Eva A. Jaarsma, MSc, PhD1, Rienk Dekker, MD, PhD1,2, Jan H. B. Geertzen, MD, PhD1 and Pieter U. Dijkstra, PT, PhD1,3
From the 1Department of Rehabilitation Medicine, Center for Rehabilitation, 2Center of Sports Medicine and 3Department of Oral and Maxillofacial Surgery, University of Groningen, University Medical Center Groningen, Groningen, The Netherlands
OBJECTIVE: To analyse barriers to, and facilitators of, sports participation among people with physical disabilities after rehabilitation and to compare differences between inactive and active participants regarding these experienced barriers and facilitators.
METHODS: Participants were 1,223 adults (mean age 51.6 years, standard deviation 15.1 years) treated in the Rehabilitation Centre of the University Medical Center Groningen, who completed a questionnaire. The questionnaire consisted of a self-constructed questionnaire regarding barriers and facilitators.
RESULTS: Fifty-eight percent of the participants were active in sports after their rehabilitation. Younger age and a higher level of education were positively associated with sports participation, whereas using assistive devices and experiencing environmental barriers were negatively associated. Facilitators of sports participation were health, fun and increasing physical strength, and advice from rehabilitation professionals.
CONCLUSION: Rehabilitation professionals should emphasize the health benefits of, and enjoyment from, sports participation for people with physical disabilities. They should repeatedly remind people with physical disabilities to stay/become active after completing their rehabilitation programme. Rehabilitation professionals should also provide information about strategies to reduce environmental barriers to sports participation, which could help people using assistive devices to overcome these barriers.
Key words: disabled persons; sports; rehabilitation.
J Rehabil Med 2015; 00: 00–00
Correspondence address: Eva A. Jaarsma, Department of Rehabilitation Medicine, Center for Rehabilitation, University of Groningen, University Medical Center Groningen, Hanzeplein 1, CB41, PO Box 30.0001, NL-9700 RB, Groningen, The Netherlands. E-mail: e.a.jaarsma@umcg.nl
Accepted Jul 31, 2015; Epub ahead of print Nov 4, 2015
INTRODUCTION
On average, only one-third of people with physical disabilities regularly participate in sports, compared with two-thirds of people without physical disabilities (1, 2). Previous research has demonstrated that not participating in sports could increase the risk of secondary health conditions such as heart disease, type 2 diabetes and obesity (1, 3). Even though sports are often part of rehabilitation programmes in the Netherlands, only a few people with physical disabilities remain active in sports after completing their rehabilitation programme (4). To understand why the majority of people with physical disabilities do not participate in sports, it is important to know what prevents them doing so, and how they could be facilitated and motivated to become active in sports. A recent systematic review on barriers to, and facilitators of, sports participation demonstrated that people with physical disabilities often experience barriers such as (disability-related) health problems, lack of energy or fatigue that prevent them from participating in sports (5). Difficulties with sports accommodation, transport and costs were also reported as barriers to sports participation (5). Frequently reported facilitators of sports participation for people with and without physical disabilities were health, fun and social contact (5–14).
Several models or theories can be used to study why people with physical disabilities decide to participate (or not participate) in sports. Two models that have been used frequently in previous research are the International Classification of Functioning, Disability and Health (ICF) of the World Health Organization and the theory of planned behaviour (TPB) (9, 12, 15–17). The ICF is a classification of health domains from body, personal and environmental perspectives. Focusing on the personal perspective, a health condition can be divided into 3 sections: “Body structure and functions”, “Activity” and “Participation” (18). This study will focus on the “Participation” component of the ICF, which also includes sports participation (18). Regarding (sports) participation, the ICF distinguishes personal and environmental factors.
The TPB, proposed by Ajzen (19), combines the components Attitude, Subjective Norm and Perceived Behavioural Control to determine intention, which, in turn, could lead to behaviour (Fig. 1). Attitude is a person’s positive or negative expectancy towards behaviour. Subjective norm refers to the social pressure regarding behaviour. Perceived behavioural control is the belief that a person can control his or her own behaviour in certain situations (19). Both frameworks are often used in research into sports participation. They can help in determining important factors related to sports participation in people with physical disabilities and in structuring the research results (9, 17, 20, 21).
