Christian Geroin, PT1*, Stefano Mazzoleni, PhD3*, Nicola Smania, MD1,2, Marialuisa Gandolfi, MD, PhD1, Donatella Bonaiuti, MD4, Giulio Gasperini, MD5, Daniele Munari, PT1, Patrizio Sale, MD, PhD6, Andreas Waldner, MD7, Raffaele Spidalieri, MD8, Federica Bovolenta, MD9, Alessandro Picelli, MD1, Federico Posteraro, MD10, Franco Molteni, MD5, Marco Franceschini, MD6 and the Italian Robotic Neurorehabilitation Research Group (IRNRG)
From the 1Neuromotor and Cognitive Rehabilitation Research Centre (CRRNC), Department of Neurological and Movement Sciences, University of Verona, 2Neurological Rehabilitation Unit Azienda Ospedaliera-Universitaria Integrata Verona, 3The BioRobotics Institute, Scuola Superiore Sant’Anna, Pisa, 4Physical Medicine and Rehabilitation Department, S. Gerardo Hospital, Monza, 5Department of Rehabilitation Medicine, Ospedale Valduce, Villa Beretta, Costamasnaga, Lecco, 6Department of Rehabilitation IRCCS San Raffaele Pisana, Rome, 7Department of Neurological Rehabilitation, Private Hospital Villa Melitta, Bolzano, 8Istituto di Riabilitazione Neurologica “Madre Della Divina Provvidenza” di Agazzi, Arezzo, 9Medicine Rehabilitation NOCSAE Hospital AUSL of Modena, Modena and 10Neurological Rehabilitation Unit, Auxilium Vitae Rehabilitation Center, Volterra, Italy. *Both authors contributed equally to this work.
OBJECTIVE: The aim of this systematic review was to identify appropriate selection criteria of clinical scales for future trials, starting from those most commonly reported in the literature, according to their psychometric properties and International Classification of Functioning, Disability and Health (ICF) domains.
DATA SOURCES: A computerized literature research of articles was conducted in MEDLINE, EMBASE, CINALH, PubMed, PsychINFO and Scopus databases.
STUDY SELECTION: Clinical trials evaluating the effects of electromechanical and robot-assisted gait training trials in stroke survivors.
DATA EXTRACTION: Fifteen independent authors performed an extensive literature review.
DATA SYNTHESIS: A total of 45 scales was identified from 27 studies involving 966 subjects. The most commonly used outcome measures were: Functional Ambulation Category (18 studies), 10-Meter Walking Test (13 studies), Motricity Index (12 studies), 6-Minute Walking Test (11 studies), Rivermead Mobility Index (8 studies) and Berg Balance Scale (8 studies). According to the ICF domains 1 outcome measure was categorized into Body Function and Structure, 5 into Activity and none into Participation.
CONCLUSION: The most commonly used scales evaluated the basic components of walking. Future studies should also include instrumental evaluation. Criteria for scale selection should be based on the ICF framework, psychometric properties and patient characteristics.
Key words: stroke; lower limb; rehabilitation; motor recovery; robot; training; therapy; physiotherapy; function; study; robot- assisted, trial.
J Rehabil Med 2013; 45: 987–996
Correspondence address: Christian Geroin, Neuromotor and Cognitive Rehabilitation Research Centre (CRRNC), Department of Neurological, and Movement Sciences, University of Verona, 37134 Verona, Italy. E-mail: christian.geroin@univr.it
Accepted Jun 17, 2013; Epub ahead of print XXX?, 2013
Introduction
Stroke is a leading cause of disability (1, 2). Among areas with population-based studies, the overall age-standardised incidence of stroke in people aged ≥ 55 years range from 4.2 to 11.7 per 1,000 person-years (1). Approximately 64% of stroke survivors have persisting sensorimotor deficits leading to progressive upper and lower limb disability (3), which restricts their autonomy in activities of daily living (ADLs). Recovery of walking is one of the main objectives in stroke rehabilitation, which contributes to an improvement in independence (4).
Conventional rehabilitation has been proven, to some extent, to be effective in improving walking function; however, it often requires great physical effort by physiotherapists (4). In recent years, several innovative technologies and strategies have been proposed to overcome this difficulty and improve walking function (4–6). According to the modern concept of task-specific training, electromechanical and robotic-assisted gait training, in combination with conventional rehabilitation, has been shown to be feasible and effective to improve walking in stroke survivors (4, 5), even facilitating repetitive practice of gait-like movement in individuals who are wheelchair users. Although research regarding these neurorehabilitation approaches is growing, literature concerning specific outcome measures is scant (7).
