Lauren DeMeyer, DPT1, Marcie Brown, DPT1 and Ashley Adams, BA2
From the 1Rehabilitation Hospital, New Hanover Regional Medical Center and 2Southeast Area Health Education Center, Wilmington, NC, USA
OBJECTIVE: To investigate the effect of night positioning on ankle motion in patients after stroke or brain injury.
DESIGN: Prospective randomized controlled pilot study with 3 groups: bivalve cast; pressure-relieving ankle–foot orthosis; and control.
SUBJECTS/PATIENTS: Adults (n = 46) in inpatient rehabilitation with lower extremity paresis following stroke or brain injury.
METHODS: Intervention group participants wore a custom bivalve cast or pre-fabricated orthosis 8–12 h/night. The primary outcome variable was passive ankle dorsiflexion. Muscle spasticity (Modified Ashworth Scale) and functional mobility (Functional Independence Measure) were also assessed.
RESULTS: No significant differences were found between groups for all outcome measures at the pilot sample size (p > 0.05). Control and pressure-relieving ankle–foot orthosis groups showed improvement in ankle dorsiflexion, and the bivalve cast group demonstrated a trend toward decreased spasticity. Positioning interventions were tolerated for approximately 11 h/night. Baseline range of motion was measured and a retrospective power analysis determined that a sample size of 234 is needed for 80% power to establish significance.
CONCLUSION: Future research with a larger sample size is recommended to determine significance and whether a more specific subset of patients would benefit from night positioning to maximize treatment time during daytime therapy sessions.
Key words: stroke; brain injuries; ankle; range of motion; muscle spasticity.
J Rehabil Med 2015; 47: 873–877
Correspondence address: Lauren DeMeyer, Rehabilitation Hospital, New Hanover Regional Medical Center, 2131 S. 17th Street, Wilmington, NC 28401, USA. E-mail: lauren.demeyer@nhrmc.org
Accepted Jun 22, 2015; Epub ahead of print Sep 7, 2015

*This abstract was presented as a poster at University of North Carolina at Wilmington’s 2014 College of Health and Human Services First Annual Research Day, 11 April 2014; as well as a poster at North Carolina Physical Therapy Association Fall Conference, 10 October 2014.
INTRODUCTION
Stroke (cerebrovascular accident; CVA) and brain injury (BI) are diagnoses in the rehabilitation setting that often lead to decreased mobility. Once a person is less mobile, more time is spent in resting positions that can predispose them to muscle shortening, which can impact recovery of function.
Studies have reported a significant decrease in ankle dorsiflexion (DF) range of motion (ROM) after a CVA (1) and high prevalence of muscle tightness in the ankle following a traumatic BI (2). Loss of ankle DF ROM can affect regaining independence, mobility, deformities, spasticity, pain, and risk of pressure sores. Physical therapists address these deficits with interventions such as stretching, standing programmes, serial casting, splinting, and modalities.
Researchers have reported that the duration of stretch needed to be effective is greater than typically applied in a therapy session, specifically 6 h in the soleus (3). Others have compared stretching devices with neutral ankle positioning during the night with no significant difference (4). A systematic review concluded that stretching has minimal effects on joint mobility (5).
Standing programmes are used for increased duration of weight-bearing when addressing ankle tightness and cardiovascular endurance. Researchers found no significant difference between a standing programme group and a night splint group (6).
Serial casting is an intervention for reducing contracture in which consecutive casts are applied to provide a low load, prolonged stretch to increase ROM. Research has reported an increase in ankle DF with serial casting and casting with stretching in subjects after traumatic BI (7).
Splinting can be custom or pre-fabricated, static or dynamic, with various wearing schedules. Researchers have tested an adjustable ankle–foot orthosis for duration, with and without a nerve block and reported large increases in DF ROM (8).
Night positioning programmes using a cast, bed positioning, or a pressure-relieving ankle-foot orthosis (PRAFO) can provide longer stretching than manual therapy. A cast provides a custom rigid frame, whereas a PRAFO is generic and aligns the lower extremity while offsetting the heel.
