a better understanding of the aspects covered in the second-level category. Thirdly, a new proposal was developed only if the original definition of the respective ICF category and the further specification on the third level of the classification did not lead to a simple, intuitive description, based on the judgement of the research team.
Second phase: Consensus conference
Fig. 2 illustrates the flow chart of the consensus process.
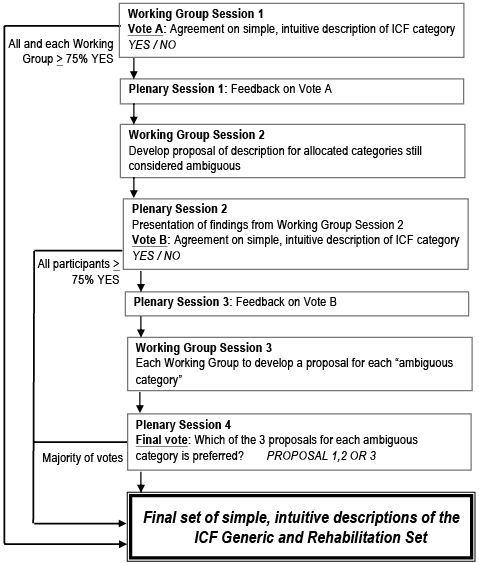
Fig. 2. Consensus conference. ICF: International Classification of Functioning, Disability and Health.
In working group session 1, participants were asked to review the proposed descriptions first individually, and then discuss them in their working groups. After discussing a given ICF category, the moderator instructed the group that each participant had to vote in secret whether he or she agreed or disagreed that the description was simple and intuitive. Disagreement implied that the description was still ambiguous and required further revision. Consensus was achieved if an ICF category achieved 75% or more agreement in each group. The results of vote A were presented in plenary session 1.
For working group session 2, the ICF categories that did not achieve consensus were distributed equally across the 3 groups. Each group was asked to develop a new proposal for a simple, intuitive description for the ICF categories assigned to it. The groups were provided with the original definition of the respective ICF category, the first proposal of a simple, intuitive description, which was not agreed upon, and discussion notes from the first phase. All the descriptions were compiled and presented to all participants in plenary session 2 for voting. This time the vote took place in the plenary, and consensus was achieved when at least 75% of all participants agreed that the new description was simple and intuitive. Subsequently, in plenary session 3 feedback on vote B was provided to participants.
In working group session 3, each group received all ICF categories that were still deemed ambiguous and were asked to develop a new description of each ICF category. The working groups again received the original description, the first and second proposals of a simple, intuitive description, and the discussion notes from the first and second phases. All descriptions were collated and participants were provided with 3 proposals (each developed by a different group) for review. In plenary session 4 participants were asked to vote for their preferred description out of the 3 options. The proposal with the majority vote was considered as the final simple, intuitive description for this given ICF category.
An access database was created to facilitate the organization of the materials and findings of the consensus process. The full process was conducted in Mandarin Chinese. As not all members of the study team speak Chinese, and international observers attended the consensus conference, simultaneous translation was available. All materials were translated into English for analysis by the international study team. All discussion notes from the entire consensus process were analysed using qualitative content analysis.
Third phase: Implementation phase
The consensus process led to the implementation phase. An implementation task-force was established, which will be responsible for developing a user manual for the system-wide implementation of the ICF Generic and Rehabilitation Set. The manual will summarize the consensus process and details of how the ICF Generic and Rehabilitation Set can be applied in routine clinical practice to enhance consistency in administration and thus reliability of the data.
RESULTS
This paper presents the results of the preparatory phase, as well as phases 1–3 of the consensus conference, including the results of the qualitative content analysis of the main points for discussion throughout the consensus process. The implementation phase is ongoing.
Participants
The consensus conference was held in August 2014 in Suzhou, mainland China. Twenty-one health professionals (19 medical doctors, 2 therapists) who are in the position of a clinical leader (or sent on behalf of the leader) of a rehabilitation facility participated in the consensus conference, divided into 7 persons per group, participated in the consensus process. Their median time working in rehabilitation departments was 12 years (range 7–36 years). In terms of their areas of expertise, most of them worked in either neuro-rehabilitation (7) or orthopaedics (5) or in a combination of neuro-rehab and orthopaedics (6); in addition, 2 participants worked in internal medicine and 1 in paediatrics. Eight participants indicated that they work in an acute setting, 4 in a long-term rehabilitation setting, and 4 in acute and long-term settings.
Four ICF categories, b152 Emotional functions, b710 Mobility of joint functions, d710 Basic interpersonal interactions, and d920 Recreation and leisure, achieved consensus in vote A; 16 in vote B, and 8 in vote C, as specified in Table II. The final list of simple, intuitive descriptions of the ICF categories contained in the ICF Rehabilitation Set in Mandarin Chinese can be requested by the authors.
