Mathieu Panchoa de Sèze, MD, PhD1, Etienne Guillaud, PhD2, Laure Slugacz, MD1 and Jean René Cazalets, PhD2
From the 1University Hospital of Bordeaux and Research group EA 4136 Handicap and Nervous System, and 2University of Bordeaux CNRS UMR 5287, Bordeaux, France
OBJECTIVE: Camptocormia is a disabling pathology of the axial system that debilitates patients in their daily life. To date, there have been no studies evaluating the impact of camptocormia on walking performance. This study presents a new method for assessing sagittal posture under walking conditions in patients with camptocormia.
DESIGN: The severity of camptocormia was evaluated by measuring sagittal inclination, represented indirectly by the horizontal distance between the C7 and S1 markers (C7 sagittal arrow; C7-SAR). Sagittal inclination was measured under various behavioural conditions using clinical, radiological and kinematic approaches.
Patients: Forty-three patients were included in the study (17 with Parkinson’s disease and 26 with idiopathic camptocormia).
RESULTS: Under static conditions, C7-SAR could be assessed using different methods. During walking, there was a dramatic increase in C7-SAR values. Correlation analysis revealed a relationship between functional impairment and dynamic C7-SAR values, but not with radiological C7-SAR values. Patients with Parkinson’s disease behaved differently from idiopathic patients, suggesting the involvement of different underlying physiopathological mechanisms.
CONCLUSION: Monitoring sagittal inclination during walking is more accurate than radiological measurements to determinine the detrimental effects of camptocormia and its consequences for quality of life.
Key words: spine; locomotion; adult spinal muscular atrophy; Parkinson’s disease.
Correspondence address: Jean-René Cazalets, Université Bordeaux CNRS UMR 5287, INCIA, Zone nord, Bat 2, 2e étage, 146, rue Leo Saignat, 33076 Bordeaux cedex France. E-mail: jean-rene.cazalets@u-bordeaux.fr
J Rehabil Med 2014; 46: 00–00
Accepted Jun 10, 2014; Epub ahead of print Sep 29, 2014
The disabling axial system pathology camptocormia (or bent spine syndrome) is defined as an abnormal posture with marked forward flexion of the thoraco-lumbar spine. Classically, camptocormia is diagnosed when excessive bending is observed, with an increase during walking and disappearance in the supine position, or when patients can undertake active straightening by pushing with their hands against their thighs or leaning against a wall (1). This definition indicates that the symptoms of camptocormia may cover a wide variety of physiopathological disorders. Indeed, camptocormia may be associated with several aetiologies, including neurological disorders with dystonia, amyotrophy and structural changes in the spine (2). Its physiopathology is not univocal and an association of neuromuscular disease and degenerative spinal processes is thought to explain its occurrence (3). Furthermore, there are no consensus criteria for camptocormia diagnosis, therefore its prevalence is difficult to determine. For example, depending on the study reported, the prevalence of camptocormia in Parkinson’s disease (PD) may range from 3% to 17% (4). Some authors have arbitrarily defined camptocormia by an angle of forward flexion greater than 45° when standing or walking (4, 5). Since camptocormia induces compensation, with retroversion of the pelvis and flexion of the knees, in order to maintain the centre of gravity over the feet (6), the latter definition may lead to an underestimation of problems of sagittal posture, although the patient endures considerable discomfort. Moreover, this may lead to a delay in diagnosis of camptocormia until it develops into rigid kyphosis, which is more difficult to correct (3, 7). In general, diagnosis is made by subjective assessment of the patient’s posture, which in itself is unsatisfactory since the pathology may then be overestimated (2) and lead to confusion with physiological variations in posture (8–10), pain compensation (11, 12), natural kyphosis resulting from ageing (4, 6, 13–16), or natural forward inclination during walking (17–21).
Kyphosis originating from osteoporosis or from Scheuermann’s disease is known to induce discomfort and disability and is thought to increase the risk of falling in elderly patients (22, 23). By analogy with kyphosis, camptocormia is considered very disabling (24), although, to our knowledge, there is no study that has assessed its repercussions on gait.