In inpatient rehabilitation, therapists have limited time for hands-on approaches to maximize daytime sessions. The primary aim of this study was to assess the potential of night positioning for improving ankle ROM in patients with hemiparesis. It was hypothesized that the bivalve cast group would have the greatest benefit due to the rigid frame and the PRAFO would have greater gains than the control group by preventing excess plantarflexion during night hours.
MATERIALS AND METHODS
Study design
A prospective randomized controlled pilot study was conducted with approval from the Institutional Review Board. Participants were recruited from an inpatient rehabilitation hospital. The study randomized subjects to 1 of 3 arms for night positioning: bivalve cast; PRAFO; or control. All participants received individualized physical therapy for 60–90 min/day, 5–7 days/week. A waiver of consent was approved by the Institutional Review Board. A hand-out was provided to all participants or legally authorized patient representatives prior to enrollment, setting out study information and the right to withdraw.
Inclusion criteria included a diagnosis of CVA or BI with paresis of 1 or both sides of the body. Exclusion criteria were: contraindications to casting (9), prior stroke or ankle injury causing restricted ankle ROM, and agitation. It was determined that a pilot study would be needed to determine the necessary sample size due to lack of available baseline ankle ROM measurements in this patient population. Upon admission, patients were assessed for eligibility criteria by their evaluating physiotherapist. Participants were randomized using an electronic number generator and group assignments were provided in opaque envelopes, which were opened sequentially.
Intervention groups
For the bivalve cast group, a custom fibreglass cast was fabricated that extended from just distal to the fibular head to the distal interphalangeal joints. The subject was seated with the ankle held in subtalar neutral and submaximal DF. Within 24 h the cast was removed and made into a bivalve. The PRAFO group was provided with an off-the-shelf, semi-flexible Healwell Soft Ease Multi Ankle Foot Orthosis at neutral ankle positioning. The intervention groups were provided a wearing schedule of 8–12 h every night. Data-tracking sheets were utilized for duration of wear and to note daily skin checks.
Assessed outcomes
The primary outcome measure was passive ankle DF ROM with a 5° change as clinically significant (5). Secondary outcome measures included the Functional Independence Measure (FIM) scores for transfer and ambulation and lower extremity spasticity assessed with the Modified Ashworth Scale (MAS). The FIM is an 18-item motor and cognitive assessment utilizing a 7-point scale from total dependence to independence. Facility staff participated in annual FIM credentialing. The MAS is a 6-point scale that measures spasticity in individuals with a central nervous system lesion. Outcome measures were collected on admission, weekly, and upon discharge by the treating physiotherapist. All data were analysed with an intent-to-treat analysis.
Device/instrumentation
Research supports the need for standardized torque application to the joint and establishment of systematic methods rather than standard goniometry (10). A literature review for measurement of ankle DF revealed 2 devices found to have good to excellent reliability in prior studies: Modified Lidcombe template (11, 12) and Iowa Ankle Range of Motion device (13).
Based on prior research and current needs, a modified version of the Iowa Ankle Range of Motion device was constructed (Fig. 1). The device for this study consisted of 2 hinged Plexiglas plates: under the lower leg and a footplate. Two straps threaded through slits in the Plexiglas secured the lower leg. A digital inclinometer from Checkpoint, Inc. with a resolution of 0.1° was used to measure the angle of DF. A custom metal plate was fabricated to secure the inclinometer on the footplate during measurement. A FDK handheld force gauge from Wagner Instruments was chosen for its resolution of 0.45 kg and accuracy of ± 1%. A notch was created 30.48 cm above the centre of the hinge to ensure that force generation was applied perpendicular to the footplate.

Fig. 1. Ankle range of motion measure device using standardized torque (13).
A standardized protocol for measurement was developed. As this study was investigating ankle ROM for functional gains, subjects were positioned in supine with knee extension to simulate a standing position. With the force gauge in the notch, 6.8 kg of force was slowly applied to avoid the stretch reflex. Based on the findings by Wilken et al., a torque of 20.3 Nm was selected to ensure tolerance by elderly or frail participants (13).