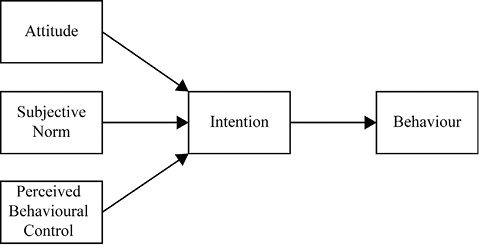
Fig. 1. Theory of Planned Behaviour (19).
Most studies focusing on barriers to, and facilitators of, sports participation among people with physical disabilities have included either active or inactive participants (13, 22–26). Focusing on a single group does not allow direct comparison of differences in barriers and facilitators between active and inactive participants. Knowledge of these differences could help rehabilitation professionals in providing a more thoroughly founded advice for sports participation depending on the activity level of the person with a physical disability.
Studies often also do not distinguish between physical disabilities, and thus do not show whether differences exist in barriers and facilitators of sports between different physical disabilities (9, 12, 27, 28).
The aim of this study is therefore to analyse which barriers and facilitators influence sports participation among people with different physical disabilities. We also compared inactive and active participants regarding their experienced barriers and facilitators of sports participation. Finally, we determined which variables were significantly associated with sports participation.
METHODS
Participants
Participants in this study were all people with a physical disability, aged 18 years or older, who had been treated in the Rehabilitation Centre of the University Medical Center Groningen, the Netherlands between 1 January 2009 and 31 December 2011. These participants also included people with chronic pain, defined according to the Classification of Chronic Pain of the International Association for the Study of Pain (29). Excluded were patients with a diagnosis of orthopaedic origin (e.g. anterior cruciate ligament injury and total hip or knee replacement) and patients receiving cardiac or pulmonary rehabilitation. A total of 3,169 (ex-)patients were invited to complete the questionnaire.
Questionnaire
The questionnaire (36 items) (Appendix SI1) used in this study was a self-constructed questionnaire on barriers and facilitators of Paralympic athletes, published elsewhere (6). The self-constructed questionnaire on barriers and facilitators was used, because no questionnaire is available specifically focusing on both barriers and facilitators of sports participation. Items from the questionnaire on barriers and facilitators in Paralympic athletes were modified to make them relevant for people with physical disabilities. Therefore items about mental training and nutrition in the original Paralympic questionnaire were excluded. A definition of sports participation was included for this study, namely “an activity involving physical exertion with or without a game or competition element with a minimal duration of 30 min for at least two times a week where skills and physical endurance are either required or to be improved” (4, 8, 30). To be able to compare sports participation among the participants, we only focused on sports. We excluded the broader term physical activity because it has various definitions, from household chores to moderate intensity activity (31). All items about barriers and facilitators were divided into personal and environmental factors according to the ICF. Items about physical disability and sports participation were grouped according to the components of the TPB. The complete methodology of the Paralympic questionnaire has been published elsewhere (6).
Procedure
In the envelope sent to the subjects, a cover letter was included that explained the purpose and methodology of the study. The letter also ensured all data would be processed anonymously and participation was voluntary. An informed consent form was included for participants to sign. Subjects were invited to either complete the paper questionnaire included in the envelope or to use the provided link to complete the questionnaire online. Both paper and online versions of the questionnaire were included in this study, to also allow participants without a computer to participate in the study. The study was approved by the medical ethics committee of the Universal Medical Centre Groningen, the Netherlands (METc 2012.450).
Data collection and analysis
The patients’ names, addresses, disability, sex, date of birth and date of last treatment of the research population were retrieved from the database of the Rehabilitation Center of the University Medical Center Groningen, the Netherlands.