The aim of this study was quantitatively to assess camptocormia by comparing clinical, radiographic and kinematic measurements of sagittal trunk anteflexion in patients with a sagittal postural imbalance under static and dynamic walking conditions, and to examine the functional repercussion of camptocormia on walking performance. We therefore designed a non-invasive, reliable and automated method to measure camptocormia quantitatively and establish the link between walking performance and the degree of severity of the pathology. Furthermore, by comparing 2 patient populations, i.e. idiopathic vs PD patients, we found that they expressed different motor profiles that were revealed by the dynamic assessment of bending during walking. The characteristic kinematic pattern of PD patients compared with idiopathic patients suggests that different physiopathological mechanisms are involved in camptocormia.
Material and methods
Patients
Forty-three subjects (28 females and 15 males; mean age 69 years (standard deviation (SD) 10 years)) were included in the study. Patients were initially referred to the orthopaedic medical unit of our hospital for camptocormia treatment. Once diagnosed with possible camptocormia according to usual subjective clinical criteria (some degrees of forward flexion of the thoraco-lumbar spine during walking that disappeared in the recumbent position), they were invited to participate in the study. Patients were excluded from the study, however, if they were not able to walk distances of more than 10 m without the help of another person or mobility equipment. The mean age for the idiopathic group was 69.4 years (SD 11.2) (n = 26) and 70.4 years (SD 6.8) (n = 17) for the Parkinsonian group. The mean duration of camptocormia onset was 2.02 years (SD 1.7) for the idiopathic group and 2.17 years (SD 1.3) for the Parkinsonian group. Each patient was tested for creatine phosphokinase (CPK) levels, and electromyography (EMG) recordings were not performed, since none of the patients had high levels of CPK. With regard to possible orthopaedic complications, none were found to have scoliosis or vertebral fractures. Therefore, although no definitive testing was performed to exclude significant myopathic or orthopaedic features, there were no clinical or historical findings to suggest a major contribution from these conditions. None of the patients presented orthopaedic complications or myopathy. The mean time since onset of PD was 10.4 years (SD 6.7). The patients were not rated according to the Unified Parkinson’s Disease Rating Scale (UPDRS) since orthopaedic physicians in general are not familiar with this type of evaluation. All patients with PD were being treated with L-DOPA (levodopa) and their level of disability was assessed by the Hoehn & Yahr scale and ranged from 1.5 to 4 (median 3, quartile 2; mean 2.9 (SD 0.95)). They were hospitalized for 4 weeks in our rehabilitation unit and the daily fluctuation with L-DOPA was evaluated during the first week. Within the patient cohort there were no subjects with large fluctuations; in any case, the off periods were observed only in the afternoon, while experiments were carried out in the morning. The patients were also treated with dopamine agonists. While dopamine agonists may induce antecollis (11), none of the patients in the current study exhibited this feature, and due to the early onset of camptocormia (mean 2.17 years (SD 1.3) this hypothesis was not explored.
Study design
The subjects gave their written informed consent and the experimental procedures were approved by the local ethics committee, the “Comité de protection des personnes Bordeaux A nu 2005/46”, and were in accordance with the ethics standards of the Declaration of Helsinki. The patients were asked to attend a morning of clinical, radiological and kinematic evaluation in the following 30 days. For clinical assessment, trunk inclination was first measured for 10 s in the natural self-adopted posture where the patients were asked to adopt their usual inclination, and then to straighten up with or without the help of their hands. Lateral radiographs of the whole spine were obtained with the EOS system as usual, with hands on clavicles and without any specific order being given (25–27). During kinematic analysis, trunk inclination was first measured for 10 s in a static position and with a natural self-adopted posture, then in a straightened-up position without the help of the hands. Secondly, trunk inclination was established under dynamic conditions during walking. In this condition, the patients were evaluated with an optoelectronic system (ELITE, BTS, Milano, Italy) for kinematic acquisition. The system consists of 8 infra-red cameras (100 Hz sampling rate, accuracy < 1 mm) that track the motion of passive reflective markers. Synchronized acquisition and data processing were performed with BTS Biomech software. The patients were equipped with reflective markers on their limbs in order to measure gait cycle parameters. They were requested to walk continuously along a closed-loop trajectory (total distance 20 m) as many times as possible (for a maximum of 10 min) and inclination was measured in a recording area (3 m long) during each passage.