Reliability of device
Participating physiotherapists were trained on the measurement procedure. Reliability testing was completed by 6 physiotherapists using the ankles of 2 healthy subjects. Each clinician completed 3 trials without feedback. The standardized measurement protocol was available during testing. The intraclass correlation coefficient was 0.53.
Data analysis
Data were reported in counts, frequencies, means, and standard deviations (SD). Categorical data were analysed using a χ2 test of independence or Fisher’s exact test, as appropriate. Numerical data were analysed with Kruskal–Wallis, and changes in measurement from admission to discharge were analysed using non-parametric analysis of covariance (ANCOVA), using baseline (admission) value as a covariate. Data were analysed using SAS 9.1 (SAS Institute, Cary, NC, USA). p-values less than 0.05 were considered significant and all applicable tests were 2-tailed.
RESULTS
A total of 46 patients agreed to participate in the pilot study between January 2012 and July 2013, with length of stay ranging from 9 to 55 days (Fig. 2). Nineteen patients (41.3%) were assigned to the control group, 14 (30.4%) to the PRAFO group, and 13 (28.3%) to the bivalve cast group (Table I). One subject in the PRAFO group had bilateral involvement, therefore 15 ankles were analysed. One subject in the control group dropped out with no discharge information to analyse. Subjects did not differ significantly in sex, age, injury type, side of injury, nor days from injury to intervention between arms, but differed significantly in baseline ROM.
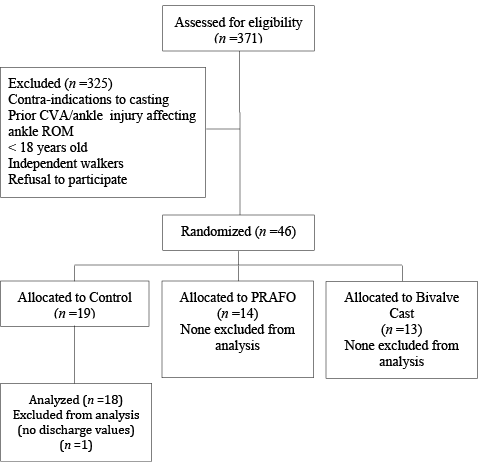
Fig. 2. Subject participation. ROM: range of motion; CVA: cerebrovascular accident; PRAFO: pressure-relieving ankle-foot orthosis.
|
Table I. Participant characteristics |
||||
|
|
Control |
PRAFO |
Bivalve cast |
p-value |
|
Participants, n (%) |
19 (41.3) |
14 (30.4) |
13 (28.3) |
n/a |
|
Sex, n |
||||
|
Female |
7 (36.8) |
5 (35.7) |
7 (53.8) |
0.5543 |
|
Male |
12 (63.2) |
9 (64.3) |
6 (46.2) |
|
|
Age, years, mean (SD) |
64.7 (15.6) |
65.4 (11.6) |
67.1 (11.0) |
0.9814 |
|
Diagnosis (%) |
||||
|
CVA |
19 (100) |
13 (92.9) |
13 (100) |
0.1077 |
|
BI (bilateral ankle) |
0 (0) |
1 (7.1) |
0 (0) |
|
|
Baseline |
||||
|
ROM, mean (SD) |
83.2 (5.2) |
82.1 (5.5) |
85.1 (7.7) |
0.4651 |
|
Spasticity, mean (SD) |
0.2 (0.4) |
0.3 (0.5) |
