Birgit Prodinger, PhD, MSc1,2,3, Carolina Saskia Ballert, MSc1,3 and Alarcos Cieza, PhD, MSc, MPH1,4,5, for the SwiSCI Study Group
From the 1Swiss Paraplegic Research (SPF), 2ICF Research Branch, a cooperation partner within the World Health Organization Collaborating Centre for the Family of International Classifications in Germany (at DIMDI), 3Department of Health Sciences and Health Policy, University of Lucerne, Lucerne, Switzerland, 4Faculty of Social and Human Sciences, University of Southampton, Southampton, UK and 5Department of Medical Informatics, Biometry and Epidemiology – IBE, Public Health and Health Services Research, Research Unit for Biopsychosocial Health, Ludwig-Maximilians-University (LMU), Munich, Germany
OBJECTIVE: Cohort studies are an appropriate method for the collection of population-based longitudinal data to track people’s health and functioning over time. However, describing and understanding functioning in its complexity with all its determinants is one of the biggest challenges faced by clinicians and researchers.
DESIGN: This paper focuses on the development of a cohort study on functioning, outlining the relevant steps and related methods, and illustrating these with reference to the Swiss Spinal Cord Injury Cohort Study (SwiSCI).
Methods and results: In setting up a cohort study the initial step is to specify which variables are to be included, i.e. what to assess. The International Classification of Functioning, Disability and Health (ICF) is valuable in this process. The second step is to identify how to assess the specified ICF categories. Existing instruments and assessments can then be linked to the ICF.
CONCLUSION: The methods outlined here enable the development of a cohort study to be based on a comprehensive perspective of health, operationalized through functioning as conceptualized and classified in the ICF, yet to remain efficient and feasible to administer.
Key words: International Classification of Functioning, Disability and Health; standardized reporting; cohort study; epidemiology.
J Rehabil Med 2016; 48: 131–140
Correspondence address: Birgit Prodinger, ICF Unit, Swiss Paraplegic Research (SPF), CH-6207 Nottwil, Switzerland. E-mail: birgit.prodinger@paraplegie.ch
Accepted Sep 21, 2015; Epub ahead of print Feb 1, 2016
INTRODUCTION
Gaining an understanding of health, in all its complexity with all of its components and determinants, is one of the biggest challenges faced by clinicians, health researchers and policy-makers. Such understanding requires consideration of the interaction of a health condition with its related impairments and the person’s environment, which together yield the person’s experience of living with a given health condition. Describing the occurrence and distribution of relevant outcomes related to health, informing the generation of specific hypotheses, and providing the foundation for the planning and evaluation of health and related policies and programmes is at the core of descriptive epidemiology (1). Within epidemiology, cohort studies constitute an observational study design suitable for the collection of population-based longitudinal data (2). Common outcomes of cohort studies are morbidity, including the incidence and prevalence of a health condition, and mortality (3). Functioning, which according to the World Health Organization’s (WHO) International Classification of Functioning, Disability and Health (ICF) is the operationalization of health from a comprehensive perspective (4, 5), is also a relevant outcome (6), but this has not, as yet, received as much attention.
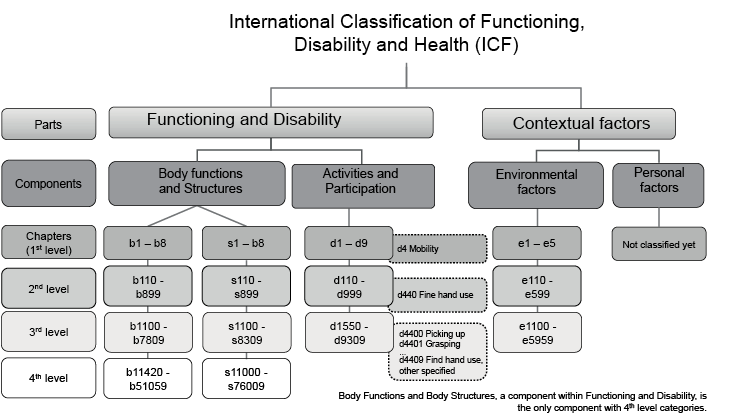
Functioning is an umbrella term for the interaction of a health condition, including impairments of body functions and structures of a person, activities and participation of a person with personal and environmental factors (4). The ICF, which offers an internationally agreed standard for describing and monitoring functioning, has been endorsed by all WHO member states (4). As shown in Fig. 1, the ICF is structured into 2 parts, each of which is further specified into 2 components, which together classify more than 1,450 ICF categories. ICF categories are the units of the classification and are presented in the ICF with alphanumeric codes that reflect: (i) the part to which the category belongs, e.g. codes starting with a d belong to the component Activity and Participation, and (ii) their location in the hierarchy, e.g. codes on the second level have 3 digits (e.g. d440 Fine hand use) and codes on the third level 4 digits (e.g. d4402 Manipulating). The specificity of an ICF category increases with each level. The ICF provides a promising conceptual framework and, at the same time, an exhaustive classification for setting up a cohort study of functioning. However, ICF categories have not been developed as operational variables, but rather mutually exclusive and cumulatively exhaustive units of a classification to describe a universal human experience. Hence, the ICF neither specifies which ICF categories of a component are the most relevant to describe, nor in which context, and it certainly does not determine how to measure those categories that are relevant. Nevertheless, once relevant ICF categories have been specified, data on these aspects of functioning can be derived by conducting clinical tests, interviews or surveys, as well as through existing registries or hospital and health statistics. Regardless of which source the information is derived from, a commonly agreed framework is needed that provides the conceptual foundation to facilitate the development of a new cohort study on functioning, in particular to facilitate the systematic selection of which variables to include, while at the same time enabling the comparability of existing data sets. The question remains, therefore, how to proceed from the complex phenomenon of functioning to operational variables for a cohort study designed to describe and understand functioning over time.