The main themes that emerged from qualitative content analysis of the notes taken throughout the consensus process refer to: (i) the different aspects contained in an ICF category, (ii) the use of examples in the simple, intuitive descriptions, and (iii) the frame of reference in coding.
|
Table II. Descriptive statistics of consensus ratings across the 3 phases of the process |
|||||||||
|
ICF Code |
ICF Category |
Vote A |
Vote B |
Vote C |
Consensus achieved |
||||
|
WG1 |
WG2 |
WG3 |
WG1 |
WG2 |
WG3 |
||||
|
b130 |
Energy and drive functions (G) |
0.00 |
0.00 |
14.30 |
47.60 |
0.00 |
20.00 |
1.00 |
Vote C |
|
b134 |
Sleep functions |
0.00 |
28.60 |
0.00 |
61.90 |
19.00 |
1.00 |
1.00 |
Vote C |
|
b152 |
Emotional functions (G) |
100.00 |
100.00 |
100.00 |
|
|
|
|
Vote A |
|
b280 |
Sensation of pain (G) |
100.00 |
71.40 |
100.00 |
95.20 |
|
|
|
Vote B |
|
b455 |
Exercise tolerance functions |
42.90 |
57.10 |
85.70 |
28.60 |
7.00 |
6.00 |
8.00 |
Vote C |
|
b620 |
Urination functions |
28.60 |
85.70 |
85.70 |
85.70 |
|
|
|
Vote B |
|
b640 |
Sexual functions |
100.00 |
71.40 |
85.70 |
100.00 |
|
|
|
Vote B |
|
b710 |
Mobility of joint functions |
100.00 |
100.00 |
100.00 |
|
|
|
|
Vote A |
|
b730 |
Muscle power functions |
100.00 |
100.00 |
14.30 |
100.00 |
|
|
|
Vote B |
|
d230 |
Carrying out daily routine (G) |
42.90 |
57.10 |
0.00 |
81.00 |
|
|
|
Vote B |
|
d240 |
Handling stress and other psychological demands |
14.30 |
14.30 |
14.30 |
57.10 |
11.00 |
3.00 |
6.00 |
Vote C |
|
d410 |
Changing basic body position |
100.00 |
71.40 |
14.30 |
90.50 |
|
|
|
Vote B |
|
d415 |
Maintaining a body position |
85.70 |
0.00 |
33.30 |
100.00 |
|
|
|
Vote B |
|
d420 |
Transferring oneself |
71.40 |
42.90 |
14.30 |
90.50 |
|
|
|
Vote B |
|
d450 |
Walking (G) |
0.00 |
28.60 |
14.30 |
95.20 |
|
|
|
Vote B |
|
d455 |
Moving around (G) |
0.00 |
14.30 |
28.60 |
81.00 |
|
|
|
Vote B |
|
d465 |
Moving around using equipment |
100.00 |
42.90 |
14.30 |
61.90 |
9.00 |
11.00 |
1.00 |
Vote C |
|
d470 |
Using transportation |
0.00 |
42.90 |
0.00 |
100.00 |
|
|
|
Vote B |
|
d510 |
Washing oneself |
28.60 |
71.40 |
57.10 |
100.00 |
|
|
|
Vote B |
|
d520 |
Caring for body parts |
0.00 |
14.30 |
28.60 |
66.70 |
18.00 |
0.00 |
3.00 |
Vote C |
|
d530 |
Toileting |
0.00 |
0.00 |
0.00 |
76.20 |
|
|
|
Vote B |
|
d540 |
Dressing |
0.00 |
42.90 |
14.30 |
42.90 |
11.00 |
7.00 |
3.00 |
Vote C |
|
d550 |
Eating |
0.00 |
14.30 |
14.30 |
90.50 |
|
|
|
Vote B |
|
d570 |
Looking after one’s health |
85.70 |
100.00 |
0.00 |
42.90 |
10.00 |
7.00 |
4.00 |
Vote C |
|
d640 |
Doing housework |
28.60 |
85.70 |
100.00 |
100.00 |
|
|
|
Vote B |
|
d660 |
Assisting others |
0.00 |
85.70 |
28.60 |
61.90 |
7.00 |
8.00 |
6.00 |
Vote C |
|
d710 |
Basic interpersonal interactions |
100.00 |
100.00 |
100.00 |
|
|
|
|
Vote A |
|
d770 |
Intimate relationships |
100.00 |
57.10 |
14.30 |
47.60 |
6.00 |
0.00 |
15.00 |
Vote C |
|
d850 |
Remunerative employment (G) |
0.00 |
42.90 |
14.30 |
95.20 |
|
|
|
Vote B |
|
d920 |
Recreation and leisure |
100.00 |
100.00 |
100.00 |
|
|
|
|
Vote A |
|
(G): ICF Category contained in the ICF Generic Set; WG: working group. |
|||||||||
Different aspects contained in a given ICF category. This theme refers to the objective of this consensus conference and addresses the different aspects contained in an ICF category. Participants discussed whether, for example, b620 Urination functions refers to urinating freely, to being incontinent as an indicator of an impairment of urination functions, and to the time needed to discharge urine. The initial proposal “Urination function refers to frequency and control of discharge of urine” was modified throughout the consensus process into “Urination function refers to the ability to voluntarily control and discharge urine”. In some instances the discussion as to what is contained in an ICF category also referred to questions about the wording and use of terms in the ICF and its different language versions. For instance, it was discussed whether the Chinese translation of d550 Eating includes swallowing. Based on these discussions, the initial proposal of “Eating refers to eating food that has been served, bringing it to the mouth, cutting or breaking food into pieces, opening bottles and cans, and using eating utensils” has been changed in the consensus process to “Eating refers to bringing food into the mouth by using appropriate eating utensils and swallowing the food”.
