Yuko Kasashima-Shindo, MD1, Toshiyuki Fujiwara, MD, PhD1,2, Junichi Ushiba, PhD3, Yayoi Matsushika, MS3, Daiki Kamatani, PhD1, Misa Oto, MS3, Takashi Ono, MS3, Atsuko Nishimoto, OTR1, Keiichiro Shindo, MD, PhD1, Michiyuki Kawakami, MD, PhD1, Tetsuya Tsuji, MD, PhD1 and Meigen Liu, MD, PhD1
From the 1Department of Rehabilitation Medicine, Keio University School of Medicine, Tokyo, 2Department of Rehabilitation Medicine, Tokai University School of Medicine and 3Department of Biosciences and Informatics, Faculty of Science and Technology, Keio University, Kanagawa, Japan
OBJECTIVE: Brain–computer interface technology has been applied to stroke patients to improve their motor function. Event-related desynchronization during motor imagery, which is used as a brain–computer interface trigger, is sometimes difficult to detect in stroke patients. Anodal transcranial direct current stimulation (tDCS) is known to increase event-related desynchronization. This study investigated the adjunctive effect of anodal tDCS for brain–computer interface training in patients with severe hemiparesis.
SUBJECTS: Eighteen patients with chronic stroke.
DESIGN: A non-randomized controlled study.
METHODS: Subjects were divided between a brain–computer interface group and a tDCS-brain–computer interface group and participated in a 10-day brain–computer interface training. Event-related desynchronization was detected in the affected hemisphere during motor imagery of the affected fingers. The tDCS-brain–computer interface group received anodal tDCS before brain–computer interface training. Event-related desynchronization was evaluated before and after the intervention. The Fugl-Meyer Assessment upper extremity motor score (FM-U) was assessed before, immediately after, and 3 months after, the intervention.
RESULTS: Event-related desynchronization was significantly increased in the tDCS- brain–computer interface group. The FM-U was significantly increased in both groups. The FM-U improvement was maintained at 3 months in the tDCS-brain–computer interface group.
CONCLUSION: Anodal tDCS can be a conditioning tool for brain–computer interface training in patients with severe hemiparetic stroke.
Key words: event-related desynchronization; upper extremity motor function; stroke; rehabilitation; electroencephalography; brain stimulation; brain–machine interface.
J Rehabil Med 2015; 47: 00–00
Correspondence address: Toshiyuki Fujiwara, Department of Rehabilitation Medicine, Tokai University School of Medicine, 143 Shimokasuya, Isehara, Kanagawa 259-1193, Japan. E-mail: tofuji@xc5.so-net.ne.jp
Accepted Oct 28, 2014; Epub ahead of print Feb 5, 2015
Introduction
More than half of patients with stroke cannot achieve full recovery from motor impairment. (1). Various treatments have been developed to facilitate motor recovery of the paretic upper extremity (UE) in stroke patients. However, functional recovery depends on the severity of motor impairment (2). Langhorne et al. (3) performed a meta-analysis of multiple clinical trials and found that few treatments consistently improved hand motor function. The prognosis of functional motor recovery for severely affected UEs is poor. More recently, some newer interventions have been applied for UE rehabilitation, such as constraint-induced movement therapy (CIMT) (4), robot-assisted arm training (5), hybrid assistive neuromuscular dynamic stimulation (HANDS) therapy (6) and brain–computer interface (BCI) training (7–11). BCI training, in particular, can be a revolutionary method for patients with severe hemiparesis who have undergone few effective treatments (9).
BCI technology can directly translate brain signals into commands for the control of external devices (12). BCI systems estimate a patient’s motor intention based on the amplitude modulation of the mu rhythm (7), which is typically found over the sensorimotor cortex with a frequency of 8–13 Hz and is attenuated by movement execution and imagery. This phenomenon is referred to as event-related desynchronization (ERD). The ERD of the mu rhythm, termed mu ERD, is interpreted as the desynchronized activities of the activated neurones. The mu ERD is known to appear in the motor area during motor execution, preparation or imagery (13). However, the application of BCI in patients with severe motor disabilities has been limited because it is sometimes difficult to detect a sufficiently strong ERD (14). If ERD can be potentiated, it would be easier to utilize BCI in patients with severe motor disabilities.