This paper tackles this challenge by outlining the steps and related methods in the development of a cohort study on functioning, and illustrating these steps and methods by drawing on the example of the Swiss Spinal Cord Injury Cohort Study (SwiSCI). SwiSCI, we believe, can serve as a model for this purpose, as it is one of the few cohort studies that has as its main objective describing the functioning of people living with a health condition over their life-span (7).
METHODS
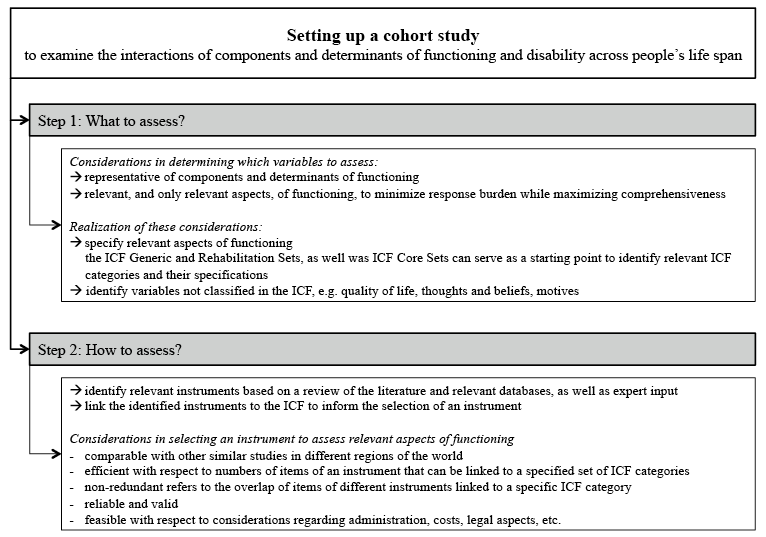
There are 2 main steps involved in setting up a cohort study on functioning. The first is to specify the relevant aspects of functioning to be considered in the cohort study. Secondly, suitable instruments for the assessment of these aspects must be identified. Fig. 2 outlines these 2 steps and summarizes the relevant considerations in each.
Step 1: Specification of relevant aspects of functioning to be considered in a cohort study on functioning
The first step in setting up a cohort study on functioning is to determine the relevant domains for assessing the components and determinants of functioning for a given clinical population. This process serves the specification of the variables to be included in the study and responds to the question what to assess. The strength of the ICF is its comprehensiveness, although this also makes it impractical for use in routine practice or research. A systematic approach is needed to determine the ICF categories that are most relevant in a given setting or context. In response to this challenge, ICF Core Sets have been developed. These are sets of ICF categories that have been identified by means of a multi-phase and multi-method, international consensus process for certain health conditions (8). A comprehensive and brief version of the Core Sets exists for each health condition for which an ICF Core Set is available. Comprehensive ICF Core Sets contain a number of ICF categories necessary to be sufficiently comprehensive in describing the typical spectrum of functioning of a person with a given health condition. Brief ICF Core Sets are a selection of ICF categories from the corresponding Comprehensive ICF Core Set and are recommended for use in clinical studies (9). Each ICF Core Set can be complemented with any category of the ICF, as deemed relevant in a given context.
There are 2 points worth mentioning regarding ICF Core Sets. First, their development aimed to identify the most relevant ICF categories to be consistently described and reported in a given health condition based on what we know from the literature and from experts, including patients themselves, across the world (8). While these ICF categories are definitely significant for a comprehensive description of functioning, we also need to ensure that the ICF Core Sets contain those ICF categories that make it possible to best describe variations in functioning within and between individuals and populations. In response to this challenge, additional statistical sets have been developed that build upon, and are complementary to, the existing ICF Core Sets. Statistical sets are compiled based on regression models using self-reported and clinician-reported health as dependent variable and the ICF categories from the comprehensive ICF Core Sets as independent variables (10). The ICF categories found to have most explanatory power of self-reported health in a given health condition can then be added to the ICF categories that were selected from the literature and expert opinion during the multi-stage consensus process in the development of ICF Core Sets.
Secondly, the health condition-specific focus of ICF Core Sets has limited value for ensuring comparability with the general population, as well as with other clinical populations. To address this problem, ICF Generic and Rehabilitation Sets have been developed psychometrically. The ICF Generic Set contains 7 ICF categories that have shown statistically to best describe functioning in people across health conditions and the general population (11). When the focus is specifically on clinical populations, these ICF categories can be complemented with 23 ICF categories into a more extended ICF set of 30 ICF categories, referred to as the ICF Rehabilitation Set (12). These additional 30 ICF categories best describe functioning across various clinical populations and across the continuum of rehabilitation care from acute, to early post-acute and long-term care. To summarize, the ICF Generic and Rehabilitation Sets contain the ICF categories most relevant to compare information across the general and clinical populations. ICF Core Sets for a specific health condition complement the ICF Generic and Rehabilitation Set with ICF categories that are most relevant to be described in a specified clinical population. Furthermore, a statistical set adds additional relevant ICF categories by specifying those ICF categories needed to best describe variations in functioning within a given health condition. Any additional ICF category that is relevant in a given context or for a particular patient can subsequently be added from the entirety of the ICF.