Participants who completed the questionnaire were divided into inactive (less than 2 × 30 min a week) and active (at least 2×30 min/week) participants, based on their answer on the sports question (Appendix I, question 12). χ2 tests were used to analyse differences in barriers and facilitators as well as experienced environmental barriers between inactive and active participants. A Mann-Whitney U test was used to analyse differences between inactive and active participants in follow-up time (i.e. time between last date of treatment and date of distribution of the questionnaire). A Bonferroni correction was applied for post-hoc tests. To determine which variables were associated with sports participation a binary logistic regression (Enter method) was used, which included all variables associated with sports participation (p ≤ 0.1). The alpha level for statistical significance was set at 0.05 for all tests in this study, except post-hoc tests.
RESULTS
A total of 3,169 people were invited to participate in this study, with a mean age of 51.6 years (standard deviation (SD) 15.1) and 49% were male. A total of 1,223 participants (39%) completed the questionnaire. The mean age of participants was 53.4 years (SD 14.5) and 50% were male (Table I). Participants were significantly older than non-participants t (2,465.207) = 5.125, p < 0.001. There were no significant differences in gender between participants and non-participants. Participants and non-participants did not differ significantly in time between the date of last treatment and the date of receiving the questionnaire (1 March 2013) (median 27 months, interquartile range (IQR) 20–37; and median 29 months, IQR 20–39, respectively).
|
Table I. Characteristics of all participants and inactive and active participants separately |
||||
|
Total (n = 1,223) |
Inactive (n = 509) |
Active (n = 714) |
||
|
Age*, years, mean (SD) |
53.4 (14.5) |
55.8 (14.7) |
51.6 (14.0) |
|
|
Follow-up, months, median [IQR] |
27 [20–37] |
27 [19–38] |
27 [20–37] |
|
|
Gender, n (%) |
||||
|
Men |
609 (50) |
264 (52) |
345 (49) |
|
|
Diagnosis groupa,*, n (%) |
||||
|
Amputation |
49 (4) |
28 (5) |
21 (3) |
|
|
Brain injuryb |
418 (34) |
180 (35) |
238 (33) |
|
|
Chronic pain |
334 (27) |
112 (22) |
222 (31) |
|
|
Multiple sclerosis |
73 (6) |
44 (9) |
29 (4) |
|
|
Spinal cord injury |
98 (8) |
44 (9) |
54 (8) |
|
|
Other neurological disabilityc |
99 (8) |
49 (10) |
50 (7) |
|
|
Otherd |
152 (12) |
52 (10) |
100 (14) |
|
|
Education*, n (%) |
||||
|
Lower education |
796 (65) |
366 (72) |
430 (60) |
|
|
Higher education |
428 (35) |
144 (28) |
284 (40) |
|
|
Living arrangements*, n (%) |
||||
|
Independent, alone |
200 (17) |
73 (14) |
127 (18) |
|
|
Independent, with spouse and/or children |
817 (67) |
317 (63) |
500 (71) |
|
|
Independent, with home care |
115 (10) |
72 (14) |
43 (6) |
|
|
Othere |
81 (7) |
43 (9) |
38 (5) |
|
|
Monthly net household income, n (%) |
||||
|
Lower income |
445 (36) |
226 (44)* |
219 (31)* |
|
|
Higher income |
549 (45) |
191 (38)* |
358 (50)* |
|
|
Rather not say |
229 (19) |
92 (18) |
137 (19) |
|
|
Assistive devices$, n (%) |
||||
|
Use of assistive devices* (Yes) |
477 (39) |
265 (52) |
212 (3) |
|
|
Prosthetics/orthotics |
35 (3) |
14 (3) |
21 (3) |
|
|
Wheelchair/mobility scooterf |
80 (7) |
48 (9)* |
32 (5)* |
|
|
Wheeled walker/ crutches/canef |
254 (21) |
137 (27)* |
117 (16)* |
|
|
Otherg |
92 (8) |
44 (9) |
48 (7) |
|
|
