Marita Bengtsson, MD1 and Alison K. Godbolt, MRCP, MD1,2
From the 1University Department of Rehabilitation Medicine Stockholm, Danderyd Hospital and 2Institute of Clinical Sciences Danderyd Hospital, Karolinska Institutet, Stockholm, Sweden
OBJECTIVE: To undertake a systematic review of the evidence for the effect of acetylcholinesterase inhibitors (AChEIs) on cognition late after moderate or severe traumatic brain injury.
BACKGROUND: Cognitive impairment after traumatic brain injury has significant consequences for the individual and society. Cholinergic pathways play an important role in cognitive processing and a hypocholinergic state exists in the chronic phases after traumatic brain injury. AChEIs are already used off-label to treat patients with traumatic brain injury.
Data sources and study selection: PubMed, CINAHL, PsycINFO, the Cochrane Collaboration and Web of Science were searched with pre-specified criteria between 1999 and June 2015.
Data extraction and synthesis: A total of 153 studies were identified. None met pre-specified criteria. The criteria were revised in order to identify studies that may provide useful information despite some risk of bias. Three studies met the revised criteria and were evaluated by 2 reviewers using the Swedish Council on Health Technology Assessment grading system, based on GRADE. Key findings and limitations were tabulated. One study found no effect and 2 found limited effect.
CONCLUSION: Large randomized controlled studies are needed to establish whether AChEIs are effective for cognition late after moderate or severe traumatic brain injury. Clinicians should be aware of the weak evidence base when considering the off-label use of AChEIs.
Key words: traumatic brain injury; cholinesterase inhibitors; treatment; cognition.
J Rehabil Med 2016; 48: 1–5
Correspondence address: Alison Kate Godbolt, Institute of Clinical Sciences Danderyd Hospital, Karolinska Institutet, SE-182 88 Stockholm, Sweden. E-mail: alison.godbolt@ki.se
Accepted Oct 23, 2015; Epub ahead of print Dec 11, 2015
INTRODUCTION
Traumatic brain injury (TBI) is a major public health issue, with an estimated annual incidence of more than 10 million worldwide (1). Mortality has decreased over the past 20 years, but TBI remains a leading cause of long-term neurological disability in young and middle-aged adults (2). Of those sustaining severe injury, less than 40% have returned to full-time work 2 years after the trauma (3). Interventions to improve functioning after TBI are therefore important.
Cognitive impairment is a common sequela of TBI, and often includes deficits in arousal, attention, memory, speed/rate of information processing, language, social communication and executive function (4–7). Cognitive impairment has been linked to poor long-term outcome in the areas of independent living, return-to-work, and community integration (4, 8). Cognitive impairments associated with TBI are thus logical therapeutic targets, the treatment of which could result in decreased handicap, improved quality of life, and improved functioning in everyday life.
Cholinergic deficits contribute to cognitive impairment after TBI (5). The cholinergic neurones in the hippocampal and limbic systems, which are important for attention and memory processes, are vulnerable to trauma due to the bony structure of the skull. The period of increased cholinergic activity that occurs directly after trauma later develops into a chronic hypocholinergic state (5).
Central-acting acetylcholinesterase inhibitors act to increase the amount of endogenous acetylcholine at the synaptic sites, and thus could theoretically alleviate the cholinergic-mediated symptoms of chronic TBI. Previous studies have suggested positive effects of first-generation acetylcholinesterase inhibitors (AChEIs), such as physostigmine (6, 7) in improving long-term memory in chronic TBI, but their short half-life and systemic side-effects have limited their use.
Central-acting AChEIs with fewer side-effects were therefore developed, and in 1997 the US Food and Drug Administration (FDA) approved donepezil, followed by rivastigmine and galantamine, for the treatment of cognitive dysfunction in Alzheimer’s disease. These medications have been shown to enhance cholinergic function and to improve measures of cognition and global functioning in patients with mild to moderate Alzheimer’s disease (9). They are not approved for use following TBI, although some clinicians use them off-label. Previous reviews of the effects of the AChEIs donepezil, galantamine and rivastigmine on cognition after TBI in the sub-acute and chronic stages found insufficient evidence to support their use (10–12).
The aim of this study is to undertake an updated, systematic review of the literature to determine whether central cholinesterase inhibitors (donepezil, galantamine or rivastigmine) have a meaningful effect on cognition in patients with chronic TBI, in order to assist clinicians who may be considering the off-label use of AChEIs in the treatment of patients with TBI.