A further consideration is that ICF categories are ordered hierarchically, with increasing levels of specificity, as illustrated in Fig. 1 by a detailed illustration for the ICF category d440 Fine hand use. The majority of ICF categories contained in the ICF Core Sets are on the second level. Regardless of the level in the hierarchy, in order to be transparent concerning the operational variables that need to be considered in a cohort study some further specification of identified categories may be required. Category specification therefore refers to the identification of the aspect of an ICF category that is particularly relevant to assess in a given population As highlighted by Cieza et al. (23), category specifications need to relate to the same component of functioning as the category itself (e.g. only body functions can be specifications of Body Functions) and may or may not correspond to a more detailed level of ICF category. For instance, the category specification for b152 Emotional functions may include anxiety in its specification, which is covered by neither of the third-level ICF categories. On the other hand, the category specification for b134 Sleep functions may refer to sustaining sleep throughout the night, which corresponds to b1342 Maintenance of sleep. The proposed methods therefore require a further systematic literature review of completed and ongoing studies and international recommendations, in order to determine the most relevant constructs in a given field and population related to an ICF category to be accounted for as variables in clinical research and practice specific to the area of study (13).
Step 2: Identification of how to assess relevant aspects of functioning
Once it has been specified what to assess, the second step is to identify how to assess the specified ICF categories. Given the number of instruments and assessment tools that have been developed over the decades there is no need to develop new instruments, but rather to link existing instruments and assessments to the ICF. To identify relevant instruments, various sources of information can be used, including a review of the literature, existing databases on outcome measures commonly used in the field (e.g. 14), and expert feedback on what is used in practice. Relevant instruments can then be linked to the ICF based on established rules (15, 16).
Once relevant items, sub-scales, or full instruments have been specified, the researchers need to reflect on the properties of an instrument, which include comparability, efficiency and non-redundancy, reliability and validity, as well as feasibility to finally decide which to select (17). Comparability with other studies or routine clinical practice is important, as it influences whether the study findings can be later pooled or compared with data and knowledge in the field of practice. In this context “efficiency” refers to the number of items of an instrument that can be linked to a specified ICF category, based on the selected ICF Core Sets and the total number of items in an instrument. The instrument is most efficient if most of its items link to an ICF category that has been selected as relevant for consideration in a cohort study on functioning. Redundancy points to the number of items derived from various identified instruments and linked to the same ICF category in relation to the overall number of ICF categories identified in the linking process. The instrument is most redundant if the items of both instruments are linked to the same ICF categories. There are no predefined cut-off points for when an instrument is inefficient or redundant. Examining these properties is meant to provide relevant information on the content coverage of relevant ICF categories in the process of deciding which one of several instruments to use. To ensure that the data gathered are eventually reliable and valid, the psychometric properties of instruments must be examined. Existing standards, such as the Consensus-based Standards for the Selection of Health Measurement Instruments (18), may serve to guide the critical appraisal of instruments. Feasibility refers to practical considerations, such as the administration mode (e.g. patient-administered vs expert-administered), costs and legal aspects associated with administering a certain instrument, as well as the acceptability of certain questions in a given (sub-)population and length of an instrument. To make the final determinations of which items, sub-scales or instruments to use, researchers need to ensure that, as far as possible, the respondents’ burden is minimized, while comprehensiveness and comparability are maximized (17). Additional variables on aspects not classified in the ICF, e.g. quality of life, thoughts and beliefs, and personal motives can be added when meaningful for a given study.
Development of SwiSCI as a case in point
The process outlined in Fig. 2 has been followed in the case of SwiSCI. We present here examples from the development of SwiSCI. The full materials can be requested from the authors.