The evaluation of treatment outcomes is a key factor in both clinical rehabilitation practice and research settings, but there is no agreement on the most appropriate modality to select outcome measures (7–10). Three main limitations can be identified. First, a large number of instruments is available, but they have poor psychometric properties. Secondly, there is no shared consensus on specific clinical outcome measures that should be used to assess the effects of electromechanical and robot-assisted gait training trials (ERAGTT). Finally, the outcome measures regarding the evaluation of recovery of function and compensation adaptation processes, which strongly affect the patient’s involvement in ADLs, are often unclear and misinterpreted (11, 12).
Choosing a suitable scale to assess sensorimotor recovery is a challenging issue in rehabilitation, given that several constraints could interfere with their appropriate selection (10). For instance, the domain to be measured (e.g. function, activity, quality of life), clinical area (e.g. neurological, geriatric), setting (e.g. hospital, community, home), as well as psychometric properties (e.g. reliability, validity, responsiveness) could interfere with the selection of the most appropriate outcome measures.
The aim of this systematic review is to identify appropriate selection criteria of clinical scales for future trials, starting from those most commonly used in the literature, according to their psychometric properties and International Classification of Functioning, Disability and Health (ICF) domains.
Material and Methods
The systematic review was performed by the authors in 3 stages, as described below, according to the methodology reported by Sivan et al. (7).
Stage 1: Search for clinical trials involving electromechanical and robot-assisted gait training in patients after stroke and determine the outcome measures used in each trial
Data sources. A search of MEDLINE, EMBASE, CINALH, PubMed, PsychINFO and Scopus databases was performed to identify relevant ERAGTT. The keywords used were: stroke, lower limb, rehabilitation, motor recovery, robot, training, therapy, physiotherapy, function, study, robot-assisted and trial. From the initial search, all abstracts were reviewed.
Study selection. Inclusion criteria were: (i) studies published from January 2000 to January 2012; studies involving participants with diagnosis of a stroke; (ii) lower limb exercise assisted by a robot device. A robotic device was defined as any technology able to assist the patient’s limb movement for therapeutic exercises, to support the therapist during administration of programmable and customized rehabilitation programmes and composed of mechanical structure with actuators and energy supply; (iii) at least one scale used in the study.
The exclusion criteria were: (i) studies involving a robotic orthosis device; (ii) studies enrolling only healthy volunteers; and (iii) articles published in languages different from English.
Data extraction. Multiple independent investigators performed the article selection as follows: 15 investigators carried out an extensive literature review and selected the studies according to the inclusion criteria; NS, FP, GG, FM and PS independently read in detail all the selected articles; MG, AW, RS, FB and AP reviewed the same articles and listed the scales used; DB, DM, MF, CG, SM performed a review based on the psychometric properties of the different scales; CG, SM and MG drafted the manuscript. Disagreements were resolved by discussion between authors. All authors have read, edited and agreed on the contents of the manuscript.
In this review the term “scale” was used to define the assessment instrument used as a discriminative or predictive tool in ERAGTT. Discriminative scales are used to cluster patients into homogeneous groups for treatment studies (10). Predictive scales are used to predict how the motor recovery will evolve over time. The term “outcome measure” was used to define the evaluative instruments that reflect clinically important changes after intervention (10). Evaluative instruments are used to estimate the quantity of longitudinal change in an individual or group of patients who underwent the rehabilitation intervention (10).
Stage 2. List and classify the scales collected during stage 1 according to the ICF domains
The content of each scale identified in Step 1 was classified in terms of the ICF categories, according to literature classification and specific website research (9, 13, 14). When necessary, the scale classification was discussed between authors. Three categories were identified as follows:
• Body functions and structures: functions refer to physiological functions of body systems including psychological. Structures are anatomical parts or regions of the body and their components. Impairments are defined as problems or disorders in body function or structure (9).
• Activity: activity refers to execution of a task by an individual. Limitations of a task are defined as difficulties an individual might experience in completing a given activity (15).
• Participation: involvement of an individual in a life situation. Restrictions to participation describe difficulties experienced by the individual in a life situation or role (16).