METHODS
A systematic review was performed of the evidence for effectiveness of central cholinesterase inhibitors in improving cognition in patients who have experienced a TBI according to pre-specified criteria. The process for study inclusion is summarized in a PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow chart (Fig. 1).
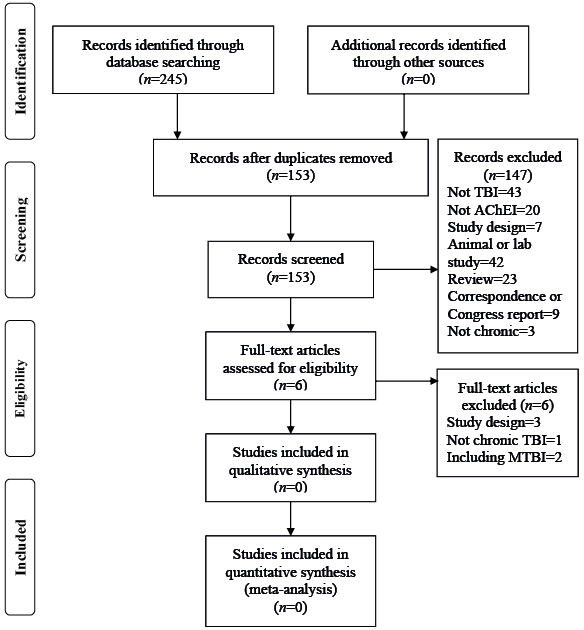
Fig. 1. PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram. AChEIs: acetylcholinesterase inhibitors; TBI: traumatic brain injury; MTBI: mild TBI.
Inclusion criteria
Population. Persons 15 years of age or older at trauma, with moderate or severe TBI, due to blunt trauma to the head.
Intervention. Donepezil, galantamine or rivastigmine to improve cognition, intervention to start at least 12 months after injury, to minimize confounding due to spontaneous recovery.
Study design. Randomized controlled trials (RCT), controlled non-randomized trials (CT), and cohort cross-over studies with a minimum of 10 subjects, to avoid underpowered studies.
Outcome. Objective assessment of cognition, evaluated with validated neuropsychological tests.
Language. English.
Types of publication. Reports in peer-reviewed journals.
Publication date. April 1999 to 18 June 2015. The start date was chosen because of the introduction of central cholinesterase inhibitors in the late 1990s.
Exclusion criteria
Studies where the author had not defined the following: severity of brain injury; neurological or psychiatric illness that could affect cognition; concomitant treatment with centrally acting drugs, that could affect cognition; active drug or alcohol misuse; mild TBI, were excluded to avoid the risk of uncertainties about causality. Uncontrolled case series and case reports, which have a high risk of bias, were also excluded.
Search strategy
An electronic search of published literature was performed using PubMed, CINAHL, PsycINFO, the Cochrane Collaboration and Web of Science databases. The search strategy included both free text and appropriate thesaurus terms for keywords, such as “brain injury”, “cholinesterase inhibitor”, “rivastigmine”, “galantamine” and “donepezil”, and is given in Table I. Filters used were publication date last 15 years 1999 to 29 April 2014 and English language. The searches were updated on 18 June 2015.
|
Table I. Search strategy |
|
1. ”brain injury, chronic” [MeSH Terms] OR ”brain injuries” [MeSH Terms]) OR ”brain hemorrhage, traumatic”[MeSH Terms]) OR ”diffuse axonal injury”[MeSH Terms]) OR ”brain concussion”[MeSH Terms]) |
|
2. ”traumatic brain injury”[Title/Abstract]) OR ”craniocerebral trauma”[Title/Abstract]) OR (”brain injury”[All Fields] OR ”brain injuries”[All Fields] OR ”diffuse axonal injury”[Title/Abstract]) |
|
3. 1 OR 2 |
|
4. cholinesterase inhibitors[MeSH Terms] OR cholinergic agents[MeSH Terms] |
|
5. rivastigmine OR ENA 713 OR ENA713 OR (”donepezil”[All Fields]) OR E2020 OR E 2020 OR (galanthamine OR galantamine OR galanthamin))) |
|
6. 4 OR 5 |
|
Combined sets |
|
7. 3 AND 6 |
|
Additional filter: English and Date (April 1999–29 April 2014) |
|
Additional articles, updated search 29 April 2014 to 18 June 2015: n = 17. Passed screening: 0. |
Data collection and analysis
After the electronic search 153 articles were identified for screening. Titles of all the citations were read and the citations that were clearly not related to TBI were removed. Of the remaining articles, abstracts were obtained and screened according to the inclusion and exclusion criteria. Articles not meeting the inclusion criteria or meeting any exclusion criteria were discarded. If there was any doubt about the relevance of the studies, the full text was retrieved. If a study was reported in more than 1 paper, data were extracted from the most relevant published paper.