Step 1: What to assess in SwiSCI. The aim of SwiSCI is to examine the components and determinants of functioning in people living with spinal cord injury (SCI) in Switzerland. Using the ICF Generic and Rehabilitation Sets as the starting point for specifying variables ensured that most relevant aspects of functioning for people with SCI were considered, in addition to aspects of functioning relevant for comparison across different health conditions. Subsequently, SCI-specific Brief ICF Core Sets were identified; one for the early post-acute (19) and another for the long-term (20) context. In addition, a statistical set has been developed for SCI (10). It is worth mentioning that the latter set was developed only after SwiSCI was launched, so that the categories in the statistical set were not considered in the first survey wave. Table I outlines the list of ICF categories contained in SwiSCI and lists the ICF set from which they are derived. Fig. 3 outlines the linking of these items to the components of the ICF.
|
Table I. International Classification of Functioning, Disability and Health (ICF) categories contained in the Swiss Spinal Cord Injury Cohort Study (SwiSCI), and the ICF set from which they were derived |
||||||||||||
|
ICF Code |
Title |
ICF Generic Set |
ICF Rehabilitation Set |
Brief EPA |
90%a EPA |
Pat EPA Rankingb |
HP EPA Rankingb |
Brief LT |
90%a LT |
Pat LT |
Pat LT Rankingb |
HP LT Rankingb |
|
b126 |
Temperament and personality functions |
|
|
|
|
17 |
12 |
|
|
1 |
6 |
27 |
|
b130 |
Energy and drive functions |
1 |
1 |
|
|
6 |
|
|
|
1 |
7 |
7 |
|
b134 |
Sleep functions |
|
1 |
|
|
|
|
|
|
1 |
5 |
22 |
|
b152 |
Emotional functions |
1 |
1 |
1 |
|
11 |
|
1 |
|
1 |
4 |
6 |
|
b270 |
Sensory functions related to temperature and other stimuli |
|
|
|
|
|
19 |
|
|
|
|
|
|
b280 |
Sensation of pain |
1 |
1 |
1 |
|
|
|
1 |
|
|
|
|
|
b415 |
Blood vessel functions |
|
|
|
|
28 |
7 |
|
|
|
|
|
|
b420 |
Blood pressure functions |
|
|
|
|
|
|
|
|
|
|
29 |
|
b430 |
Haematological system functions |
|
|
|
|
27 |
11 |
|
|
|
|
|
|
b440 |
Respiration functions |
|
|
1 |
|
|
|
|
|
|
|
|
|
b445 |
Respiratory muscle functions |
|
|
|
|
|
15 |
|
|
|
|
|
|
b455 |
Exercise tolerance functions |
|
1 |
|
|
|
|
|
|
|
|
35 |
|
b525 |
Defecation functions |
|
|
1 |
|
|
|
1 |
|
|
|
|
|
b530 |
Weight maintenance functions |
|
|
|
|
|
|
|
|
|
|
26 |
|
b550 |
Thermoregulatory functions |
|
|
|
|
|
16 |
|
|
|
|
|
|
b610 |
Urinary excretory functions |
|
|
|
|
|
|
|
|
|
|
33 |
|
b620 |
Urination functions |
|
1 |
1 |
|
|
6 |
1 |
|
|
|
34 |
|
b640 |
Sexual functions |
|
1 |
|
|
|
|
1 |
|
|
|
19 |
|
b670 |
Sensations associated with genital and reproductive functions |
|
|
|
|
20 |
|
|
|
|
|
|
|
b710 |
Mobility of joint functions |
|
1 |
|
|
14 |
|
1 |
|
|
|
|
|
b715 |
Stability of joint functions |
|
|
|
|
|
18 |
|
|
|
|
|
|
b730 |
Muscle power functions |
|
1 |
1 |
1 |
|
|
1 |
1 |
|
|
|
|
b735 |
Muscle tone functions |
|
|
1 |
|
|
|
1 |
1 |
|
|
|
|
b740 |
Muscle endurance functions |
|
|
|
1 |
|
|
|
1 |
|
|
|
|
b750 |
Motor reflex functions |
|
|
|
|
|
|
|
1 |
|
|
|
|
b755 |
Involuntary movement reaction functions |
|
|
|
|
13 |
|
|
|
|
|
|
|
b760 |
Control of voluntary movement functions |
|
|
|
|
24 |
|
|
|
|
|
|
|
b780 |
Sensations related to muscles and movement functions |
|
|
|
|
|
17 |
|
|
|
|
|
|
b810 |
Protective functions of the skin |
|
|
1 |
|
15 |
|
1 |
|
|
|
37 |
|
b840 |
Sensation related to the skin |
|
|
|
|
|
|
|
|
1 |
13 |
15 |
|
s120 |
Spinal cord and related structures |
|
|
1 |
1 |
|
|
1 |
1 |
|
|
|
|
s430 |
Structure of respiratory system |
|
|
1 |
|
|
13 |
1 |
|
|
|
|
|
s610 |
Structure of urinary system |
|
|
1 |
|
8 |
|
1 |
|
|
|
|
|
s720 |
Structure of shoulder region |
|
|
|
|
29 |
|
|
|
|
|
|
|
s810 |
Structure of areas of skin |
|
|
|
|
|
22 |
1 |
|
|
|
|
|
d155 |
Acquiring skills |
|
|
|
|
|
|
|
|
|
|
12 |
|
d230 |
Carrying out daily routine |
1 |
1 |
|
|
|
|
1 |
|
|
|
|
|
d240 |
Handling stress and other psychological demands |
|
1 |
|
|
|
9 |
1 |
|
1 |
9 |
|
|
d360 |
Using communication devices and techniques |
|
|
|
|
|
|
|
|
|
|
4 |
|
d410 |
Changing basic body position |
|
1 |
1 |
|
|
|
1 |
|
|
|
|
|
d415 |
Maintaining a body position |
|
1 |
|
|
|
|
|
|
|
|
|
|
d420 |
Transferring oneself |
|
1 |
1 |
|
|
|
1 |
|
|
|
|
|
d435 |
Moving objects with lower extremities |
|
|
|
1 |
|
|
|
|
|
|
|
|
d445 |
Hand and arm use |
|
|
1 |
|
|
|
1 |
|
1 |
16 |
16 |
|
d450 |
Walking |
1 |
1 |
1 |
|
|
|
|
|
|
|
|
|
d455 |
Moving around |
1 |
1 |
|
1 |
|
|
1 |
1 |
|
|
|
|
d460 |
Moving around in different locations |
|
|
|
1 |
|
|
|
|
|
|
|
|
d465 |
Moving around using equipment |
|
1 |
|
|
4 |
3 |
1 |
|
|
|
|
|
d470 |
Using transportation |
|
1 |
|
|
|
|
1 |
|
|
|
|
|
d475 |
Driving |
|
|
|
|
|
|
|
|
|
|
10 |
|
d510 |
Washing oneself |
|
1 |
1 |
|
|
|
|
|
|
|
|
|
d520 |
Caring for body parts |
|
1 |
|
|
|
|
1 |
|
|
|
2 |
|
d530 |
Toileting |
|
1 |
1 |
|
7 |
|
1 |
|
|
|
|
|
d540 |
Dressing |
|
1 |
1 |
|
|
|
|
|
|
|
|

|
Table I. Contd. |
||||||||||||
|
ICF Code |
Title |
ICF Generic Set |
ICF Rehabilitation Set |
Brief EPA |
90%a EPA |
Pat EPA Rankingb |
HP EPA Rankingb |
Brief LT |
90%a LT |
Pat LT |
Pat LT Rankingb |
HP LT Rankingb |
|
d550 |
Eating |
|
1 |
1 |
|
|
|
1 |
|
|
|
|
|
d560 |
Drinking |
|
|
1 |
|
|
|
|
|
|
|
|
|
d570 |
Looking after one’s health |