Use of examples in the simple, intuitive descriptions. Participants discussed that using examples would enhance clarity, but might also make descriptions more culturally or geographically specific. For instance in the original definition of the ICF category d465 Moving around using equipment, examples of using skates, skis or scuba equipment were mentioned. If in a given region, e.g. skiing or diving is not an option given the natural environment, having such examples listed would make the description more comprehensive rather than simple. Therefore, the initial proposal of “Moving around using equipment refers to moving the whole body from one place to another, on any surface or space, by using specific devices designed to facilitate moving around” changed throughout the consensus process into “Moving around using equipment refers to moving from one place to another by using specifically-designed devices (e.g. wheelchairs, canes) to facilitate moving around”. On the other hand it was discussed that the same wording may have a different meaning across cultures, such as doing housework or carrying out daily routine. Including examples may clarify the meaning in these cases and the initially proposed description of “Doing housework refers to managing a household by cleaning living area, washing and drying clothes, using household appliances, storing daily necessities and disposing of garbage” achieved consensus in vote B with no further modifications.
Frame of reference for coding. In this theme topics discussed reflected experiences and challenges that participants encountered in previous usage of the ICF in their practice. For example, b455 Exercise tolerance functions refers in its original description to “respiratory and cardiovascular capacity as required for enduring physical exertion” and was revised into “ability that is required for enduring a certain time or intensity of exercise”. Participants raised the question as to whether some specification of time and intensity is required to make the understanding of this ICF category intuitive. Another example refers to d850 Remunerative employment, where the question was raised o as to whether it matters when the performance is limited due to factors within or outside the person. To clarify these considerations in the simple, intuitive descriptions, the initial proposal of “Remunerative employment refers to engaging in remunerative work” was revised into “Remunerative employment refers to engaging in all aspects of work for payment, including full- or part-time or self-employed, and performing the tasks of the job in an appropriate and timely manner”. Some gender issues were also raised in this context. For instance, with reference to d640 Doing housework, it was discussed how to deal with this ICF category if, for example, a man’s ability to do housework does not necessarily matter if it is done for him. Related to age and d920 Recreation and leisure, some participants challenged whether there are activities that are independent of age. At certain times in a person’s life, e.g. when they have a young family, recreation and leisure may not be at the forefront compared with caring for the family.
DISCUSSION
This study presents a national, multi-phase, consensus process to develop simple, intuitive descriptions of ICF categories contained in the ICF Generic and Rehabilitation Sets to serve as the foundation for ICF-based tools for routine clinical practice. This process has been part of a larger effort toward the system-wide implementation of the ICF in routine clinical and rehabilitation practice to allow for the regular and comprehensive evaluation of health outcomes most relevant for the monitoring of quality of care. While the ICF serves as the universal language for reporting functioning to be understood by various stakeholders in the health system, the consensus process provided a frame for further concretizing these ICF categories to facilitate their consistent understanding when used in routine practice.
The themes discussed throughout the consensus process provide a valuable resource for the implementation task force to further develop a user manual. The advantages and disadvantages of using examples in the simple, intuitive descriptions voiced in the process point to the merit of having examples to enhance the understanding and practical applications of the descriptions. While participants mainly refrained from using examples in the descriptions, examples can be included in the user manual and subsequent teaching materials. Challenges regarding the relevance of certain ICF categories for individuals of a certain age or gender were named. In this context it is worth bearing in mind that the ICF provides a universally applicable, neutral framework. It can be applied across cultures and individuals to describe a person’s functioning in a given domain. This needs to be separated from, for example, the relevance of a certain activity for a person at a given time or whether the ICF categories and their specifications can be used to create measures that are invariant across relevant groups. The latter is an empirical question and requires further psychometric studies.