Transcranial direct current stimulation (tDCS) is a non-invasive brain stimulation method that can modulate cortical excitability by inducing a weak current on the scalp (15). Anodal tDCS increases motor cortex excitability, whereas cathodal tDCS decreases it (15). Some studies have reported that combining tDCS with rehabilitation may potentiate the effect of rehabilitation (16, 17). Furthermore, it has been suggested that motor recovery following stroke or motor relearning of the paretic limb is maximized by anodal tDCS (18).
Matsumoto et al. (19) reported that anodal tDCS increased the magnitude of mu ERD induced by motor imagery in healthy subjects. They found that the magnitude of mu ERD was related to motor cortex excitability. Kasashima et al. (14) showed that anodal tDCS over the affected hemisphere increased the magnitude of mu ERD during paretic finger motor imagery in stroke patients. Therefore, it was assumed that anodal tDCS would potentiate ERD for BCI applications.
The hypothesis of this study was that the application of anodal tDCS could potentiate the effects of BCI training in stroke patients. This study explored the adjunctive effect of tDCS for BCI training and the long-lasting effects of BCI training in patients with chronic severe hemiparetic stroke.
Material and Methods
A non-randomized, controlled, cohort before–after, single-blind trial was conducted in patients with chronic hemiparetic stroke.
Participants
Participants were recruited from an outpatient rehabilitation clinic of a university hospital. Patients were included in the study if they met the following criteria: (i) a first unilateral subcortical stroke not involving the sensorimotor cortex as confirmed by brain magnetic resonance imaging (MRI) or computed tomography (CT); (ii) time from stroke onset of more than 180 days; (iii) ability to raise the paretic hand to the height of the nipple; (iv) inability to extend the paretic fingers; (v) no motor improvement during the 30 days prior to starting the intervention as confirmed by both the patients and their physicians; (vi) ability to walk independently in their daily lives; (vii) no severe cognitive deficits as determined by a Mini Mental State Examination score > 25; (viii) no severe pain in the paretic UE; (ix) no pacemaker or other implanted stimulator; and (x) no history of seizures within the past 2 years and no use of anticonvulsants at 1 month before the intervention.
From August 2009 to March 2011, 24 patients visited the outpatient clinic to join this study. Six patients were excluded because they did not meet the inclusion criteria, and 18 patients were enrolled in the study. The study purpose and procedures were explained to the participants, and written informed consent was obtained from each. No patient had a history of seizures. Two patients, who had brain surgery in the acute stroke phase, and 5 patients, who had used anticonvulsants until more than 1 month before the intervention, were assigned to the BCI group in order to avoid adverse events due to brain stimulation. The others were assigned to the BCI combined with tDCS group (tDCS-BCI group). No changes were made in medications, such as anti-spastic drugs, from 1 month before until 3 months after the intervention. No participant received any pharmacological therapies to enhance or modify motor recovery during the same period. The study was approved by the institutional ethics review board and was registered at the UMIN Clinical Trial Registry (UMIN000002121).
Electroencephalographic recording
Electroencephalography (EEG) was performed with Ag–AgCl electrodes (1 cm in diameter), with a right ear reference at C3 in patients with right hemiparesis and at C4 in patients with left hemiparesis, according to the international 10–20 system. An additional electrode was placed at a position 2.5 cm anterior to C3 or C4. A ground electrode was placed on the forehead, and the reference electrode was placed on either A1 or A2 (ipsilateral to the affected hemisphere). EEGs were recorded in a bipolar manner and were filtered with a bandpass of 2–100 Hz. The signals were digitized at 256 Hz using a biosignal amplifier (g.USBamp, g. tec medical engineering GmbH, Austria). Surface electrodes were placed bilaterally on the skin overlying the extensor digitorum communis (EDC) muscle to confirm the absence of electromyographic (EMG) activity during motor imagery tasks and to avoid unexpected muscle contraction (1,024 Hz sampling with a bandpass of 10–512 Hz).
Event-related desynchronization quantification
As a feature representing the participant’s motor imagery, mu ERD, which is a diminution of the alpha band (8–13 Hz) of the mu rhythm amplitude, was used to control the BCI. The ERD was expressed as the percentage of the power decrease related to the 1-s reference interval before the direction of imagery. The ERD at a certain frequency was calculated for each time and frequency according to equation (1):
ERD (f, t) = {(R(f) − A(f, t)) / R(f)} × 100 (%); (1)
where A(f, t) is the power spectrum density of the EEG at a certain frequency band f [Hz] and time t [s] since the imagery task was started, and R(f) is the power spectrum at the same frequency f [Hz] of the baseline period.