|
1 |
|
|
1 |
|
|
|
1 |
3 |
|
|
d620 |
Acquisition of goods and services |
|
|
|
|
|
|
|
|
1 |
1 |
|
|
d630 |
Preparing meals |
|
|
|
|
2 |
2 |
|
|
|
|
|
|
d640 |
Doing housework |
|
1 |
|
|
|
|
|
|
|
|
|
|
d660 |
Assisting others |
|
1 |
|
|
|
|
|
|
1 |
11 |
3 |
|
d710 |
Basic interpersonal interactions |
|
1 |
|
|
|
|
|
|
|
|
|
|
d770 |
Intimate relationships |
|
1 |
|
|
3 |
4 |
|
|
1 |
8 |
11 |
|
d820 |
School education |
|
|
|
|
|
|
|
|
1 |
18 |
|
|
d840 |
Apprenticeship (work preparation) |
|
|
|
|
|
|
|
|
|
|
17 |
|
d845 |
Acquiring, keeping and terminating a job |
|
|
|
|
|
|
|
|
|
|
5 |
|
d850 |
Remunerative employment |
1 |
1 |
|
|
|
|
|
|
|
|
|
|
d870 |
Economic self-sufficiency |
|
|
|
|
|
1 |
|
|
1 |
2 |
|
|
d910 |
Community life |
|
|
|
|
|
|
|
|
|
|
1 |
|
d920 |
Recreation and leisure |
|
1 |
|
|
|
|
|
|
|
|
|
|
d930 |
Religion and spirituality |
|
|
|
|
18 |
10 |
|
|
|
|
|
|
e110 |
Products or substances for personal consumption |
|
1 |
|
|
|
|
1 |
|
|
|
|
|
e115 |
Products and technology for personal use in daily living |
|
1 |
1 |
|
|
|
1 |
|
|
|
|
|
e120 |
Products and technology for personal indoor and outdoor mobility and transportation |
|
1 |
1 |
|
9 |
20 |
1 |
|
|
|
|
|
e125 |
Products and technology for communication |
|
|
|
|
26 |
|
|
|
|
|
|
|
e135 |
Products and technology for employment |
|
1 |
|
|
25 |
14 |
|
|
|
|
31 |
|
e140 |
Products and technology for culture, recreation and sport |
|
|
|
|
23 |
|
|
|
1 |
15 |
9 |
|
e150 |
Design, construction and building products and technology of buildings for public use |
|
1 |
|
|
19 |
|
1 |
|
1 |
12 |
|
|
e155 |
Design, construction and building products and technology of buildings for private use |
|
1 |
|
|
|
|
1 |
|
|
|
20 |
|
e165 |
Assets |
|
|
|
|
|
21 |
|
|
|
|
39 |
|
e225 |
Climate |
|
1 |
|
|
|
|
|
|
|
|
|
|
e310 |
Immediate family |
|
1 |
1 |
1 |
|
|
1 |
|
|
|
|
|
e320 |
Friends |
|
1 |
|
|
|
|
|
|
|
|
|
|
e325 |
Acquaintances, peers colleagues, neighbours and community members |
|
|
|
|
10 |
|
|
|
1 |
17 |
|
|
e340 |
Personal care providers and personal assistants |
|
|
1 |
|
|
8 |
1 |
|
|
|
14 |
|
e355 |
Health professionals |
|
1 |
1 |
1 |
|
|
1 |
|
|
|
|
|
e360 |
Health-related professionals |
|
|
|
|
30 |
|
|
|
|
|
30 |
|
e415 |
Individual attitudes of extended family members |
|
|
|
|
|
|
|
|
1 |
14 |
8 |
|
e420 |
Individual attitudes of friends |
|
|
|
|
|
|
|
|
|
|
36 |
|
e440 |
Individual attitudes of personal care providers and personal assistants |
|
|
|
|
|
|
|
|
1 |
19 |
|
|
e450 |
Individual attitudes of health professionals |
|
1 |
|
1 |
|
|
|
|
1 |
20 |
|
|
e455 |
Individual attitudes of health-related professionals |
|
|
|
|
|
|
|
|
|
|
25 |
|
e460 |
Societal attitudes |
|
|
|
|
|
|
|
|
|
|
28 |
|
e510 |
Services, systems and policies for the production of consumer goods |
|
|
|
|
|
|
|
|
|
|
21 |
|
e515 |
Architecture and construction services, systems and policies |
|
|
|
|
|
|
|
|
|
|
13 |

|
Table I. Contd. |
||||||||||||
|
ICF Code |
Title |
ICF Generic Set |
ICF Rehabilitation Set |
Brief EPA |
90%a EPA |
Pat EPA Rankingb |
HP EPA Rankingb |
Brief LT |
90%a LT |
Pat LT |
Pat LT Rankingb |
HP LT Rankingb |
|
e525 |
Housing services, systems and policies |
|
|
|
|
|
|
|
|
|
|
32 |
|
e530 |
Utilities services, systems and policies |
|
|
|
|
|
|
|
|
|
|
23 |
|
e540 |
Transportation services, systems and policies |
|
|
|
|
|
|
|
|
1 |
21 |
|
|
e555 |
Associations and organizational services, systems and policies |
|
|
|
|
5 |
5 |
|
|
|
|
18 |
|
e575 |
General social support services, systems and policies |
|
|
|
|
12 |
|
|
|
|
|
38 |
|
e580 |
Health services, systems and policies |
|
1 |
|
|
|
|
1 |
|
|
|
|
|
e585 |
Education and training services, systems and policies |
|
|
|
|
|
|
|
|
1 |
10 |
24 |
|
a90% refers to ICF categories, in the description of functioning of persons with SCI, for which more than 90% of people in the empirical study indicated problems. These categories were, however, not included in the Regression model for developing the statistical set due to their lack of variance. bRanking refers to the explanatory value of the ICF category; it was ranked according to the size of the regression coefficients that resulted from the Lasso regression analysis in the development of the statistical sets; the smaller the number, the higher the rank. Brief: Brief ICF Core Set; EPA: early post-acute; Pat: patients; HP: health professionals; LT: long-term. |
||||||||||||
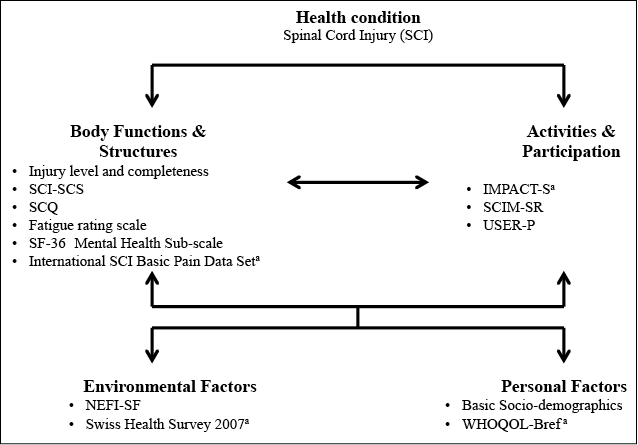
Fig. 3. Overview of components of the International Classification of Functioning, Disability and Health (ICF) and the corresponding instruments included in the Swiss Spinal Cord Injury Cohort Study (SwiSCI) community survey. SCI-SCS: SCI Secondary Conditions Scale; SCQ: Self-Administered Comorbidity Questionnaire; SF-36: 36-item Short Form; IMPACT-S: ICF Measure of Participation and Activities Questionnaire-Screener; SCIM-SR: SCI Independence Measure Self-Report; USER-P: Utrecht Scale for Evaluation Rehabilitation-Participation; NEFI-SF: Nottwil Environmental Factor Inventory Short-Form; WHOQOL-BREF: 5-item World Health Organization Quality of Life Assessment. aSelected items of the instrument are included.