• Contextual factors: which include environmental and personal factors that may influence the relationship among different factors (16).
Stage 3. Describe the measurement properties of the identified scales in patients after stroke
A literature search of the psychometric properties of each scale was performed. The reliability, validity and responsiveness of each scale were investigated. The score for each property was identified as high or excellent (+++), moderate (++) or poor (+) (16, 17).
Moreover, minimal clinically important difference (MCID), floor and ceiling effect, time of administration and level of measurement (nominal, ordinal, interval and ratio) for each scale were evaluated. Table I describes the definition and standards values of the psychometric properties considered. A further classification of the scales used in the trials according to phase of disease was performed.
|
Table I. Definition and standard values for the evaluation criteria. (Modified with permission from ref 7) |
||
|
Properties |
Definition of the properties |
Standard values |
|
Reliability |
Reproducibility of an outcome measure is defined as the amount of the score that includes information about the characteristic of interest opposite to measurement error (10). Reliability can be evaluated in 3 basic ways: (i) test-retest reliability; (ii) inter-rater reliability; and (iii) internal consistency reliability (10). |
Test-retest or inter-rater reliability (Icc; kappa statistics): excellent: ≥ 0.75; adequate: 0.4–0.74; poor: ≤ 0.40. A minimum test-retest reliability of 0.90 is recommended whether the measure is performed during the ongoing progress of a subject undergoing treatment (15). Internal consistency (split-half or Cronbach’s α statistics): excellent: ≥ 0.80; adequate: 0.70–0.79; poor: < 0.70 (15). |
|
Validity |
Validity is the faculty of a scale to measure what it is intended to measure. Many types of validity exist in literature, e.g. face, content, discriminative, convergent, predictive, and criterion. The most important are criterion and predictive validity (10). |
Construct/convergent and concurrent correlations: excellent: ≥ 0.60; adequate: 0.31–0.59; poor: ≤ 0.30. ROC analysis – AUC: excellent: ≥ 0.90; adequate: 0.70–0.89; poor: < 0.70. No agreement on ideal values by which to judge sensitivity and specificity as a validity index (15). |
|
Responsiveness |
Responsiveness is sensitivity to changes within patients over time, which could be indicative of therapeutic effects. Minimal clinically important difference (MCID) is the smallest score difference in the domain of interest that patients perceive as beneficial (10). Floor and ceiling indicate limits to the range of evident modification beyond which no further improvement or worsening can be detected (10). |
Sensitivity to change: excellent: with standardized effect sizes: < 0.5 = small; 0.5–0.8 moderate; ≥ 0.8 = large. Further available methods are: Standardized Response Mean (SRM), ROC Analysis – Area Under Curve (AUC), Statistical Significance p-value, correlation values of observed change compared to change in other scales, MCID described as a score value (7). Adequate: evidence of moderate/less change than expected; contradictory evidence. Poor: feeble evidence based solely on p-values (statistical significance). Floor/ceiling effects: excellent: no floor or ceiling effects; adequate: floor and ceiling effects < 20%; poor: > 20% (15). |
|
Acceptability |
Acceptability can be divided into respondent and administrative burden. Respondent refers to whether the length and content are acceptable to the intended participants (e.g. stroke individuals). Administrative refers to whether the tool is user-friendly, easy to understand and cheap (7). |
Respondent burden: optimal – time to administration less than 15 min and easy to understand; adequate –longer or some problems of acceptability; poor – problems of acceptability and lengthy (7). Administrative burden: optimal when score is immediately obtained and easy to understand; adequate when score requires interpretation by computer; and poor when score is complex and expensive to be detected (7). |
|
ROC: receiver operator characteristic; AUC: area under curve; ICC: intraclass correlation coefficient. |
||
Results
Stage 1
A total of 27 studies published from 2000 to 2012 (involving 966 subjects) fulfilled the inclusion criteria for the review. A total of 45 scales was identified. The list of the scales used in these studies and the corresponding abbreviations are provided in Table II. Details regarding the type of electromechanical or robot device, authors, number and type of patients and the scales used are provided in Table III. The most common outcome measures used were: Functional Ambulation Category (FAC; 18 studies); 10-Meter Walking Test (10MWT; 13 studies); Motricity Index (MI; 12 studies); 6-Minute Walking Test (6MinWT; 11 studies); Rivermead Mobility Index (RMI; 8 studies); and Berg Balance Scale (BBS; 8 studies). The scales reported in Table III considered as “others” represent a mix of discriminative, evaluative and predictive scales.