Parameters
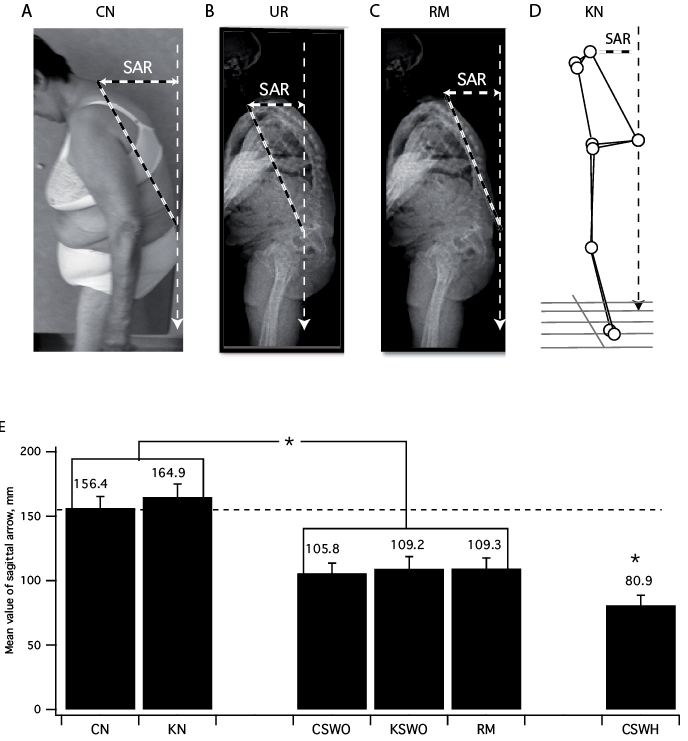
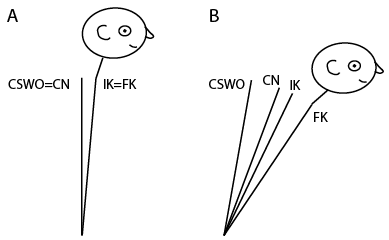
Two visual markers detectable by X-rays and the kinematic system were initially positioned on the patients. They were kept attached to the skin throughout the evaluation so that the same references could be employed under clinical, radiological and kinematic conditions. The first marker was positioned on the spinous process of C7, while the second marker was positioned in the middle of the segment linking the 2 Venus dimples in order to project horizontally to S1. Clinical sagittal inclination was determined by C7 sagittal arrow (C7-SAR) (28), provided indirectly by the horizontal distance between the C7 and S1 markers (Fig. 1A) in a natural self-adopted position (“Clinical Natural”; CN), in a straightened-up position without help (CSWO) and in a straightened-up position with the help of the subject’s hands (CSWH). The ability of patients to maintain their natural self-adopted posture for a period of 10 min was tested specifically on a different group of patients (n = 7). There was virtually no change in the C7-SAR when the patients remained immobile; the mean C7-SAR was 196 ± 1.4 mm (standard error of the mean; SEM) at time 0, and 20.1 ± 1.4 mm (SEM) at 10 min. As described previously (29), radiological inclination was determined on the lateral whole spine by measuring either the horizontal distance from the centre of C7 to the posterior corner of the sacrum (vertebral radiological value, Fig. 1B), or the horizontal distance between the C7 marker and the S1 marker (“marked” radiological value, Fig. 1C). These 2 values were obtained in order to be able to correlate usual radiographic assessment (UR) and assessment with markers (RM). Kinematic inclination was indirectly assessed by measuring the distance between the C7 marker and the S1 marker (Fig. 1D), in a natural standing position for 10 s (KN), in a straightened-up position without assistance (KSWO), and during walking. In the present study we examined the C7 sagittal arrow instead of the angle of trunk inclination that is usually reported in radiological analyses, in order to collect comparable data values in all 3 conditions (clinical, radiological and kinematic). In all cases, we found that the sagittal angle and the sagittal arrow values were highly correlated (0.98, p < 0.0001). On this basis, therefore, we considered the latter values alone, as is normally the case in clinical assessment and also for the purpose of simplicity: unlike the 2 measurements required for angle calculations, an arrow value is only a single measurement (30). Furthermore, measuring height requires precise positioning, both at the C7 and sacral levels.