$Multiple answers were possible. aDiagnosis groups are according to those of the Paralympic Movement (where “disability group” is used instead of “diagnosis group”). bBrain injury include brain injuries from vascular, traumatic or oncological origin and meningitis. cOther neurological diseases include cerebral palsy, spina bifida, Parkinson’s disease, Guillain-Barré syndrome and cauda equina syndrome. dOther diseases include disabilities such as tumours, fibromyalgia, arthritis, multiple trauma and chronic fatigue syndrome. eOther living arrangements are living at home (with parents or a guardian), sheltered housing or elderly person’s home. fBonferroni correction α/4 = 0.0125. gOther assistive devices include devices such as a stair-lift, white cane, toilet with handles or shower chair. *Significant differences between inactive and active participants (p < 0.01). SD: standard deviation; IQR: interquartile range. |
||||
Fifty-eight percent of the participants participated in sports. The distribution of inactive and active participants differed between diagnosis groups (χ2 = 31.807, df = 1, p < 0.001). More active participants were found for chronic pain (67%), brain injury (57%) and spinal cord injury (SCI) (55%), whereas more inactive participants were found for multiple sclerosis (MS) (60%) and amputation (57%). Living arrangements (χ2 = 29.913, df = 1, p < 0.001) differed significantly between inactive and active participants; more active participants lived independently, either alone (64%) or with family (61%). More active participants also had a higher level of education (χ2 = 17.424, df = 1, p < 0.001), and higher monthly net household income (χ2 = 25.454, df = 1, p < 0.001) compared with inactive participants. Inactive participants used assistive devices more often than active participants (χ2 = 63.081, df = 1, p < 0.001), especially wheelchairs (χ2 = 20.454, df = 1, p < 0.001; α/4 = 0.0125) and/or wheeled walkers (χ2 = 57.709, df = 1, p < 0.001; α/4 = 0.0125). Cycling (60%), walking (59%) and fitness (36%) were most frequently performed sports (Table II).
|
Table II. Sports performed by active participants (n = 714) |
|
|
Sportsa |
n (%) |
|
Cycling |
431 (60.4) |
|
Walking |
425 (59.4) |
|
Fitness (including physio fitness) |
256 (35.9) |
|
Swimming |
133 (18.6) |
|
Endurance training |
98 (13.7) |
|
Running |
29 (4.1) |
|
Yoga |
28 (3.9) |
|
Zumba or equivalent |
26 (3.6) |
|
Gymnastics |
20 (2.8) |
|
Dancing |
18 (2.5) |
|
Spinning |
16 (2.2) |
|
Aqua gym or aqua jogging |
15 (2.1) |
|
Golf |
13 (1.8) |
|
Rowing |
11 (1.5) |
|
Football (soccer) |
10 (1.4) |
|
(Ice) skating |
10 (1.4) |
|
Tennis |
9 (1.3) |
|
Equestrian |
8 (1.1) |
|
Skiing |
8 (1.1) |
|
Sailing |
7 (1.0) |
|
Athletics |
6 (0.8) |
|
Basketball |
5 (0.7) |
|
Shooting |
5 (0.7) |
|
Martial arts |
4 (0.6) |
|
Body pump |
4 (0.6) |
|
Aerobics |
3 (0.4) |
|
Climbing |
2 (0.3) |
|
Judo |
2 (0.3) |
|
Table tennis |
2 (0.3) |
|
Other |
109 (15.3) |
|
aMultiple answers were possible. |
|
Barriers
Inactive participants reported their disability (53%) (χ2 = 7.472, df = 1, p = 0.006) and fatigue (42%, Table III) (χ2 = 8.719, df = 1, p = 0.003) more often as personal barriers than did active participants (45% and 33%, respectively). Inactive participants also reported dependency on others (10%) more often than did active participants (6%; χ2 = 6.049, df = 1, p = 0.014). Active participants reported pain (7%) as a personal barrier more often than did inactive participants (2%) (χ2 = 14.269, df = 1, p < 0.001). Inactive participants more often reported costs (12%) (χ2 = 4.989, df = 1, p = 0.02) and lack of a sports buddy (5%) (χ2 = 9.479, df = 1, p = 0.002) as environmental barriers than did active participants (8% and 2%, respectively). Overall, more inactive participants (44%) experienced at least 1 environmental barrier compared with active participants (30%; χ2 = 26.996, df = 1, p < 0.001).