The reference lists of all identified review articles and articles meeting the eligibility criteria were searched for any additional papers/studies. Experienced colleagues were contacted for any additional studies.
The retrieved articles were critically appraised by the 2 authors, using standardized checklists from the Swedish Council on Health Technology Assessment grading system (SBU) (http://www.sbu.se/en/About-SBU/). This is based on the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) system, and uses well-established methods for evaluating common issues and biases of various study designs, including RCTs, cohort studies and case-control studies.
RESULTS
After the electronic search 153 articles were retained for screening. Of these, 147 articles were discarded at the screening stage. Six full-text articles (13–18) were assessed for eligibility according to the predefined inclusion and exclusion criteria. None of these articles fulfilled the criteria. The criteria were therefore relaxed to allow evaluation of studies that, despite some risk of bias, may nevertheless provide useful information as a basis for future studies.
The following adjustments were made for the revised inclusion criteria:
• the range of TBI severity was extended to include mild TBI. This allowed inclusion of studies where severity of injury was not specified;
• the minimum number of patients was reduced to 5;
• subjective outcome measures were allowed;
• studies that had used a mix of validated and non-validated tests were included;
• studies including patients taking centrally acting drugs were allowed if the patients were on stabile medication;
• stable psychiatric illness during the study period was also allowed.
Three articles were found to meet the revised inclusion and exclusion criteria (13–15). These studies underwent critical review and are summarized below and in Table II. The remaining 3 articles did not meet revised criteria, due to inclusion of patients during the period of spontaneous recovery early after injury (17, 18), and due to non-controlled study design (16).
|
Table II. Summary of the included papers |
||||||||
|
Author Year Country |
Participants |
Testing |
Study design |
Intervention |
Primary outcome measures |
Results |
Risk of bias |
Limitations |
|
Tenovuo et al., (13) 2009 Finland |
n = 102 M/F %: 61/39 Age: mean 45 years All severities TSI: > 12 months Mean: 8 years |
Baseline 8 weeks 12 weeks 20 weeks |
RCT with a crossover design Single centre |
Rivastigmine 2.5–12 mg/day 8 weeks placebo 4 weeks washout 8 weeks rivastigmine |
Memory Attention Vigilance |
Primary outcome: Significant result for Sustained attention (Vigilance test OR 0.08) Attention (subtraction test OR 2.8) Secondary outcome: Subjective positive response in 45% (placebo 27%) |
Low to moderate |
Large dropout (32%) Some un-standardized tests Not stratified for disease severity Dropouts had more severe injury, concentration and memory problems at baseline Large number of primary outcome measures |
|
Silver et al., (15) 2006 USA |
n = 157 M/F %: 68/32 Age: mean 37 years All severities TSI: ≥ 12 months Mean: 7.5 years |
Primary outcome: 4, 8, 12 weeks Secondary outcome: Baseline and 12 weeks |
RCT Multi centre |
Rivastigmine 3–6 mg/day 12 weeks |
Verbal memory Attention Life Satisfaction |
Primary outcome: No significant results in attention or verbal memory Secondary outcome: Not significant, various neuropsychological tests |
Low |
Comorbidity Severity not specified Short treatment period |
|
Morey et al., (14) 2003 USA |
n = 7 M/F %: 71/29 Age: mean 31 years Does not specify severity TSI: ≥ 18 months Mean: 2.5 years |
Baseline 6 months, 6 months + 6 weeks, End of trial (12 months + 6 weeks) |
ABAC design Single centre |
Donepezil 5 mg 1 month 10 mg 5 months Washout 6 weeks Second phase 5 mg 6 months |
Memory |
Primary outcome: Visual memory and learning Significant for 10 mg (p < 0.05), but not for donepezil 5 mg |
Moderate |
Small study Changed protocol (dosage) at second phase Not blinded |
|
n: number of study population; TSI: time since injury; M: male; F: female; NPS: neuropsychological tests; RCT: Randomized controlled trials. |
||||||||
Tenovuo et al. (13) performed a single-centre, randomized double-blind, placebo-controlled trial with crossover design, comparing rivastigmine with placebo. They included 102 patients with chronic TBI of all severities. A wide array of primary outcome measures was used to evaluate memory, vigilance and attention. A significant effect was found for only 2/11 neuropsychological tests, measuring working memory and sustained attention, comparing rivastigmine with placebo.