Brain–computer interface training
Motor imagery-based BCI training was carried out for approximately 45 min a day, 5 times a week, for a total of 10 days. All participants received 40 min of standard occupational therapy per day, which consisted of gentle stretching exercises, active muscle re-education exercises and introduction to bimanual activities in their daily lives.
Details of the training protocol are described in detail elsewhere (8). A brief overview is given here. The participants were seated in a comfortable chair with their arms supported and relaxed on the armrest in pronation. They were facing a 15.4-inch computer monitor placed approximately 60 cm in front of their eyes. A motor-driven orthosis with a servomotor (9.5 kg·cm for output torque at 4.8 V supply; S9351, Futaba Sangyo, Tokyo, Japan) was attached to the affected hand to achieve finger extension–flexion movement at the metacarpophalangeal joints (Fig. 1).
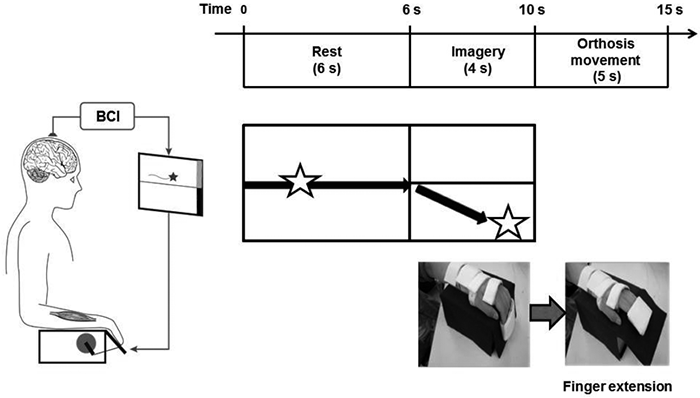
A star-shaped cursor began to move at a fixed rate from left to right across the monitor over a 10-s period. Participants were instructed to rest for 6 s and then to either imagine extending their affected fingers or remain relaxed for the next 4 s, depending on the task cue on the monitor. If the mu ERD was detected after the cue instruction to imagine finger extension, the star-shaped cursor moved down on the screen as a visual feedback, and then the motor-driven orthosis extended their affected fingers for 5 s (Fig. 1). Each trial was performed at 30-s intervals. One training session consisted of 10 trials of motor imagery and 10 trials of relaxation, presented in a randomized order. Daily BCI training consisted of 3 training sessions.
A calibration session was performed before the training session to adjust the EEG classification parameters, as described elsewhere (20). In a randomized order, the participants were asked either to imagine extension of their paretic fingers or to remain relaxed for 4 s. Each task was repeated 20 times.
Transcranial direct current stimulation (tDCS)
Participants in the tDCS-BCI group received anodal tDCS over the affected hemisphere before BCI training. The tDCS was applied through rectangular, saline-soaked sponge electrodes (50 × 70 mm) with a battery-driven stimulator (CX-6650, Rolf Schneider Electronics, Gleichen, Germany). The position of the primary motor cortex (M1) of the affected hemisphere was determined as a site symmetrically opposite to the unaffected M1 side. This was confirmed by induction of the largest motor-evoked potential (MEP) in the unaffected EDC muscle with constant stimulus intensity using transcranial magnetic stimulation (TMS) with a figure-of-eight stimulation coil connected to a Magstim 200 magnetic stimulator (Magstim, Whitland, UK). The MEPs were used on the unaffected M1 because the MEPs on the affected M1 were not evoked well in all patients. The anode electrode was placed over the M1 of the affected hemisphere, and the cathode was placed over the contralateral supraorbital area. tDCS was applied for 10 min with a current intensity of 1 mA. Participants were awake and sat in an upright position in a comfortable armchair during stimulation.
The positions of EEG electrodes were established before tDCS. For placing the stimulation electrodes, the EEG electrodes over the stimulus sites were removed after marking the scalp. After the tDCS stimulation, the EEG electrodes were placed in the same position as before, and this procedure took less than 1 min.