|
Table III. Barriers to sports participation according to inactive and active participants |
||
|
Barriers |
Inactive (n=509) |
Active (n=714) |
|
Personal factorsa, n (%) |
||
|
Disability |
268 (53)** |
318 (45)** |
|
Fatigue/ lack of energy |
213 (42)** |
234 (33)** |
|
Dependency of others |
49 (10)* |
42 (6)* |
|
Injuries |
49 (10) |
76 (11) |
|
Takes too much time/too busy with other activities |
49 (10) |
61 (9) |
|
Participant does not like sports |
32 (6) |
– |
|
Uncomfortable among others |
27 (5) |
42 (6) |
|
Ashamed of disability |
22 (4) |
– |
|
Pain |
11 (2)*** |
49 (7)*** |
|
Other |
– |
60 (8) |
|
Environmental factorsa, n (%) |
|
|
|
Costs |
62 (12)* |
59 (8)* |
|
No fitting sport |
43 (9) |
46 (6) |
|
Lack of a sports buddy |
24 (5)** |
12 (2)** |
|
Lack of information about sports facilities |
19 (4) |
30 (4) |
|
Lack of sufficient transport facilities |
19 (4) |
19 (3) |
|
Lack of sports facilities in the neighbourhood |
18 (4) |
33 (5) |
|
Lack of acceptance of other people |
17 (3) |
13 (2) |
|
Lack of (sufficient) supervision |
15 (3)** |
35 (5)** |
|
Lack of support/help from environment |
15 (3) |
11 (2) |
|
Courses are not (sufficiently) adjusted |
10 (2) |
22 (3) |
|
Equipment is not (sufficiently) adjusted/available |
10 (2) |
9 (1) |
|
Accommodation is not (sufficiently) adjusted |
8 (2) |
22 (3) |
|
Lack of possibilities to sport with peers |
4 (1) |
13 (2) |
|
Other |
42 (8) |
44 (6) |
|
No barriers |
– – |
136 (19) |
|
aMultiple answers were possible. *Significant differences between inactive and active participants (p < 0.05). **Significant differences between inactive and active participants (p < 0.01). ***Significant differences between inactive and active participants (p < 0.001). |
||
Facilitators
Health (88%), fun (63%) and increasing physical strength (50%) were the most important personal facilitators of sports participation for active participants. The most important environmental facilitators for active participants were advice from rehabilitation professionals (39%) and support from family (30%, Table IV).
|
Table IV. Facilitators of sports experienced by active participants |
|
|
Facilitators |
Active (n = 714) |
|
Personal factorsa, n (%) |
|
|
Health |
629 (88) |
|
Fun |
451 (63) |
|
Getting stronger |
355 (50) |
|
Social contacts |
249 (35) |
|
Coping with disability |
190 (27) |
|
Lose weight |
192 (27) |
|
Increase self-confidence |
126 (18) |
|
Acceptance of disability |
114 (16) |
|
Release energy |
93 (13) |
|
Gain independence |
99 (14) |
|
Winning/competition |
47 (7) |
|
Learning a new skill |
32 (5) |
|
Other |
53 (7) |
|
Environmental factorsa, n (%) |
|
|
Advice from rehabilitation professional |
279 (39) |
|
Support from family, spouse and/or children |
217 (30) |
|
Support from friends, colleagues and/or peers |
105 (15) |
|
Other |
45 (6) |
|
aMultiple answers were possible. |
|
Multivariate analysis
Gender, age, education, living arrangements, use of assistive devices, diagnosis group, costs, dependency on others, disability (experienced as a barrier), experiencing environmental barriers, lack of energy, lack of a sports buddy, lack of supervision and pain were entered as predictors of sports participation in a logistic regression (Table V). Dummy variables were created to enter the different diagnoses as categorical variables, with amputation as reference category. Younger age and higher level of education were positively associated with sports participation, whereas use of assistive devices and experiencing environmental barriers were negatively associated. Lack of supervision and pain were also positively associated with sports participation. Diagnoses did not have significant influence on the prediction of sports participation. The overall correct prediction of sports participation was 65%.