Analysis
Data were processed offline with MATLAB software. Correlations were performed with Pearson’s test and comparisons between different values were made with the non-parametric test for multiple comparisons of Bonferroni with SAS software (Cary, NC, USA). For the multiple correlation analyses between performance parameters and C7-SAR values, a correction function was applied to significance levels with the Holm-Bonferroni method (Anastats, France). The coefficient of variation (CV), known as “relative variability”, was determined by the SD divided by the mean and expressed as a percentage. Unless otherwise specified, values are given as mean ± SEM and were considered to be significantly different at p < 0.05.
Results
Of the 43 patients included in the study, 17 had PD and 26 were initially diagnosed as having idiopathic camptocormia. As reported by patients during the initial consultation, the mean time from onset of trunk discomfort was 3 years (SD 2.8) (for all patients) and they have been referred to the hospital because their trunk posture had worsened during the preceding year.
C7-SAR mean values collected under the 2 different radiological conditions (usually radiographic assessment (UR) and assessment with markers (RM), Fig. 1B–C) did not present any significant differences (101 mm (SD 11) and 109 mm (SD 11), respectively, p > 0.05) and were highly correlated (r = 0.97; p < 0.0001). Therefore, in the course of this study we compared RM values with C7-SAR values collected under the other conditions (Fig. 1E). For comparable conditions, there was virtually no difference according to the measurement modality. Mean C7-SAR values were very similar when the subjects stood in their “natural” position (clinical assessment, CN, and kinematic assessment, KN, 156.4 mm (SD 9) and 164.9 mm (SD 10), respectively). When the patients straightened up on their own without using their hands (clinical assessment, CSWO and kinematic assessment, KSWO) or were straightened up by the measurement method (radiographic assessment with markers, RM), there was a significant reduction in C7-SAR values. This decrease was still more obvious when the patients pushed with their hands on their thighs (CSWH). Table I presents the correlation matrix for C7-SAR values assessed under the various methods. They were all highly and significantly correlated. Altogether, these results indicate that the C7-SAR can be consistently assessed by various methods, including kinematic measurements under static conditions.
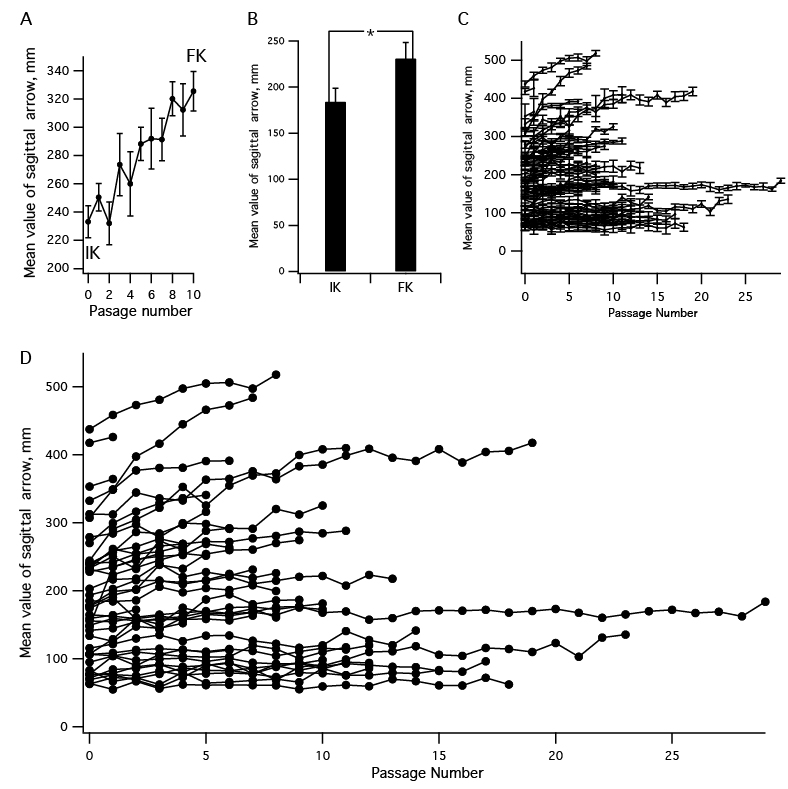
Next we evaluated the changes in C7-SAR values over time during walking. The mean ± SEM distance that the patients were able to walk was 214 ± 18 m, with a mean of 11 ± 1 passages through the recording area. The mean number of recorded gait cycles in each passage was 6.1 ± 0.1. For each patient, we compared the speed with the passage number and did not find any consistent relationship, with only 8 of the 43 patients expressing a significant change in their walking speed with time, although 2 of them produced a speed increase rather than decrease. During each passage, we calculated the mean C7-SAR value by using kinematic analysis (Fig. 1D). Fig. 2A presents the changes in C7-SAR values over time during all passages for a typical subject. The minimum C7-SAR value during the first passage was termed the initial kinematic position (IK), while the maximum value during the last passage provided the final kinematic position (FK). There was a dramatic increase in values with time, indicating that patients drooped progressively during walking. Fig. 2B shows the mean IK and FK values for the whole cohort studied (n = 43) and indicates that there was a significant increase in C7-SAR during walking. FK values were significantly correlated with IK values (r = 0.95; p < 0.0001) and with the other C7-SAR values (Table I).