Outcome measures
The following clinical assessments and the measurement of mu ERD were conducted 1 day before (before) and after the intervention (post-), as described below. The accuracy rate of BCI training was also calculated on each day. To determine the long-term effects, the clinical evaluations were also assessed 3 months after the intervention (3 months) (Fig. 2).
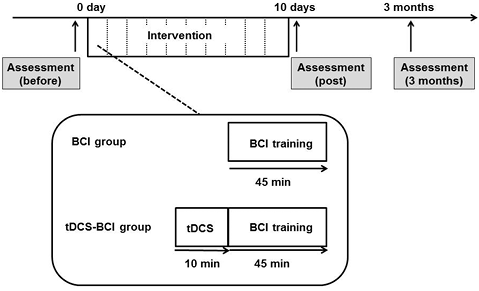
Fig. 2. Experimental design. All participants received the intervention of 10 days of training, which consisted of 1 × 45-min brain–computer interface (BCI) training session per day. The participants in the transcranial direct current stimulation (tDCS)-BCI group received anodal tDCS (1 mA, 10 min) over the affected motor cortex immediately prior to every BCI training session. Clinical examinations were performed 1 day before (before), 1 day after (post), and 3 months after the intervention (3 months).
Clinical assessments
UE motor function was assessed with the Fugl-Meyer Assessment UE motor score (FM-U) (66 points, total score) (21). The FM-U includes 33 items and consists of test A (shoulder/elbow/forearm: 36 points, A score), test B (wrist: 10 points, B score), test C (hand/finger: 14 points, C score) and test D (coordination: 6 points, D score). The D score was excluded because all patients in this study could not touch their noses with their index finger fully extended and had no remaining finger extension. The FM-U was assessed according to the scoring manual (22), and the validity and reliability of this method has been previously confirmed (23). Spasticity was measured with the Modified Ashworth Scale (MAS) (24) for finger, wrist and elbow flexors.
The FM-U and the MAS were scored by an independent assessor who was blinded to the allocation of the participants. This assessor scored all patients with stroke who were admitted to the department during the study period, including patients not recruited for this study.
The brain lesions were assessed with MRI or CT. The volumes of haemorrhage were calculated by the ABC/2 method, where A is the greatest haemorrhage diameter by MRI, B is the diameter 90° to A, and C is the approximate number of slices with haemorrhage multiplied by the slice thickness (25).
Assessment of mu event-related desynchronization
The values of mu ERD during motor imagery of extension of the affected fingers were assessed 1 day before and 1 day after the 10-day intervention. The detail method was described previously (14) and is summarized in Appendix S11.
Accuracy rate of brain–computer interface training
The numbers of successful performances (i.e. moving the orthosis after imagery cues and not moving after the resting cues) were counted, and the accuracy rate was calculated as the number of successful performances divided by the number of trials. The mean accuracy rates on the first day and the last day of BCI training were compared.
Data analysis
Student’s t-test was used to compare the baseline data of age, time from stroke onset and FM-U total score/subscores of the 2 groups. The Mann–Whitney U test was used to compare the baseline data of volumes of haemorrhage and MAS scores. The normality of the distribution of these variables was confirmed with the Kolmogorov–Smirnov test. A χ2 test was used to compare categorical variables (gender, type of stroke, paretic side and lesion) of the 2 groups. Differences were considered significant if p < 0.05.
A 2-factor mixed factorial analysis of variance (ANOVA) was used to compare the FM-U and MAS scores with the between-subjects factor of Intervention (BCI and tDCS-BCI groups) and the within-subjects factor of Time (before, post- and 3 months). The mu ERD and accuracy rate were also analysed using a 2-factor mixed factorial ANOVA with the between-subjects factor of Intervention (BCI and tDCS-BCI groups) and the within-subjects factor of Time (before and post for the mu ERD; the first and last trials for the accuracy rate). If the difference within the subjects was significant, post-hoc analysis was performed with a paired t-test in the FM-U, mu ERD and accuracy rate, and the Wilcoxon signed-rank test in the MAS. All statistical analyses were performed with SSPS version 18.0J (SPSS Japan, Japan).