Building upon the categories in the ICF Rehabilitation Set implies that the data captures aspects of functioning that are important across health conditions. Furthermore, having consensus on their semantic and conceptual meaning facilitates the process toward consistently applying them within and across systems. As in any cross-cultural adaptation process, the semantic and conceptual equivalence must be sustained. Semantic equivalence refers to the meaning of wording of a category, and conceptual equivalence to the relevance and meaning of the concept under investigation (17). The consensus process detailed in this study must ensure semantic and conceptual equivalence of any consensus-based description with the original ICF definitions. This principle also applies if a similar study is conducted in another language. Adhering to this principle is important to not threaten the comparability of data.
The simple, intuitive descriptions of ICF categories contained in the ICF Rehabilitation Set are an important step toward developing ICF-based clinical data collection tools. Having functioning information available in a systematic way will ensure that this information is available to all stakeholders in the health system, who can, in turn, use it to inform their decision-making at the clinical as well as management level, and ultimately contribute to optimizing the quality of care. Furthermore, the ICF was designed to foster interdisciplinary communication. In the Chinese consensus conference participants had a predominantly medical background. For similar efforts we strongly recommend aiming for an interdisciplinary group of participants.
Successful implementation of any innovative system builds upon a strong network of support and advocacy, including strong support of senior management and clinical leadership (18). The system-wide implementation of the ICF in rehabilitation practice is an ongoing effort aligned with the rehabilitation quality control system of the People’s Republic of China, one of the main research priorities launched by the National Health and Family Planning Commission (previously the Health Ministry). This quality control system is set up to monitor people’s functioning as the primary outcome of rehabilitation services (19). Hence, there is strong support and advocacy at the level of policy and clinical leadership available for this implementation project. Furthermore, the Chinese approach illustrates that there is a need for dedicated time and resources to foster an information system that is consistently applied across care settings to monitor quality in healthcare. All of these factors; support by leadership, time and resources, have been described to contribute to the successful diffusion of innovations in healthcare systems (20).
On a national level, the system-wide ICF implementation in rehabilitation may serve as a future model for the whole healthcare system. On an international level, the Chinese approach can serve as a model to facilitate ICF implementation in rehabilitation and ultimately in the healthcare system at large. Regardless of in which national context this process is applied, it is important to ensure consistency between the descriptions revealed in the consensus process and the original definition of the ICF categories. The process of transforming the original definitions into simple, intuitive descriptions of ICF categories can be seen as adaptation of the ICF into an easily accessible language for clinical practice.
ACKNOWLEDGEMENTS
The authors would like to acknowledge the following persons for providing support for this study: Wen Zhang, Shanghai General Hospital; Yanyan Yang, Peking University Third Hospital; Zhihai Lv, Third Affiliated Hospital of Jiamusi University; Long Jiao, Zhoushi People’s Hospital; Yuanbiao Liu, Second Affiliated Hospital of Nanjing Medical University; Qiaojun Zhang, Second Affiliated Hospital of Xi’an Jiaotong University; Weibo Lu, Shanghai First Rehabilitation Hospital; Zhuo Xu, Chinese-Japanese Friendship Hospital of Jilin University; Weiqun Song, Xuanwu Hospital Capital Medical University; Jinyu Yan, Second Affiliated Hospital of Inner Mongolia Medical University; Rongqiu Mao, First Affiliated Hospital of Guangxi Medical University; Xiaoyan Song Beijing United Family Rehabilitation Hospital; Yajun Mao, Hangzhou Hospital of the Chinese People’s Armed Police Force; Jianhua Lin, Shanghai Sunshine Rehabilitation Hospital; Hongwei Zhai, Xuzhou Central Hospital; Zhen Feng, First Affiliated Hospital of Nanchang University; Baolan Wang, First Affiliated Hospital of Xinjiang Medical University; Xiaojun Zhu, Jiangsu Province Official Hospital; Tiechen Guo, Tongji Medical College Huazhong University of Science and Technology; Qing Xie, Rui Jing Hospital Shanghai Jiao Tong University School of Medicine; Pu Wang, West China Hospital of Sichuan University. In addition, the authors acknowledge the support of the assistants: Shouguo Liu, First Affiliated Hospital of Nanjing Medical University; Jiayan Jiang, First Affiliated Hospital of Nanjing Medical University; Feng Jiang, First Affiliated Hospital of Nanjing Medical University. Also, the authors acknowledge the work of the translators: Mingyue Xiao, First Affiliated Hospital of Nanjing Medical University; and Yu Zheng, First Affiliated Hospital of Nanjing Medical University. For support in setting up the programme used throughout the conference, the authors are indebted to Wolfgang Segerer, Swiss Paraplegic Research, Switzerland.
REFERENCES