|
Table I. Correlations between C7 sagittal arrow (C7-SAR) values measured under different methods and conditions |
||||||||||||
|
C7-SAR under static conditions |
C7-SAR under dynamic conditions |
|||||||||||
|
Natural self-adopted posture |
Radiological |
Straighten up with or without hand help |
||||||||||
|
CN |
KN |
RM |
UR |
CSWO |
KSWO |
CSWH |
IK |
FK |
||||
|
CN |
0.89** |
0.79** |
0.81** |
0.92** |
0.88** |
0.85** |
0.84** |
0.56** |
||||
|
KN |
0.89** |
0.81** |
0.83** |
0.87** |
0.93** |
0.82** |
0.93** |
0.52** |
||||
|
RM |
0.79** |
0.81** |
0.97** |
0.78** |
0.83** |
0.74** |
0.8** |
0.57** |
||||
|
UR |
0.81** |
0.83** |
0.97** |
0.78** |
0.82** |
0.72** |
0.81** |
0.53** |
||||
|
CSWO |
0.92** |
0.87** |
0.78** |
0.78** |
0.92** |
0.92** |
0.87** |
0.51** |
||||
|
KSWO |
0.88** |
0.93** |
0.93** |
0.82** |
0.92** |
0.91** |
0.91** |
0.53** |
||||
|
CSWH |
0.85** |
0.82** |
0.74** |
0.72** |
0.92** |
0.91** |
0.85 |
0.47** |
||||
|
IK |
0.84** |
0.93** |
0.8** |
0.81** |
0.87** |
0.91** |
0.85 |
0.57** |
||||
|
FK |
0.56** |
0.52** |
0.57** |
0.53** |
0.51** |
0.53** |
0.47** |
0.57** |
||||
|
CN: clinical assessment in natural self-adopted posture; CSWH: clinical assessment in straighten-up with hand self-help; CSWO: clinical assessment in straighten-up without hands; FK: kinematic assessment for final position during walking; IK: kinematic assessment for initial position during walking; KN: kinematic assessment in natural self-adopted posture; KSWO: kinematic assessment in straighten-up without hands; RM: radiographic assessment with markers; UR: usual radiographic assessment. |
||||||||||||
Fig. 2C presents changes in C7-SAR values for all patients over time. To enable a detailed view of individual profiles, the same data are presented in Fig. 2C, but without including the SD for the sake of clarity. Only 1 patient was able to walk for the total duration of the test (10 min), performing 30 passages, whereas others walked for a single loop only. Although at first sight the patient sagittal profiles illustrated in Fig. 2D might suggest the existence of different behavioural subsets, an analysis of the relative (percentage) increase rather than of changes in absolute values failed to reveal any significant differences between subjects with low or higher IK values.