0.8 (1.1) |
0.2411 |
|
FIM transfer |
||||
|
Mean (SD) |
2.5 (1.1) |
1.6 (0.8) |
2.1 (0.9) |
0.0807 |
|
Median [IQR] |
2.0 [2.0–3.0] |
1.5 [1.0–2.0] |
2.0 [1.5–2.5] |
|
|
FIM walk |
||||
|
Mean (SD) |
0.9 (0.6) |
1.0 (0.7) |
1.1 (0.5) |
0.6714 |
|
Median [IQR] |
1.0 [1.0–1.0] |
1.0 [1.0–1.0] |
1.0 [1.0–1.0] |
|
|
Time from injury to intervention, days, mean (SD) |
n/a |
5.5 (2.3) |
10.8 (4.9) |
0.0840 |
|
Rehabilitation length of stay, days, mean (SD) |
27.7 (13.5) |
33.4 (11.5) |
29.3 (11.6) |
0.4206 |
|
PRAFO: pressure-relieving ankle-foot orthosis; ROM: range of motion; SD: standard deviation; IQR: interquartile range; BI: brain injury; CVA: cerebrovascular accident. |
||||
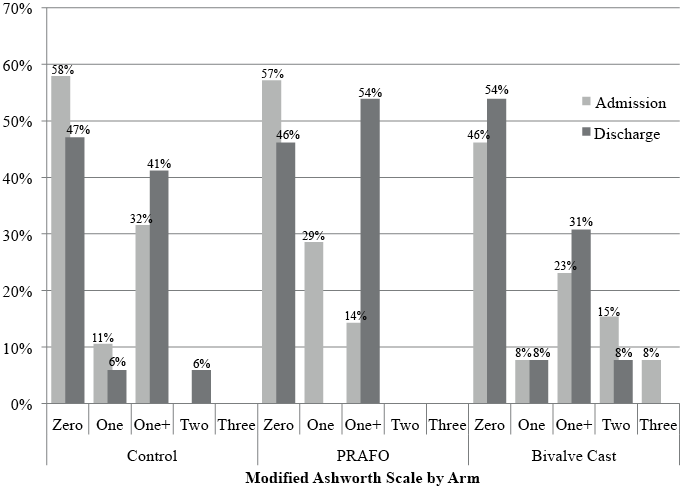
Differences in ROM, FIM transfer, FIM walking, and spasticity between admission and discharge were not significantly different between the 3 arms (Table II, Fig. 3).
|
Table II. Positioning device usage and changes in rehabilitation outcomes |
||||
|
Measurement |
Control |
PRAFO |
Bivalve cast |
p-value |
|
Positioning device usage |
||||
|
Time in cast, min/day, median [IQR] |
NA |
655.0 [515.0–740.0] |
665.0 [580.0–725.0] |
0.3079 |
|
Admitted days tracked, n (%) |
NA |
237 (64.1) |
195 (69.6) |
0.1351 |
|
Days patient refused, n (%) |
NA |
11 (3.0) |
33 (11.8) |
< 0.0001 |
|
Rehabilitation outcomes |
||||
|
FIM transfer |
||||
|
Mean (SD) |
1.8 (1.1) |
2.0 (1.3) |
2.0 (1.2) |
0.9272 |
|
Median [IQR] |
2.0 [1.0–2.0] |
2.0 [2.0–3.0] |
2.0 [1.0–3.0] |
|
|
FIM walk |
||||
|
Mean (SD) |
2.25 (1.8) |
2.0 (1.7) |
2.25 (1.9) |
0.8897 |
|
Median [IQR] |
2 [0.5–4.0] |
2 [0.0–3.0] |
2.5 [0.5–3.5] |
|
|
Range of motion, mean (SD) |
1.75 (21.4) |
4.5 (12.7) |
–1 (6.4) |
0.5666 |
|
Changes in outcomes measured as (measure at discharge – measure at admission); adjusted for baseline values. FIM: Functional Independence Measure; IQR: interquartile range; PRAFO; pressure-relieving ankle-foot orthosis; SD: standard deviation. |
||||
Participants spent a similar number of total minutes per day in either intervention device (Table II). Staff appropriately tracked device usage 64.1% (PRAFO) and 69.6% (bivalve cast) of the days after implementation of the intervention, but compliance did not differ significantly between groups. Staff documented subject refusal of the bivalve cast (11.8%) significantly more often than for the PRAFO (3.0%, p < 0.0001).