|
Table II. Abbreviations for the scales |
|
|
Abbreviation |
Scales |
|
2MinWT |
2-Minute Walking Test (18) |
|
3MinWT |
3-Minute Walking Test (19) |
|
5MWT |
5-Meter Walking Test (20) |
|
6MinWT |
6-Minute Walking Test (21) |
|
8MWT |
8-Meter Walking Test (19) |
|
10MWT |
10-Meter Walking Test (22) |
|
AS |
Ashworth Scale (23) |
|
BBS |
Berg Balance Scale (24) |
|
BI |
Barthel Index (25) |
|
BMI |
Body mass index (26) |
|
CES-D |
Center for Epidemiological Studies-Depression Scale (27) |
|
CNS |
Canadian Neurological Scale (28) |
|
EMS |
Elderly Mobility Scale (29) |
|
ESS |
European Stroke Scale (30) |
|
FAC |
Functional Ambulation Category (8) |
|
FAI |
Frenchay Activities Index (31) |
|
FIM |
Functional Independence Measure (32) |
|
FM motor |
Fugl-Meyer Motor Subscale (33) |
|
FMA |
Fugl-Meyer Assessment of Sensorimotor Recovery After Stroke (33) |
|
HR |
Heart rate |
|
LLFDI |
Late Life Function and Disability Instrument (34) |
|
MAS |
Modified Ashworth Scale (23) |
|
MEFAP |
Modified Emory Functional Ambulation Profile (20) |
|
MI |
Motricity Index (35) |
|
MMAS |
Modified Motor Assessment Scale (36) |
|
MMSE |
Mini Mental State Examination (37) |
|
MoAS |
Motor Assessment Scale (38) |
|
MRC |
Medical Research Council (39) |
|
MRS |
Modified Ranking Scale (40) |
|
NIHSS |
National Institutes of Health Stroke Scale (41) |
|
PROM |
Passive Range of Movement |
|
RMAS |
Rivermead Motor Assessment Scale (42) |
|
RMI |
Rivermead Mobility Index (43) |
|
RPE |
Borg Scale of Perceived Exertion (44) |
|
RS |
Rankin Scale (45) |
|
SAS |
Stroke Activities Scale (46) |
|
SF-36 |
Short Form Health Survey (47) |
|
SPPB |
Short Physical Performance Battery (48) |
|
SSS |
Scandinavian Stroke Scale (49) |
|
ST |
Step Test (50) |
|
TBS |
Tinetti Balance Scale (51) |
|
TCT |
Trunk Control Test (35) |
|
TGS |
Tinetti Gait Scale (20) |
|
TMS |
Toulouse Motor Scale (52) |
|
TUG |
Timed Up and Go Test (20) |
|
Instrumental measures |
|
|
JK |
Joint Kinematic |
|
STGP |
Spatio-temporal Gait Parameters |
|
Table III. Scales used in ERAGTT (classified by number of studies and year of publication) |
||||||||||
|
Electromechanical/ robotic device |
Reference |
n |
Type of patients |
Most commonly used outcome measures |
Others |
|||||
|
FAC |
10MWT |
MI |
6MinWT |
RMI |
BBS |
|||||
|
G-EO |
Hesse et al., 2010 (53) |
1 |
Subacute |
* |
* |
* |
BI |
|||
|
GT1 |
Conesa et al, 2012 (54) |
103 |
Subacute |
* |
* |
TBS, TGS |
||||
|
Morone et al., 2011 (55) |
48 |
Subacute |
* |
* |
* |
* |
* |
AS, BI, CNS, MMSE, RS, TCT |
||
|
Geroin et al., 2011 (56) |
30 |
Chronic |
* |
* |
* |
* |
* |
ESS, MMSE, STGP, MAS |
||
|
Peurala et al., 2009 (57) |
56 |
Subacute |
* |
* |
* |
* |
BI, BMI, HR, MMAS, MRS, RMAS, RPE, SSS |