Silver et al. (15) performed a multicentre, randomized double-blind placebo-controlled trial and included 157 subjects to receive either rivastigmine or placebo. The primary outcome was the percentage of patients who improved attention or verbal memory, as defined by at least 1 standard deviation (SD) improvement from baseline on specified neuropsychological tests. The study found no significant differences in the rivastigmine compared with the placebo-treated group.
Morey et al.’s pilot study (14) of 7 subjects with chronic TBI used a single-subject ABAC design, in which each subject served as their own control. Subjects underwent 2 6-month trials of donepezil, separated by a 6-week washout period. Four standardized tests were used measuring different aspects of memory. A significant improvement was shown in visual memory for subjects receiving donepezil 10 mg.
DISCUSSION
The evidence-base for the effect of AChEIs after TBI was found to be weak, based on a few relatively small studies with somewhat conflicting findings. That no studies met our original study criteria reflects important methodological weaknesses in this area of study. Even with our “relaxed” criteria (allowing inclusion of studies with a somewhat higher risk of bias), findings from the 3 studies included were conflicting. One study found no effect, and 2 found some limited effect. Factors contributing to difficulty in study interpretation include heterogeneous TBI severity in study patients, and the heterogeneity of outcome measures.
Our findings are similar to those of a previous systematic review published 7 years ago (10), which concluded that there was no evidence for using AChEIs, other than in experimental settings. In contrast to this previous review, we chose to exclude older AChEIS which have fallen out of use due to their long half-life and troublesome side-effects.
Since the last review (10) only one RCT has been published (13), which did not find a convincing effect of AChEIs. Although it has strengths, interpretation of this trial is made difficult by the very large number of outcome measures and lack of a clear definition before data collection of what was to be considered a clinically relevant effect. Dropout rate was high (32%), which is, however, approximately the same level as in the Alzheimer’s population, and the study was not stratified by injury severity.
The low number of studies and the methodological weaknesses were surprising, given the often serious consequences of TBI for the individual and society, and evidence for the role of cholinergic pathways in cognitive processing. Well-designed, larger scale RCTs are needed.
According to www.clinicaltrials.org (accessed 2015 Oct 6) 3 trials of AChEIs for TBI patients are currently recruiting patients. The “RIVET” trial evaluates a rivastigmine patch in patients with mild TBI (i.e. of interest, but not the target population for this review), the MEMRI-TBI-D trial evaluates donepezil for memory problems in patients after TBI of all severity (including recruitment of patients in the subacute period after injury) and a further study evaluates the effects of huperzine A on memory in the acute and subacute period after moderate to severe TBI. Although of interest, none of these studies meet the inclusion criteria for this review. Further study details can be found at www.clinicaltrials.org.
In addition, an online publication became available in September 2015 reporting a further trial marked as “terminated” on clinicaltrials.org (“CREATE” study (19)). This study included some patients without TBI and recruited patients earlier than one year after injury and, as such, would not have been eligible for inclusion in this review.
When defining the inclusion and exclusion criteria for this review we attempted to find a balance between inclusion of all relevant studies and avoiding the inclusion of studies with a high risk of bias, which may have affected the results. We would suggest that future studies pay careful attention to potential confounding factors, such as psychiatric comorbidity or substance misuse, which may affect both treatment effect and outcome assessment.
Findings from secondary and post-hoc analyses should be treated with caution when the primary outcome findings are negative or inconclusive. Such findings may, however, usefully guide future studies. For example, Silver et al. (15) found, on post-hoc analysis, that a sub-group of “severe cases” (memory) was found to respond better to rivastigmine than to placebo. Future studies could appropriately incorporate pre-planned analyses stratified for severity of memory impairment, or even select patients for inclusion based on the presence of more severe memory impairment.
In conclusion, this review found no convincing evidence of positive effects of current-generation AChEIs on cognition in patients with chronic TBI. There is still a lack of well-designed multicentre RCTs. Some individuals seem to have some positive effects from AChEIs, but off-label use must still be considered experimental.
REFERENCES