Results
All participants finished the intervention without experiencing any adverse effects. Table I shows the clinical characteristics of the participants. There were no significant differences between the 2 groups in any of the clinical evaluation items (age, time from onset of stroke, gender, type of stroke, paretic side, lesion and FM-U) before the intervention, except for the MAS of the finger flexors (Table I).
|
Table I. Clinical characteristics of participants |
|||
|
tDCS-BCI group (n = 11) |
BCI group (n = 7) |
p-value |
|
|
Age, years, mean (SD) |
53.5 (12.4) |
48.0 (9.7) |
0.441 |
|
TFO, months, mean (SD) |
46.2 (20.2) |
56.4 (36.4) |
0.389 |
|
Gender, M/F, n* |
9/2 |
4/3 |
0.225 |
|
Type of stroke* |
0.629 |
||
|
Ischaemic, n |
6 (1 lacunar) |
3 (1 lacunar) |
|
|
Haemorrhagic, n |
5 |
4 |
|
|
Volume of lesion* (mm3), mean (SD) |
8,000 (7,282) |
34,083 (29,795) |
0.268 |
|
Paretic side, right/left, n* |
6/5 |
5/2 |
0.417 |
|
Lesion, n* |
|||
|
Putamen |
4 |
3 |
0.398 |
|
Corona radiata |
0 |
1 |
|
|
Putamen-corona radiata |
6 |
3 |
|
|
Thalamus |
1 |
0 |
|
|
FM-U |
27.6 (11.2) |
23.4 (13.8) |
0.487 |
|
MAS, median (min-max)** |
|||
|
Finger flexors |
1+ (1, 2) |
2 (1+, 3) |
0.038 |
|
Wrist flexors |
2 (1, 3) |
2 (1, 3) |
0.845 |
|
Elbow flexors |
1+ (1, 2) |
1+ (1, 2) |
0.316 |
|
p-values were calculated with Student’s t-test, χ2 tests* or Mann-Whitney U test**. TFO: time from onset of stroke; FM-U: Fugl-Meyer Assessment upper extremity motor score; MAS: Modified Ashworth scale; tDCS: transcranial direct current stimulation; BCI: brain–computer interface; M: male; F: female. |
|||
In the clinical assessment, 2 participants were not assessed at 3 months. One in the BCI group received different treatment after the intervention, and 1 in the tDCS-BCI group did not show up. The changes of the FM-U and MAS are shown in Table II. The 2-factor mixed factorial ANOVA showed no significant interaction effect between Intervention and Time in the total FM-U score (F(2,28) = 2.43, p = 0.107), the A score (F(2,28) = 2.96, p = 0.068), the B score (F(2,28) = 0.18, p = 0.833) and the C score (F(2,28) = 1.56, p = 0.228). It showed a significant main effect of Time in the total FM-U score (F(2,28) = 17.42, p < 0.001), the A score (F(2,28) = 8.19, p = 0.002) and the C score (F(2,28) = 10.94, p < 0.001), but not in the B score (F(2,28) = 3.02, p = 0.065). A post-hoc paired t-test showed significant differences in the total, A and C scores between before and post- (p < 0.001, p = 0.004 and p = 0.011, respectively), and between before and 3 months (p = 0.001 for all) in the tDCS-BCI group. In contrast, in the BCI group, there were significance differences between before and post- in the total and C scores (p = 0.027, p = 0.038, respectively), and a not significant but slight improvement in the A score (p = 0.056). There was no significant difference in all of the scores between before and 3 months (total score: p = 0.093, A score: p = 0.376, C score: p = 0.139).