|||
|
Maple et al., 2008 (58) |
54 |
Subacute |
* |
* |
* |
5MWT, BI, EMS, FIM, MMSE |
||||
|
Pohl et al., 2007 (59) |
155 |
Subacute |
* |
* |
* |
* |
* |
BI, MRC, PROM |
||
|
Dias et al., 2007 (52) |
40 |
Chronic |
* |
* |
* |
* |
* |
* |
BI, FM motor, MMSE, ST, TMS, TUG, MAS |
|
|
Tong et al., 2006 (60) |
46 |
Subacute |
* |
* |
* |
MMSE, 5MWT, EMS, FIM, BI |
||||
|
Peurala et al., 2005 (61) |
45 |
Chronic |
* |
* |
FIM, MRC, MMAS, RPE, SSS, postural sway (Force Plate), HR, FAC, MAS |
|||||
|
Werner et al., 2002 (62) |
30 |
Subacute |
* |
* |
RMAS, BI, MAS |
|||||
|
Hesse et al., 2001 (63) |
14 |
Chronic |
* |
* |
RMAS, EMG, STGP, MAS |
|||||
|
Hesse et al., 2000 (64) |
2 |
Subacute |
* |
RMAS, MAS |
||||||
|
Hesse et al., 2000 (65) |
2 |
Subacute |
* |
RMAS, MAS |
||||||
|
LK |
Chang et al., 2011 (66) |
37 |
Subacute |
* |
* |
FM motor, AC, CR, VR |
||||
|
Magagnin et al., 2010 (67) |
5 |
Chronic |
* |
BI, FIM, TCT, ECG |
||||||
|
Lewek et al., 2009 (68) |
19 |
Chronic |
MMSE, STGP, JK |
|||||||
|
Hidler et al., 2009 (69) |
63 |
Subacute |
* |
* |
* |
* |
5MWT, FAI, MoAS, NIHSS, SF-36, MMSE, CES-D, STGP |
|||
|
Schwartz et al., 2009 (70) |
67 |
Subacute |
* |
* |
2MWT, FIM, NIHSS, SAS, TUG |
|||||
|
Westlake et al., 2009 (71) |
16 |
Chronic |
* |
* |
FM motor, LLFDI, SPPB, STGP |
|||||
|
Hornby et al., 2008 (72) |
48 |
Chronic |
* |
* |
CES-D, FAI, MEFAP, MRC, MMSE, SF-36, STGP, MAS |
|||||
|
Mayr et al., 2007 (73) |
16 |
Mixed |
* |
* |
* |
AS, MRC, RMAS |
||||
|
Krewer et al., 2007 (74) |
10 |
Mixed |
BMI, HR, Energy expenditure |
|||||||
|
Husemann et al., 2007 (75) |
30 |
Acute |
* |
* |
* |
BI, FAC, MRC, STGP, MAS |
||||
|
AA |
Fisher et al., 2011 (19) |
20 |
Mixed |
3MWT, 8MWT, MMSE, TBS |
||||||
|
LH |
Freivogel et al., 2009 (76) |
2 |
Chronic |
* |
* |
* |
* |
* |
PROM, MAS |
|
|
CaLT |
Wu et al., 2011 (77) |
7 |
Chronic |
* |
* |
STGP, MMSE |
||||
|
*Used in trial; G-EO: G-EO System; GT1: Gait-Trainer GT1; LK: Lokomat; AA: Autoambulator; LH: Lokohelp; FAC: Functional Ambulation Category; 10MWT: 10-Meter Walk Test; MI: Motricity Index; 6MinWT: 6-Minute Walk Test; RMI: Rivermead Mobility Index; BBS: Berg Balance Scale; STGP: Spatiotemporal Gait Parameters; JK: Joint Kinematic; AC: aerobic capacity; CR: cardiovascular response; VR: ventilatory response; EMG: electromyography; ECG: electrocardiography; CaLT: novel cable-driven robotic gait training system. For other abbreviations, see Table II. |
||||||||||
Stage 2
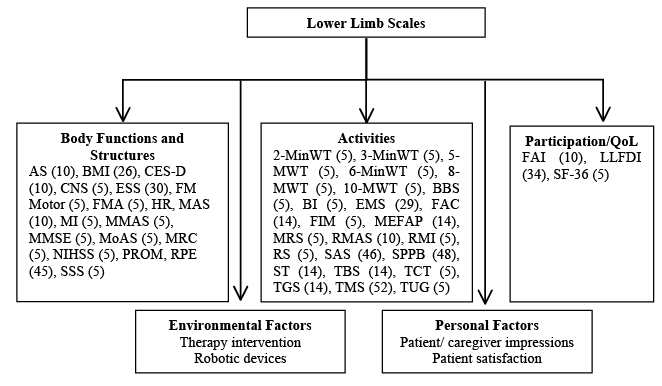
Each scale was classified into a single ICF domain, as shown in Fig. 1. Eighteen scales were classified into the body function domain, 24 scales into the activity and 3 into the participation.