|
Table V. Variables associated with sports participation that were included in the logistic regression |
|||
|
Coefficient (SE) |
p-value |
OR (95% CI) |
|
|
Characteristicsa |
|||
|
Age (centred at 50 years) |
–0.02 (0.005) |
0.001 |
0.98 (0.98: 0.99) |
|
Educationc |
0.40 (0.14) |
0.004 |
1.50 (1.13: 1.97) |
|
Genderc |
–0.002 (0.14) |
0.99 |
1.00 (0.77: 1.30) |
|
Living arrangements |
0.03 (0.08) |
0.72 |
1.03 (0.88: 1.21) |
|
Use of assistive devicesc |
–0.82 (0.17) |
< 0.001 |
0.44 (0.32: 0.61) |
|
Diagnosis groupb, c |
|||
|
Amputation |
0.23 |
||
|
Brain injury |
0.21 (0.30) |
0.49 |
1.23 (0.68: 2.24) |
|
Chronic pain |
–0.59 (0.34) |
0.08 |
0.56 (0.29: 1.07) |
|
Multiple sclerosis |
–0.14 (0.22) |
0.53 |
0.87 (0.56: 1.34) |
|
Spinal cord injury |
–0.22 (0.40) |
0.59 |
0.81 (0.37: 1.77) |
|
Other neurological disability |
–0.37 (0.27) |
0.11 |
0.69 (0.43: 1.09) |
|
Other |
–0.29 (0.30) |
0.33 |
0.75 (0.42: 1.33) |
|
Barriersd |
|||
|
Costs |
0.06 (0.24) |
0.80 |
1.06 (0.66: 1.71) |
|
Dependency of others |
0.08 (0.27) |
0.77 |
1.08 (0.64: 1.83) |
|
Disability (experienced as barrier) |
–0.09 (0.14) |
0.53 |
0.92 (0.69: 1.21) |
|
Experiencing environmental barriers |
–0.66 (0.17) |
< 0.001 |
0.52 (0.38: 0.72) |
|
Fatigue/lack of energy |
–0.20 (0.14) |
0.14 |
0.82 (0.62: 1.07) |
|
Lack of sports buddy |
–0.62 (0.41) |
0.13 |
0.54 (0.24: 1.21) |
|
Lack of (sufficient) supervision |
1.24 (0.37) |
0.001 |
3.44 (1.67: 7.11) |
|
Pain (experienced as barrier) |
1.40 (0.41) |
0.001 |
4.06 (1.83: 9.03) |
|
Constant |
0.95 (0.33) |
0.003 |
2.60 |
|
aOverall prediction of sports participation in 65%. bCategorical variables. cReferences categories: gender: female; education: lower; use of assistive devices: no; diagnosis group: amputation. dQuoted = 1, non-quoted = 0. SE: standard error; OR: odds ratio; 95% CI: 95% confidence interval. |
|||
DISCUSSION
A total of 58% of people were engaged in sports after rehabilitation. Inactive and active participants differed in characteristics as well as experienced barriers. Active participants were more often people with chronic pain, brain injury or SCI; they more frequently lived independently and had higher education and income. They were also younger and more mobile, as the majority of active participants did not use any assistive devices. Inactive participants more often experienced their disability, dependency on others, lack of energy, costs and lack of a sports buddy as barriers to sports participation. Most frequently reported facilitators were health, fun and getting stronger, and advice from rehabilitation professionals.
Factors influencing sports participation according to the ICF: Personal and environmental factors
Multivariate analysis. Multivariate analysis showed that a younger age and higher level of education were positively associated with sports participation. Previous studies reported mixed results of the influence of age on sports participation among people with physical disabilities. Some studies did not report differences in age between inactive and active participants (8, 32, 33). However, other studies, including a study focusing on people with physical disabilities in an outpatient rehabilitation programme reported that being younger was positively associated with sports participation (25, 34–36).
The positive association of education on sports participation could indicate that these people have more experience in coping with barriers. People with higher education (high-school or more) might have learned more skills in terms of coping with problems, or are more ready to become active in sports, despite possible barriers. These results have also been shown in previous studies in people with physical disabilities including visual impairments and arthritis (25, 32, 37) where active people reported less barriers.