|
Table II. Clinical assessment scores |
||||||||||
|
|
tDCS-BCI group |
BCI group |
Interaction p |
Main effect of time p |
||||||
|
Before (n = 11) |
Post (n = 11) |
3 months (n = 10) |
Before (n = 7) |
Post (n = 7) |
3 months (n = 6) |
|||||
|
FM-U, mean (SD) |
||||||||||
|
A |
21.64 (7.32) |
23.91 (7.20)** |
26.10 (6.49)** |
18.29 (8.98) |
22.00 (8.19) |
21.17 (9.56) |
0.068 |
0.002 |
||
|
B |
1.55 (1.86) |
2.73 (2.61) |
2.40 (1.58) |
1.43 (2.51) |
2.29 (2.75) |
2.67 (2.42) |
0.833 |
0.65 |
||
|
C |
4.45 (2.54) |
7.00 (2.76)* |
7.90 (2.23)** |
3.71 (2.75) |
5.71 (2.98)* |
5.67 (1.51) |
0.228 |
< 0.001 |
||
|
Total |
27.64 (11.17) |
33.64 (10.91)** |
36.40 (8.72)** |
23.43 (13.79) |
30.00 (12.48)* |
29.50 (12.23) |
0.107 |
< 0.001 |
||
|
MAS, median (min–max) |
||||||||||
|
Finger |
1+(1, 2) |
1 (0, 2)* |
1 (0, 1+)** |
2 (1+, 3) |
1+ (1, 3)* |
1 (1, 2)* |
0.663 |
< 0.001 |
||
|
Wrist |
2 (1, 3) |
1+ (0, 3) |
1 (0, 2)* |
2 (1, 3) |
1+ (1, 3) |
1~1+ (1, 1+) |
0.230 |
< 0.001 |
||
|
Elbow |
1+ (1, 2) |
1 (1, 1+)* |
1 (0, 1+)* |
1+ (1, 3) |
1+ (1, 2) |
1 (0, 1+) |
0.608 |
< 0.001 |
||
|
*p < 0.05, **p < 0.01 compared with the score of before; post-hoc paired t-test for the FM-U, Wilcoxon signed-rank test for the MAS. tDCS: transcranial direct current stimulation; BCI: brain–computer interface; FM-U: Fugl-Meyer Assessment upper extremity motor score; A: shoulder/elbow/forearm, 36 points; B, wrist, 10 points; C: hand/finger, 14 points; MAS: Modified Ashworth scale; finger: finger flexors; wrist: wrist flexors; elbow: elbow flexors; SD: standard deviation. |
||||||||||
The 2-factor mixed factorial ANOVA showed no significant interaction between Intervention and Time (p > 0.05), and a significant main effect of Time (p < 0.001) in the MAS of the finger, wrist and elbow flexors. The Wilcoxon signed-rank test showed a significant decrease in the MAS of the finger flexors in both groups between before and post- (tDCS-BCI group: p = 0.011, BCI group:p = 0.038) and between before and 3 months (p = 0.004, 0.024, respectively). There were also tendencies toward decrease in the MAS of the elbow and wrist flexors in both groups between before and post- (tDCS-BCI group: p = 0.025 and 0.059, BCI group: p = 0.102 and 0.102, respectively) and between before and 3 months (p = 0.016 and 0.010, p = 0.059 and 0.102, respectively).
The changes in the mu ERD values are shown in Fig. 3. The 2-factor mixed factorial ANOVA showed a significant interaction between Intervention and Time (F(1,16) = 6.94, p = 0.018), and a significant main effect of Time (F(1,16) = 14.68, p = 0.001). The post-hoc paired t-test showed a significant increase in the mu ERD values between before and post- in the tDCS-BCI group (p < 0.001), but not in the BCI group (p = 0.483).

The mean accuracy rate in the tDCS-BCI group increased from 49.91 ± 7.92% to 58.68% (SD 8.62), whereas it increased in the BCI group from 52.10% (SD 9.39) to 55.76% (SD 4.42). The 2-factor mixed factorial ANOVA showed no significant interaction between Intervention and Time (F(1,16) = 2.34, p = 0.145), and a significant main effect of Time (F(1,16) = 14.12, p = 0.002). The post-hoc paired t-test showed a significant improvement between the first and last trials in the tDCS-BCI group, but not in the BCI group (tDCS-BCI group: p = 0.001, BCI group: p = 0.220).
Discussion
The present study demonstrated that a 10-day BCI training improved motor function in patients with chronic severe hemiparetic stroke. Although there was a significant increase in ERD only in the tDCS-BCI group, no significant difference was found in improvement in motor function between the 2 groups. The tDCS-BCI group, however, showed a slightly longer-lasting improvement in motor function compared with the BCI group.
BCI training may produce an increase in appropriate brain activity and lead to the restoration of function through neuroplasticity (12). Shindo et al. (8) showed that BCI training increased the motor cortex excitability of the affected hemisphere, as confirmed with TMS. Functional MRI showed that BCI training increased ipsilesional motor cortex and premotor cortex activities (9). The combination of a coincident movement of the paretic fingers and the volitional brain signals by BCI training may induce sensorimotor integration and increase the recruitment of descending corticospinal fibres. These increments of excitability of motor pools may induce neural plasticity or neural compensation, leading to improvement in motor function.