Stage 3
The psychometric properties of the most commonly used outcome measures, based on the purpose of the measurement (10), are described in Table IV, whereas the levels of measurement according to Stevens (80) are reported in Table V (29 scales were ordinal, 12 ratio and 4 nominal). The classification of the scales used in the trials according to phase of disease is reported in Table VI (10 in the acute, 6 in chronic and 29 scales in both phases).
|
Table IV. Psychometric properties of the most commonly used outcome measures in electromechanical and robot-assisted gait training trials |
||||||
|
Characteristics |
FAC |
10MWT |
MI |
6MinWT |
RMI |
BBS |
|
Time taken (min) |
1 |
5 |
20 |
6 |
4 |
10–15 |
|
Number of items |
1 |
1 |
6 |
n/a |
15 |
14 |
|
Type |
1p |
Timed |
0–33p |
Meter |
2p |
4p |
|
Score range |
1–6 |
Varies |
0–33 |
Varies |
0–15 |
0–56 |
|
Test-retest reliability |
+++ |
+++ |
n/a |
+++ |
+++ |
+++ |
|
Inter-rater reliability |
+++ |
+++ |
+++ |
+++ |
+++ |
+++ |
|
Construct validity |
+++ |
+++ |
+++ |
+++ |
+++ |
+++ |
|
Responsiveness |
++ |
+++ |
n/a |
n/a |
+++ |
+++ |
|
MCID |
n/a |
0.16 m/s |
n/a |
50 m |
3 |
n/a |
|
Floor effect |
n/a |
n/a |
n/a |
n/a |
adeq |
adeq |
|
Ceiling effect |
n/a |
poor |
n/a |
n/a |
adeq |
adeq |
|
Burden |
adeq |
adeq |
adeq |
adeq |
adeq |
adeq |
|
References |
8 |
20, 78 |
35, 79 |
20 |
15, 20, 43 |
24 |
|
Scoring criteria as define in Table I. For abbreviations, see Table II. +++High/excellent; ++moderate; +low/poor; n/a: no available evidence yet; adeq: adequate (acceptable) floor/ceiling effect/burden; poor: poor (unacceptable) floor/ceiling effect/burden; nil: minimal/no burden; MCID: minimal clinically important difference. |
||||||
|
Table V. Scales classified according to levels of measurement (80) |
||||
|
Scales |
Nominal |
Ordinal |
Interval |
Ratio |
|
10MWT |
* |
|||
|
2MinWT |
* |
|||
|
3MinWT |
* |
|||
|
5MWT |
* |
|||
|
6MinWT |
* |
|||
|
8MWT |
* |
|||
|
AS |
* |
|||
|
BBS |
* |
|||
|
BI |
* |
|||
|
BMI |
* |
|||
|
CES-D |
* |
|||
|
CNS |
* |
|||
|
EMS |
* |
|||
|
ESS |
* |
|||
|
FAC |
* |
|||
|
FAI |
* |
|||
|
FIM |
* |
|||
|
FM motor |
* |
|||
|
FMA |
* |
|||
|
HR |
* |
|||
|
LLFDI |
* |
|||
|
MAS |
* |
|||
|
MEFAP |
* |
|||
|
MI |
* |
|||
|
MMAS |
* |
|||
|
MMSE |
* |
|||
|
MoAS |
* |
|||
|
MRC |
* |
|||
|
MRS |
* |
|||
|
NIHSS |
* |
|||
|
PROM |
* |
|||
|
RMAS |
* |
|||
|
RMI |
* |
|||
|
RPE |
* |
|||
|
RS |
* |
|||
|
SAS |
* |
|||
|
SF-36 |
* |
|||
|
SPPB |
* |
|||
|
SSS |
* |
|||
|
ST |
* |
|||
|
TBS |
* |
|||
|
TCT |
* |
|||
|
TGS |
* |
|||
|
TMS |
* |
|||
|
TUG |
* |
|||
|
Instrumental measures |
||||
|
JK |
* |
|||
|
STGP |
|
|
|
* |
|
For abbreviations, see Table II. |
||||
|
Table VI. Scales classified according to phase of disease used in the studies |
||||
|
Scales |
Phase of disease |
|||
|
Acute |
Chronic |
|||
|
Severe impairment |
Moderate impairment |
Severe impairment |
Moderate impairment |
|
|
2MinWT |
* |
* |
||
|
3MinWT |
* |
* |
||
|
5MWT |
* |
* |
||
|
6MinWT |
* |
* |
* |
* |
|
8MWT |
* |
* |
||
|
10MWT |
* |
* |
* |
* |
|
AS |
* |
* |
* |
* |
|
BBS |
* |
* |
* |
* |
|
BI |
* |
* |
* |
* |
|
BMI |
* |
* |
* |
* |
|
CES-D |
* |
* |
||
|
CNS |
* |
|||
|
EMS |
* |
|||
|
ESS |
* |
|||
|
FAC |
* |
* |
* |
* |
|
FAI |
* |
* |
||
|
FIM |
* |
* |
* |
* |
|