We further investigated the relationship between posture and its detrimental effect on walking performance, which was estimated by 2 parameters: mean walking speed and walking duration (the latter providing an index of locomotor endurance). The 2 parameters were significantly correlated (R = 0.4, p < 0.003): patients who walked faster also walked for longer periods. An analysis of the relationship between C7-SAR measurements and walking performance (Table II) indicated that the walking duration was solely correlated significantly with IK (–0.38, p < 0.05). Speed was best correlated with IK (–0.5, p < 0.05), but was also correlated with other static clinical and kinematic measurement values (p < 0.05). Surprisingly, however, RM (or UR) did not significantly correlate with either walking speed or duration. Altogether, these results suggest that IK was the most relevant parameter in providing clues about the functional alterations expressed during walking.
|
Table II. Correlations between C7 sagittal arrow (C7-SAR) values measured under different methods and performance |
||||||||||||||
|
C7-SAR under static conditions |
C7-SAR under dynamic conditions |
Performance |
||||||||||||
|
Natural self-adopted posture |
Radiological |
Straighten up with or without hand help |
Walking duration |
Speed |
||||||||||
|
CN |
KN |
RM |
UR |
CSWO |
KSWO |
CSWH |
IK |
FK |
||||||
|
Walking duration, total Walking duration, idiopathic Walking duration, Parkinson’s disease |
–0.3 –0.09 –0.09 |
–0.24 –0.05 –0.05 |
–0.29 –0.16 –0.16 |
–0.3 –0.18 –0.05 |
–0.29 –0.1 –0.1 |
–0.26 –0.03 –0.032 |
–0.26 –0.05 –0.05 |
–0.38* –0.25 –0.25 |
–0.27 –0.14 –0.14 |
0.44* 0.49 0.44 |
||||
|
Speed, total Speed, idiopathic Speed, Parkinson’s disease |
–0.36 –0.41 –0.41 |
–0.4* –0.47 –0.39 |
–0.2 –0.48 –0.15 |
–0.2 –0.43 –0.05 |
–0.44* –0.37 –0.57 |
–0.4* –0.42 –0.46 |
–0.45* –0.37 –0.61 |
–0.5* –0.52 –0.56 |
–0.15 –0.49 –0.18 |
0.44* 0.49 0.44 |
||||
|
CN: clinical assessment in natural self-adopted posture; CSWH: clinical assessment in straighten-up with hand self-help; CSWO: clinical assessment in straighten-up without hands; FK: kinematic assessment for final position during walking; IK: kinematic assessment for initial position during walking; KN: kinematic assessment in natural self-adopted posture; KSWO: kinematic assessment in straighten-up without hands; RM: radiographic assessment with markers; UR: usual radiographic assessment. |
||||||||||||||
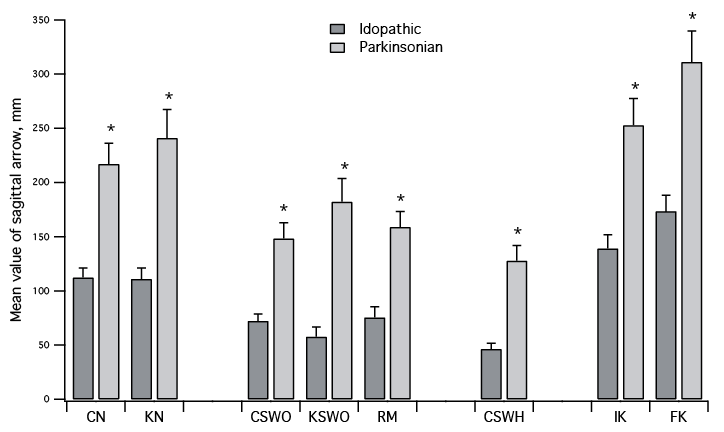
We next attempted to identify factors that could explain the inter-individual variability observed during walking. As our population included a significant proportion of patients with PD, we examined whether the 2 sub-populations displayed behavioural differences. In a first instance, however, the mean speed values of patients with PD and the idiopathic group were not significantly different (0.72 m/s (SD 0.04) and 0.67 m/s (SD 0.08), respectively). We then compared the C7-SAR values of PD and idiopathic patients. Fig. 3 indicates that, for all measurements performed, the PD population systematically had significantly higher C7-SAR values under static conditions. During walking, the increase in trunk inclination was also significantly higher in the PD group than in the idiopathic camptocormia group. We further compared a subset of patients (n = 8), in which the mean IK value was similar in the 2 groups (idiopathic 211.9 mm (SD 19.4); PD 207.8 mm (SD 19)). There was also no significant difference in the FK values (idiopathic 264 mm (SD 22.4); PD 263.5 mm (SD 29.8)) between these 2 groups. The worsening in dynamic anteflexion was not specific to the PD patients, but rather was linked to the severity of the initial anteflexion. Neither the Hoehn & Yahr patients’ score, nor PD onset or camptocormia onset were correlated with walking duration, speed, or any measurement of forward flexion (r < 0.1). When examining the 2 populations separately to explore the relationship between posture and its detrimental effect on walking performance (Table II), we did not find any significant correlations, probably due to sample size.