DISCUSSION
The aim of this study was to determine the effectiveness of night positioning devices on preventing muscle shortening or enhancing outcomes in patients with CVA or BI. Extensive literature reviews were completed and no evidence was found that evaluated the use of commonly utilized lower extremity night positioning devices.
The results of this pilot study were unable to show a significant difference in ankle ROM between the 3 groups at the current sample size. Although daytime interventions were not tracked, improved DF ROM in control and PRAFO groups may be partially due to the 3 h of combined physical and occupational therapy provided with variable durations of time spent with the ankle in weight-bearing. The mean loss of 1° of ankle ROM in the cast group may have been due to longer time from admission to application of the cast, increased baseline spasticity, sample size, or increased refusals.
Contrary to the hypothesis, there were no significant differences in spasticity between groups, although there were increased MAS scores for the control and PRAFO groups at discharge. The bivalve group had decreased discharge spasticity, although this was not statistically significant. The bivalve cast group was anticipated having less spasticity compared with the other groups because of the extensive evidence that supports casting for spasticity management. Most literature is on serial casting with longer duration of wear; whereas the current study applied and removed the cast in a day in order to fabricate a custom night splinting device. Subjects were randomly assigned into groups; therefore those with greater spasticity were not specifically chosen for the bivalve cast group. No previous studies have looked solely at an ankle bivalve cast for night wear and spasticity outcomes; however, there has been conflicting research on duration of positioning for various types of hand splints that report no reduction in spasticity over usual therapy (14).
Another aim of the study was to determine whether mobility outcomes varied between the groups. This, however, could not be determined with the current sample size. Most literature assessing the effects of splinting on activity are for the upper extremity and report no change in the motor assessment scale (14).
It was hypothesized that there would be less tolerance to the bivalve cast secondary to possible discomfort for the patient. Although data for intervention application in this study did not contain all needed values, there was similar tolerance between groups. There were significantly more documented refusals for the bivalve cast group, but the same number of patients refused the devices in both groups. It is also noted that positioning programmes may be more applicable when applied to lower level neurological patients with spasticity or severely limited mobility. Anecdotally through data collection in this pilot study, night positioning programmes may be more beneficial for cognitively intact patients, those with involved family members, or with staff accustomed to these programmes.
The results of this study indicate that further research is needed to determine whether night positioning is beneficial to affect ankle ROM, improve spasticity, or change mobility outcomes. Through gathering baseline values, a retrospective power analysis found that 234 subjects are needed for future studies to determine significance.
Study limitations
Clinical site research and randomized controlled trials are vital to the medical community to provide realistic information to support evidence-based practice, but are accompanied by additional limitations. This pilot study provides information to plan future research, but was limited by sample size power and decreased compliance for device application in the clinical setting. Extensive education and communication strategies were implemented to maximize compliance before and throughout the study. Possible barriers included the novelty of the intervention and research approach at the facility, involvement of a large number of staff, and collection of data via paper documentation.
Other limitations in this pilot study include: investigators did not track reasons for subjects who were not enrolled, blinding was not possible due to active participation of the staff and subjects with the intervention, and medications, specifically anti-spasticity interventions, were not tracked. Long-term effects were not analysed with patient follow up, as the study design was to look at benefits during the inpatient rehabilitation stay.
Conclusion
Future studies are needed in order to provide evidence-based interventions that can benefit patients with hemiparesis. Muscle-shortening, spasticity, and decreased mobility are major impairments that effect outcomes and quality of life in persons after BI or CVA. Further research into night positioning is needed to determine the most effective interventions to address these limitations and maximize daytime therapeutic treatment.
ACKNOWLEDGMENTS
The authors would like to thank Nivedita Bhatt, PhD for her significant work on statistical analysis. The authors would also like to thank Kelly Hewett, SPT for her contributions during data collection and are grateful to all contributing staff and participants in the study.
Conflicts of interest: We certify that no party having a direct interest in the results of the research supporting this article has or will confer a benefit on us or on any organization with which we are associated.
REFERENCES