Using assistive devices, such as a wheelchair or crutches, and experiencing (environmental) barriers to sports participation were negatively associated with sports participation. Previous research has demonstrated that athletes who use a wheelchair in daily living experience more barriers to sports participation than ambulant athletes (6). Sports facilities and equipment might not be sufficiently adapted or accessible for people with physical disabilities using assistive devices (12, 38–40). People who need assistive devices therefore have more barriers to overcome in order to participate in sports. However, having to use assistive devices is generally related to the type and severity of the disability of the patient. Perhaps the barrier is not necessarily the use of an assistive device, but refers to the severity of the underlying disability that necessitates the patient to use an assistive device. An athlete using a wheelchair will have more barriers to overcome in order to participate in sports than an athlete without assistive devices.
Both “lack of supervision” and “pain” were significantly and positively related to sports participation. Both barriers were mentioned more often by active than by inactive participants. According to the results from the logistic regression this would imply that experiencing pain or lack of supervision increases the chances of participating in sports. These results are counterintuitive and may be caused by the question itself. Inactive participants might not consider lack of supervision or pain as barriers when they have not participated in sports before. Without prior experience of sports, inactive participants cannot know what the effect of poor supervision or pain will be on their sports participation. These variables should therefore be interpreted with care.
The multivariate analysis did not demonstrate differences in diagnosis groups, which makes younger age, higher education, not using assistive devices and not experiencing environmental barriers applicable for all diagnosis groups. Unfortunately, age and education are fixed and unchangeable. Increasing the patient’s mobility and independence by using assistive devices when needed is already part of the rehabilitation programme. Using an assistive device is generally related to the disability of the patient, and their use cannot be reduced because they are necessary for function in daily living.
Rehabilitation professionals, however, could inform patients about environmental barriers to sports participation that they might encounter in order to help provide strategies to overcome these barriers. Information about availability of (adapted) transport, accessibility of sports clubs and/or equipment can help patients in decreasing possible environmental barriers. The final model correctly predicted 65% of sports participation for people with physical disabilities. Rehabilitation professionals should therefore also pay attention to individually experienced barriers to sports participation, in order to cover the remaining 35% that could not be predicted in the model.
Facilitators
Health, fun and improving physical strength were facilitators that were also frequently reported in previous studies (8–10, 12–14, 28, 41). Participants in our study reported similar facilitators of sports participation compared with other people with or without physical disabilities.
An interesting result of this study was that advice from a rehabilitation professional was the most frequently reported environmental facilitator. Previous research has often reported support from family to be the main environmental facilitator for sports participation (11, 42). However, several studies have also emphasized the importance of medical advice and support from rehabilitation professionals as a facilitator of sports participation (8, 12). Perhaps rehabilitation professionals in our Rehabilitation Centre pay extra attention to sports participation, which could explain why it is the most frequently reported environmental facilitator in this study. Rehabilitation professionals may also regularly remind their patients of the physical and psychosocial benefits of sports participation and advise patients to also stay active after they have completed their rehabilitation programme. The advice also seems to be successful in the long run, as there were no differences between inactive and active participants in the follow-up time between the last treatment date and the questionnaire. The beneficial effects of advice from rehabilitation professionals demonstrated the importance of continuing to provide appropriate advice about sports participation for people with physical disabilities. In 2011 our Rehabilitation Centre started a special sports office for patients with physical disabilities, with consultant time to provide advice about sports participation. This sports office may help to increase even further the percentage of people with physical disabilities who are active after their rehabilitation programme, as the sports office was not yet available for participants in our study at the time of their rehabilitation.
Fifty-eight percent of participants were active in sports after their rehabilitation. Previous research reported percentages of sports participation ranging from 32% to 60% for people with physical disabilities (8, 32–34). This shows that participants from our Rehabilitation Centre are among the most active people with physical disabilities, with similar percentages of sports participation to that of people without physical disabilities (1).