To move from ICF categories to operational variables, the ICF categories were further specified based on a literature review of PubMed, recommendations for data sets by the International Spinal Cord Society (ISCoS, 21), and a platform focusing on rehabilitation evidence in SCI (22). Through this process the category specifications for, e.g. b152 Emotional functions, became anxiety and depression, and for b280 Sensation of pain, shoulder pain and pain in general (Table II, columns 1 and 2). Details of the literature search and analysis have been published previously (23).
|
Table II. International Classification of Functioning, Disability and Health (ICF) Category Specification and the pool of candidate measurement instruments found in the literature exemplified for b152 Emotional functions and b280 Sensation of pain |
||||
|
ICF category |
Specification |
Measurement instrument |
Type of measurement |
Number of items/questionsa |
|
b152 Emotional functions |
Anxiety Depression |
Hospital Anxiety and Depression Scale |
SR, OBS |
14 |
|
Centre for Epidemiological Studies Depression Scale |
SR, SSI |
20 |
||
|
Patient Health Questionnaire-9 |
SR, SSI |
9 |
||
|
Zung Self-Rating Depression Scale |
SR, SSI |
20 |
||
|
Montgomery-Asberg Depression Rating Scale |
OBS |
10 |
||
|
Hamilton Rating Scale for Depression |
SSI |
21 |
||
|
State-Trait Anxiety Inventory |
SR |
40 |
||
|
Beck Depression Inventory |
SR |
21 |
||
|
Goldberg General Health Questionnaire (Self-completion) |
SR |
28 |
||
|
Geriatric Depression Scale |
SR |
15 |
||
|
Geriatric Mental State |
SSI |
30 |
||
|
Mental Status Questionnaire |
SSI |
10 |
||
|
Mental Health Scale of the SF-36 |
SR |
5 |
||
|
b280 Sensation of pain |
Shoulder pain Pain (general) |
International Spinal Cord Injury Pain Basic Data set |
OBS, SSI |
16 |
|
International Spinal Cord Injury Pain Basic Data set (self-reported version) |
SR |
8 |
||
|
Wheelchair User’s Shoulder Pain Index |
SR |
15 |
||
|
McGill Pain Questionnaire |
SR |
20 |
||
|
McGill Pain Questionnaire - Short Form |
SR |
15 |
||
|
Classification System for Chronic Pain in SCI |
OBS, SR |
36 |
||
|
Donovan SCI Pain Classification System |
SSI |
30 |
||
|
The Multidimensional Pain Inventory - SCI version |
SR |
50 |
||
|
Quantitative Sensory Testing |
CT |
na |
||
|
Tunk’s Classification Scheme |
SSI |
various |
||
|
Brief Pain Inventory |
SR |
17 |
||
|
SCI Secondary Condition Scale |
SR |
16 |
||
|
Numeric rating scale |
SR |
na |
||
|
Visual analogue scale |
SR |
na |
||
|
aSome instruments are available in different lengths and thus number of items; the number of items of the most widely used versions are listed here. SR: self-report instrument; OBS: observational instrument; SSI: semi-structured interview; CT: clinical test; na: not applicable. |
||||
Additional variables relevant from a psychological personal perspective, such as life satisfaction, self-efficacy, and coping, have also been identified through systematic literature reviews (24).
Step 2: How to assess relevant aspects of functioning in SwiSCI. Based on the category specification for each ICF category, (sub-)scales or (items of) instruments were identified that are commonly used to assess the respective aspects of functioning. Systematic literature searches were conducted (24–27), as well as reviews of SCI-specific databases (14, 21, 22). To exemplify this process, the second part of Table II (columns 3 and 4) lists all the resulting scales and instruments for b152 Emotional functions and b280 Sensation of pain. The same process was conducted for all of the identified ICF categories.