Anodal tDCS increases cortical excitability (15) because of the increase in spontaneous neurone firing (26, 27) and the modulation of resting membrane potential (26, 28). Anodal tDCS is known to facilitate immediate production of mu ERD in healthy subjects and stroke patients (14, 19). Anodal tDCS could help to improve decoding of brain signals during BCI training by immediately increasing mu ERD, which might lead to an additional increase in mu ERD even after the BCI training was completed. It has been reported that ERD was correlated with M1 excitability (29) and blood-oxygen-level-dependent (BOLD) response (30). An increase in mu ERD in the tDCS-BCI group may be related to neural excitation in the affected hemisphere. Although tDCS could lead to an increase in ERD, we could not find a clear difference in motor improvement between the tDCS-BCI and BCI groups in this study. There was no interaction effect between Intervention and Time. It is possible that anodal tDCS improves motor function (31), but the effect may be limited only to patients with milder paresis (32). There was no substantial difference in the accuracy rate in this study. This could mean that the number of doses offered in successful trials of BCI training was not high enough to improve motor function. However, a more extensive change in brain signals (i.e. ERD) could result in a more significant long-term effect.
We found a reduction in spasticity in both groups. This may be due to the increase in awareness and learning of relaxation that comes through BCI training. It is difficult for patients with severe motor impairment to recognize their affected hand. BCI training can help patients concentrate on their affected hand, resulting in increases in awareness and use of the affected UE in their activities of daily living (8). In addition, the sequential training between relax and imagery may enable patients to learn how to decrease involuntary muscle activity (8). These effects of BCI training could have an impact on the whole UE, leading to improvements in proximal, as well as distal, portions. All participants received occupational therapy for 40 min per day in addition to the intervention. Occupational therapy may also contribute to the improvement. However, the change in the FM-U from baseline to post-intervention was 6.6 ± 6.0 points in our BCI group. This improvement was better than the changes in the FM-U only by conventional therapy for severe chronic patients with stroke in previous studies, showing that conventional therapies for 6–8 weeks resulted in 1.2–2.2 point improvements in the FM-U (5, 33, 34).
Study limitations
Several limitations must be considered regarding this study. First, the method of group allocation could have given rise to bias. The allocation of participants to the tDCS-BCI and BCI groups was controlled, but not randomized, with different group sizes among small samples. We excluded subjects who had undergone brain surgery or who were at risk for seizures from the tDCS-BCI group, while including them in the BCI group. There was no sham stimulation in the BCI group. The clinical features in the 2 groups, such as the gender, size of stroke, lesion side and motor function, were not significantly different except for finger spasticity. These discriminations, however, may have introduced a further variable. Secondly, anodal tDCS was applied for only 10 min immediately before the BCI training. The effect of 10 min of anodal tDCS with an intensity of 1 mA on TMS-evoked MEPs was shown to be maintained for less than 40 min in a previous study (35). In this study, the BCI training was performed for 45 min. The effect of the tDCS may have been lost by the end of the training. Thirdly, the position of M1 of the affected hemisphere was determined by using the symmetrical opposite side as a marker, that is, M1 of the unaffected hemisphere. This is not the exact position as identified by MEP of the affected EDC through directly stimulating the affected hemisphere. Finally, there is a possibility that some participants did not imagine well, which is very difficult to assess. The development of more effective BCI systems for stroke patients in terms of feedback accuracy, delay and modality is needed.
Conclusion
Anodal tDCS can be used as a conditioning tool for BCI training to increase ERD for the trigger of BCI. However, further randomized controlled trials are needed to ascertain the real effect of BCI training and the adjunctive effect of anodal tDCS for BCI training in more homogenous stroke populations.
AcknowledgementS
This study was partially supported by Health Labour Sciences Research Grant (12102976) and the Strategic Research Program for Brain Sciences (SRPBS) of the Ministry of Education, Culture, Sports, Science, and Technology of Japan. The authors thank Sawako Otaki for her contributions to this study.

1http://www.medicaljournals.se/jrm/content/?doi=10.2340/16501977-1925
References