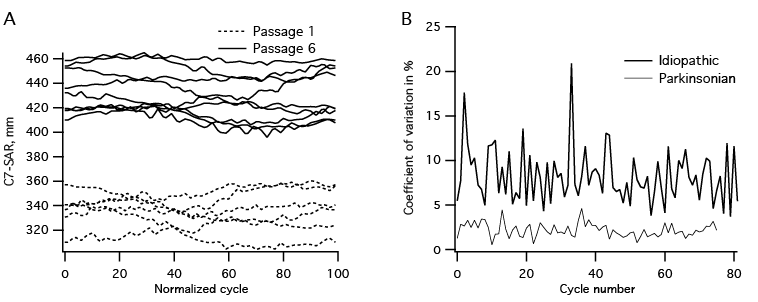
A detailed analysis of individual walking cycle characteristics revealed additional differences between the PD and idiopathic patients. For this purpose, we assessed the changes occurring in C7-SAR values during normalized cycles of walking. In Fig. 4A, the dashed and solid lines represent C7-SAR values (sampling frequency 100 Hz) in successive cycles during passages 1 and 6, respectively. As previously reported, we noted a very clear increase in C7-SAR values from the first to the last passage, together with changes related to pitch movements during each cycle. When calculating the instantaneous changes occurring in C7-SAR values, there were striking differences between patients with PD and the idiopathic population. Fig. 4 shows the C7-SAR coefficient of variation within each successive cycle for a typical idiopathic subject (black line) and for a typical patient with PD. There was a noticeable difference that remained throughout the walking task, with a much greater mean coefficient of variation in idiopathic patients (6.3% (SD 0.8)), which was highly significantly different (p < 0.001) from the mean coefficient of variation of patients with PD (2.6% (SD 0.4)). These data thus indicate that, during walking, the behaviour of patients with idiopathic camptocormia is different from that of patients with PD.
Discussion
This study presents a new method for assessing sagittal posture under walking conditions in patients with camptocormia (bent spine syndrome). We first validated this methodology by comparing it with classical clinical and radiological techniques. Our finding also establishes a clear relationship between C7-SAR values evaluated indirectly under dynamic conditions and the functional impairment observed during walking. In addition, the data suggest that the usual assessment of C7-SAR by radiological measurement does not correlate with functional impairment. Finally, we show that patients with PD behave differently from idiopathic patients and conclude that recording sagittal inclination during walking is a much more accurate way to disclose the detrimental effects of camptocormia and that it mimics more realistically what actually occurs during daily life.
Methodological considerations
Studies that measure sagittal posture are classically based on radiological measurements under various static positions (26). In the present study, we first compared C7-SAR values as an index of camptocormia using several techniques under the various static conditions generally used for diagnosing camptocormia (Fig. 1E). First, we demonstrate that the clinical, radiological and kinematic data thus obtained are strongly correlated and provide similar mean estimates of anteflexion. Secondly, we found that radiological data collected with cutaneous markers (RM) like those used for kinematic or clinical analysis were also strongly correlated with the usual radiological references (UR). Interestingly, there was no difference between C7-SAR values assessed by the radiological marker method (RM) and with the clinical or kinematic straightened-up position (CSWO and KSWO, respectively; Fig. 1E). This suggests that the radiological measurement technique is likely to possess a potential pitfall by measuring only the straightened-up position. Using the straightened-up position alone could in turn lead to a bias in the therapeutic evaluation of treatments such as braces, which are currently used for correcting sagittal posture during walking.