Once the ICF categories to be translated into operational variables were specified and the linking tables of each instrument developed, issues of comparability, efficiency, non-redundancy, reliability and validity, and feasibility were considered. Table III shows the linkings of instruments identified to assess Activities and Participation. All of these instruments have shown to be reliable and valid, while accounting for the fact that some instruments have been in use for longer (e.g. Functional Independence Measure (FIM)) than others Utrecht Scale for Evaluation of Rehabilitation-Participation (USER-P). The figures at the end of the Table show that all instruments contain items linked to ICF categories identified as relevant for SwiSCI. The instruments vary, however, in terms of the number of items beyond those in the SwiSCI category set. For instance the SCIM-SR includes only 1 item outside relevant ICF categories, whereas the ICF Measure of Participation and ACTivities – Screener (IMPACT-S) contains 17 items. On the other hand, Spinal Cord Independence Measure – Self-Report (SCIM-SR) lacks items relevant to 9 ICF categories in the SwiSCI set, whereas IMPACT-S lacks only 1 item. Thus, there is no single instrument that captures all aspects of the Activities and Participation component well while not including too many additional aspects. Thus, a combination of instruments was considered for SwiSCI. As SCIM is an SCI-specific instrument widely used in clinical practice, it was considered as a very important instrument by the SwiSCI study team. However, from the point of view of feasibility, SCIM is an expert-administered instrument. To make it feasible for reliable and valid use in the SwiSCI study required the development of a self-report version (28, 29). When combining items from SCIM-SR and USER-P, all except 3 ICF categories of the SwiSCI category set, and only 5 additional ICF categories not in the category set, are covered. The 3 ICF categories not covered are: d240 Handling stress and other psychological demands, d445 Hand and arm use, and d710 Basic personal interactions. The 5 additional categories are: d360 Using communication devices and techniques, d650 Caring for household objects, d740 Formal, d750 Informal social relationships, and d810-d830 Education. The items of the 2 instruments appeared to be non-redundant. Thus, for assessing relevant aspects of functioning in people with SCI with respect to the Activity and Participation component, the SCIM-SR and USER-P were selected. To assess the ICF categories not captured by these instruments, an additional item from the IMPACT-S was chosen for d240 Handling stress and other psychological demands. With regard to d445 Hand and arm use and d710 Basic interpersonal interactions, the balance between completeness of relevant aspects to be covered and the length of the survey were considered, and it was agreed by the research team that these aspects are addressed indirectly through other items. For instance, items in SCIM-SR imply a certain ability to reach for things or to rotate the hands. This example illustrates the value of having a linking table to inform the selection of instruments and items. In addition, the rationale of selecting a specific instrument accounts for aspects beyond the content of an instrument, such as comparability and feasibility.
|
Table III. Comparison of instruments assessing relevant International Classification of Functioning, Disability and Health (ICF) categories from the component Activities and Participation |
||||||||
|
ICF Code |
ICF Label |
SwiSCI Category Set |
FIM |
SCIM-SR |
IMPACT-S |
WHODAS 2.0 |
USER-P |
SCIM-SR & USER-P |
|
d110-d129 |
Purposeful sensory experiences |
|
|
|
× |
|
|
|
|
d130-d159 |
Basic learning |
|
|
|
× |
× |
|
|
|
d160-d179 |
Applying knowledge |
|
× |
|
× |
× |
|
|
|
d210 |
Undertaking a single task |
|
|
|
× |
|
|
|
|
d230 |
Carrying out daily routine |
× |
|
|
|
× |
× |
× |
|
d240 |
Handling stress and other psychological demands |
× |
|
|
× |
|
|
|
|
d310-d329 |
Communicating - receiving |
|
× |
|
× |
× |
|
|
|
d330-d349 |
Communicating - producing |
|
× |
|
× |
× |
|
|
|
d360 |
Using communication devices and techniques |
|
|
|
× |
|
× |
× |
|
d410 |
Changing basic body position |
× |
× |
× |
× |
× |
|
× |
|
d415 |
Maintaining a body position |
× |
× |
|
||||
|
d420 |
Transferring oneself |
× |
|
|
||||
|
d430-d449 |
Carrying, moving and handling objects |
|
× |
|
× |
|
|
|
|
d445 |
Hand and arm use |
× |
|
|
× |
|
|
|
|
d450 |
Walking |
× |
× |
× |
× |
× |
|
× |
|
d455 |
Moving around |
× |
× |
× |
|
|
× |
|
|
d460 |
Moving around in different locations |
|
× |
× |
× |
|
× |
|
|
d465 |
Moving around using equipment |
× |
× |
|
|
× |
||
|
d470-d489 |
Moving around using transportation |
× |
|
|
× |
|
× |
× |
|
d510 |
Washing oneself |
× |
× |
× |
× |
× |
|
× |
|
d520 |
Caring for body parts |
× |
× |
× |
× |
|
|
× |
|
d530 |
Toileting |
× |
× |
× |
|
|
× |
|
|
d540 |
Dressing |
× |
× |
× |
× |
× |
|
× |
|
d550 |
Eating |
× |
× |
× |
× |
× |
|
× |
|
d560 |
Drinking |
× |
|
|
||||
|
d570 |
Looking after one’s health |
× |
|
× |
|
|
× |
|
|
d610-d629 |
Acquisition of necessities |
|
|
|
× |
× |
|
|
|
d640 |
Doing housework |
× |
|
|
× |
× |
× |
× |
|
d650 |
Caring for household objects |
|
|
|
× |
|
||
|
d660 |
Assisting others |
× |
|
|
× |
|
||
|
d710 |
Basic interpersonal interactions |
× |
|
|
× |
|
|
|
|
d720 |
Complex interpersonal interactions |
|
|
|
|
|
|
|
|
d730 |
Relating with strangers |
|
|
|
|
× |
|
|
|
d740 |
Formal relationships |
|
|
|
× |
|
|
|
|
d750 |
Informal social relationships |
|
|
|
× |
× |
× |
× |
|
d760 |
Family relationships |
|
|
|
|
|
× |
× |
|
d770 |
Intimate relationships |
× |
|
|
× |
× |
× |
× |
|
d810-d839 |
Education |
|
|
|
× |
× |
× |
× |
|
d840-d859 |
Work and employment |
× |
|
|
× |
× |
× |
|
|
d860-d879 |
Economic life |
|
|
|
× |
|
|
|
|
d910 |
Community life |
|
|
|
× |
× |
|
|
|
d920 |
Recreation and leisure |
× |
|
|
× |
× |
× |
× |
|
d930 |
Religion and spirituality |
|
|
|
× |
× |
|
|
|
d940 |
Human rights |
|
|
|
|
× |
|
|
|
d950 |
Political life and citizenship |
|
|
|
× |
|
|
|
|
|
ICF category in SwiSCI Category Set, item included in instrument |
|
10 |
10 |
15 |
11 |
7 |
20 |
|
|
ICF category in SwiSCI Category Set, no item included in the instrument |
|
10 |
9 |
1 |
12 |
15 |