Factors influencing sports participation according to the theory of planned behaviour
The attitude of the person with the physical disability is very important for intention to participate in sports (6, 17, 37). Active participants reported health, fun and improving physical strength as the most important facilitators for sports participation. Even though active participants also reported their disability as a barrier, this barrier did not outweigh the experienced facilitators and kept them motivated to remain active in sports. Providing information about health benefits and interesting activities could help in developing a more positive attitude of inactive people towards sports participation.
Subjective norm also seems important for successful participation in sports for people with physical disabilities. Besides support from family and friends, advice from rehabilitation professionals can also positively influence a person’s intention to start participating in sports. Increased encouragement from family, friends or rehabilitation professionals towards sports participation (e.g. by providing information or serving as a sports buddy) could again help in improving a person’s intention to engage in sports.
Perceived behavioural control could negatively influence the intention of participating in sports among inactive participants, because they experience more environmental barriers than active participants, which could result in them having more difficulty overcoming these barriers. Providing information about strategies to reduce environmental barriers to sports participation could help people with physical disabilities in overcoming these barriers.
Strengths and weaknesses
Both inactive and active participants from different diagnosis groups were included in the study, allowing experienced barriers and facilitators of sports participation to be directly compared among both inactive and active participants. Including different diagnosis groups also provided more insight about possible differences in barriers and facilitators of sports participation between diagnosis groups. The fact that no differences were found between diagnosis groups allows rehabilitation professionals to include general measures in sports advice that are applicable to all diagnosis groups. Participants also included people with acquired and congenital physical disabilities. Sports history might be an important facilitator of sports participation; however, this is only relevant for people with acquired physical disability. We therefore decided not to include this factor as a possible facilitator and only to report barriers and facilitators of current sports participation.
Because we had a very heterogeneous population with both congenital and acquired disabilities, we decided to focus only on barriers and facilitators experienced in their current sports.
Both paper and online survey methodologies were used in order to allow every person within the population to be able to complete the questionnaire. Taking the mean age of the approached population into consideration, not all former patients might be familiar with an online survey. We therefore provided both a paper and an online survey for participants to complete.
We decided to only include sports in this study and not the broader term physical activity. For inactive people with physical disabilities engaging in physical activity could also be beneficial in improving their physical and psychosocial well-being. Future research could therefore consider focusing on barriers and facilitators of physical activity for inactive or sedentary persons with physical disabilities, as this group could benefit from any type of (physical) activity and have a more active lifestyle.
In this study we focused on determining personal and environmental factors of sports participation. We therefore divided all experienced barriers and facilitators into personal and environmental factors. According to the ICF model disability and pain should be placed under health condition and body functions, respectively. However, as we focused on personal and environmental factors, we categorized all barriers and facilitators including disability and pain under these components.
Implications
Based on the results of this study the following considerations should be kept in mind:
• Persons with a physical disability need to have a more positive attitude towards sports participation and have to be (internally) motivated to become active.
• Rehabilitation professionals should emphasize the health and psychosocial benefits of sports participation.
• Rehabilitation professionals should provide information about strategies to overcome barriers and about local sports possibilities.
• Positive environment, such as support from family and friends, is essential to provide a motivated sports climate.
Conclusion
After rehabilitation 58% of people in this study were engaged in sports. A younger age and higher level of education were positively associated with sports participation in people with physical disabilities, whereas using assistive devices and experiencing environmental barriers were negatively associated. Facilitators of sports participation were health, fun and increasing physical strength, and advice from rehabilitation professionals. Based on these results rehabilitation professionals should focus on health and psychosocial benefits of sports participation for people with physical disabilities. Rehabilitation professionals should provide information about strategies to overcome environmental barriers of sports participation that patients using assistive devices might encounter.
ACKNOWLEDGEMENTS
The authors would like to thank A. Dijkstra, Q. Kroese and M. Linders for their help with data entry of the collected data. The authors would also like to thank W. de Jong for retrieving relevant data of the research population from the database of the Rehabilitation Centre of the University Medical Center Groningen, the Netherlands.

1http://www.medicaljournals.se/jrm/content/?doi=10.2340/16501977-2017
REFERENCES