The C7-SAR measurement, as performed in the present study, clearly presents some advantages compared with other methods, such as the measurement of forward flexion angle or measurements obtained from instruments such as the spinal mouse (Idiag, Fehraltdorf, Switzerland). As indicated above (see Material and Methods), the arrow value requires a single measurement only (28), while the sagittal angle demands 2 measurements for angle calculations. Since the 2 values are highly correlated (0.98, p < 0.0001), the C7-SAR may be preferable because it is simpler. Furthermore, kinematic measurement of the C7-SAR as performed in the present study, is the only way dynamically to describe the changes that occur during locomotion and is complementary to other devices, such as the spinal mouse (Idiag, Fehraltdorf, Switzerland), which can only be used for static posture measurements.
Definition of camptocormia according to dynamic criteria
To our knowledge, this is the first study of its kind performed on camptocormia under dynamic conditions, in contrast to previous studies, which, to date, have measured the severity of the pathology only under static conditions (4, 5, 7, 31). This new approach using kinematic measurements highlights the worsening of trunk anteflexion during walking, which is one of the main criteria for defining camptocormia (1). However, the trial duration (i.e. 10 min, see Material and Methods) employed here was too long, since only 1 patient was able to walk for the 10 min maximum, suggesting that the duration could be reduced in routine practice.
In non-pathological adult subjects, the C7-SAR is close to 0 mm (4, 9, 13, 14) and is not modified with advancing age (6). Based on previous studies (17–21), it was possible to calculate that, during walking, the natural increase in trunk inclination ranges from 9 to 52 mm. Altogether, our data suggest that camptocormia transposes into the addition of anteflexion that progressively arises during the walking process, i.e. abnormal straightened-up posture + abnormal upright spontaneous posture + inclination during walking initiation + worsening during walking (Fig. 5).
The various parameters that we measured using different methods are all correlated (Table I). Furthermore, they are correlated with the functional impairment endured by patients, i.e. diminishing both walking speed and duration, except for RM. Therefore, the most important index is the value of the initial C7-SAR position (IK) at the beginning of the walking trial. In comparison with the other static parameters, IK is the posture that the patient adopts spontaneously at the beginning of walking, corresponding to the addition of the C7-SAR expressed in a natural self-adopted position and the inclination required for walking (Fig. 5). We conclude that kinematic quantification, which is simple and inexpensive, is reliable and may be used more efficiently than radiological data to assess the severity of camptocormia. Moreover, since the technique is non-invasive, it can be recommended for the therapeutic follow-up of populations with high potential risk of developing camptocormia, such as patients with PD and elderly people (32).
As stated above, a surprising result of the present study was the relative weakness of radiological measurement as an indicator of functional impairment. A possible explanation provided by comparing the various conditions tested here (Fig. 1E) is that RM is not representative of a natural posture, but only measures a straightened-up posture, as indicated by the fact that mean RM values were similar to those obtained by clinical (CSWO) and kinematic (KSWO) assessment of straightened-up positions. This elongated position is likely to be a consequence of the radiological methodology. Even if radiography does not have a predictive value for functional impairment as measured in the present study, it has been shown that a C7-SAR > 60 mm determined by radiography becomes uncomfortable (33, 34).
Parkinsonian camptocormia exhibits specific features
PD is a leading cause of camptocormia (2). In the present study, in which the patients with PD represented 40% of the total population studied, camptocormia was more pronounced in the former in all conditions (Fig. 3). This may be due to several factors that have been proposed to explain camptocormia in patients with PD, such as subjective visual vertical disturbances (35), myositis of the erector spinae (2), anterior dystonia (5, 36–38) and negative posterior dystonia (39). That these patients were less able to straighten up than the idiopathic patients (compare clinical assessment in straighten up with hand self-assistance, CSWH values in Fig. 3) indicates that anterior dystonia or acquired kyphosis may be implicated. Another interesting feature is that patients with PD do not express any postural variability during the walking cycle (Fig. 4). Currently, only speculation can be made to explain this behavioural difference. For example, possible differences in stepping dynamics could be the cause of the differences in trunk dynamics. Another explanation could be that during walking, patients with PD do not attempt to correct their posture, unlike idiopathic patients who are continuously attempting to straighten up. The lack of postural adjustment in subjects with PD may be due not only to the greater fatigability of the erector spinae induced by myopathy, but also to a negative dystonia of these muscles or to an anterior dystonia. In any case, further experiments are required to resolve this issue.
AcknowledgEments
The authors warmly thank John Simmers for correcting the English in this paper. This work was funded in part by the “Fondation pour la Recherche Médicale”.
References