3 |
|
|
ICF category not in SwiSCI Category Set, item included in instrument |
|
4 |
1 |
17 |
10 |
5 |
5 |
|
Some ICF categories are presented in blocks rather than at the category level in order to facilitate the comprehensiveness, yet simplicity, of the table. |
||||||||
DISCUSSION
This paper outlines the relevant steps and related methods in the development of a cohort study on functioning based on the ICF. In particular, it specifies how to go from the complex phenomena of functioning to specifying operational variables for consideration in a cohort study on functioning. The steps and methods outlined here ensure that the development of a cohort study is based on the comprehensive perspective of health, as operationalized through functioning in the WHO’s ICF, and yet is efficient and feasible to administer. Using the ICF as a foundation for the development of a cohort study on functioning ensures the operationalization of a comprehensive perspective of health in the specification of which aspects to consider in a given study. At the same time, the methods outlined here do not ignore existing instruments or common practice, but rather try to integrate them into a comprehensive frame of reference. This approach prevents researchers from selecting variables from existing instruments or common practice because of convenience, and ensures comparability with existing clinical and research practice.
Some further points are relevant to the selection of an instrument. First, although instruments may link to the same ICF category, they may adopt different perspectives; for example, one can ask about difficulties in getting dressed, a person’s satisfaction with his or her ability to get dressed, or the assistive devices needed for getting dressed. Secondly, instruments and assessment tools may use various approaches to quantify the responses to an item; for example, in terms of the intensity of problems in getting dressed or the frequency of personal assistance needed. The perspectives adopted in existing instruments and the approaches used for quantifying the information are all legitimate and valuable, of course, but for comparability of data it is important to clarify not only whether 2 items link to the same ICF category, but also from which perspective questions about the information are asked and how the information becomes quantified.
The challenge of setting up a cohort study on functioning comes with creating a parsimonious set of categories and related items which, at the same time, is expected to encompass a broad range of ICF categories across all components relevant to human functioning. The ICF Core Sets serve as a starting point to identify those aspects of functioning considered to be most relevant to report and assess. Complementary to that, international scientific communities, such as the International Spinal Cord Society (ISCoS), recommend techniques for assessing some of these ICF categories. For example, ISCoS has proposed standard variables for SCI data sets in order to foster the integration of clinical and research data. Data sets have been developed for specific domains, such as pain, bowel function, urodynamic, and cardiovascular function (21). Each of these data sets contains further questions, as, for example, for the domain pain: severity and frequency of pain, pain location, and quality of pain. In developing a cohort study such as SwiSCI, which captures relevant aspects of functioning across all components of the ICF, it is important to ensure comparability with these existing sets by identifying a succinct standard variable set, while trying to facilitate the development of specific modules or nested projects that enable study of a phenomenon or domain in greater depth. Such an approach makes it possible to establish a comprehensive survey, aligned with international standards and recommendations from relevant international communities, which can also be feasibly administered.
The steps in the development of the data items for SwiSCI answer the call of both the World Report on Disability (30) and the International Perspectives on Spinal Cord Injury (31), for strengthening comparable data. Using the ICF as a foundation to specify what is important to consider, and being transparent in the methods to specify the relevant categories and their translation into operational variables is highly valuable, as it enables the establishment of qualitative and quantitative comparability with any other study. Having the ICF categories of the ICF Generic and Rehabilitation Sets included in the variable set facilitates comparability across health conditions and across settings in the future. These ICF categories can be seen as the minimum standard most relevant for comparability of functioning information across clinical (sub-)populations, across settings along the continuum of care, and across countries.
In conclusion, we have outlined the conceptual and methodological framework for setting up a cohort study on functioning that is also designed to assist comparability with data from existing data sets. The specific steps toward specifying what to assess in rehabilitation practice and research, and how to assess the specified domains are described using SwiSCI as an example. The approach outlined in this paper facilitates bridging classification with existing approaches and methods of assessment. As such, it facilitates, on the one hand, standardized reporting and, on the other hand, comparability with existing clinical practice and research.
ACKNOWLEDGEMENTS
This study has been financed in the framework of the Swiss Spinal Cord Injury Cohort Study (SwiSCI, www.swisci.ch), supported by the Swiss Paraplegic Research.
The members of the SwiSCI Steering Committee are: Xavier Jordan, Bertrand Léger (Clinique Romande de Réadaptation, Sion); Michael Baumberger, Hans Peter Gmünder (Swiss Paraplegic Center, Nottwil); Armin Curt, Martin Schubert (University Clinic Balgrist, Zürich); Margret Hund-Georgiadis, Kerstin Hug (REHAB Basel, Basel); Hans Georg Koch, (Swiss Paraplegic Association, Nottwil); Hardy Landolt (Representative of persons with SCI, Glarus); Hansjörg Koch (SUVA, Luzern); Mirjam Brach, Gerold Stucki (Swiss Paraplegic Research, Nottwil); Martin Brinkhof, Christine Thyrian (SwiSCI Study Center at Swiss Paraplegic Research, Nottwil).
REFERENCES