FM motor |
* |
* |
||
|
FMA |
||||
|
HR |
* |
* |
* |
* |
|
LLFDI |
* |
|||
|
MAS |
* |
* |
* |
|
|
MEFAP |
* |
|||
|
MI |
* |
* |
* |
* |
|
MMAS |
* |
* |
* |
* |
|
MMSE |
* |
* |
* |
|
|
MoAS |
* |
|||
|
MRC |
* |
* |
* |
* |
|
MRS |
* |
* |
||
|
NIHSS |
* |
* |
||
|
PROM |
* |
* |
||
|
RMAS |
* |
* |
* |
* |
|
RMI |
* |
* |
* |
* |
|
RPE |
* |
* |
* |
* |
|
RS |
* |
|||
|
SAS |
* |
* |
||
|
SF-36 |
* |
* |
||
|
SPPB |
* |
|||
|
SSS |
* |
* |
* |
* |
|
ST |
* |
|||
|
TBS |
* |
* |
* |
|
|
TCT |
* |
* |
||
|
TGS |
* |
* |
||
|
TMS |
* |
|||
|
TUG |
* |
* |
* |
|
|
Severe impairment – Functional Ambulation Category ≤ 2: the patient is not able to ambulate independently. Moderate impairment – Functional Ambulation Category ≥ 3: the patient is able to ambulate with verbal supervision, without physical contact. For abbreviations, see Table II. |
||||

Discussion
Our results show that FAC, 10MWT, MI, 6MinWT, RMI and BBS were the most used commonly outcome measures in ERAGTT. As regards ICF classification, they mainly belong to the activity domain (FAC, 10MWT, 6MinWT, RMI, and BBS) and only one to body function and structure (MI). No scale belonged to participation category (Fig. 1).
Fig. 1. International Classification of Functioning, Disability and Health (ICF) categorization of scales used in studies on the effects of rehabilitation treatments using electromechanical and robotic devices. “()”: ICF classification reference for each scale. For abbreviations of the scales, see Table II.
ICF classification
Body Function and Structures. The function level is an essential part of the assessment process. However, this level alone cannot provide information on whether the improvements are related to recovery of function or to compensation (12). The scales included in this classification often provide specific information regarding the quantity of movement performed by a subject, but not about the quality of movement needed to distinguish between the 2 different recovery processes (12). From a clinical point of view this represents a substantial weakness. Previous studies have not distinguished the 2 different processes in the selection of scales. Thus, the impairment scales should be accompanied with data about the quality of movement, as, for instance, provided by a dynamic electromyography (EMG) evaluation and gait analysis.
The main finding of this review is that the MI is the most widely used and reliable scale to evaluate body function and structure. Thus, post-stroke strength training represents an important part of a rehabilitation programme. The validity of the MI in the evaluation of lower limb muscle strength is also confirmed by instrumental strength evaluations, such as the dynamometer (79). However, the MI does not provide information regarding quality of motor performance and other associated phenomena (35), which could be important to evaluate specific ERAGTT effects. It is also noteworthy that the MI includes one sub-item (ankle dorsiflexion) that has been considered as a potential predictive factor of lower limb motor recovery (81).
Activity. The activity level is an essential part of the assessment process as well. However, the activity level alone cannot provide information on whether the improvements are related to the recovery of function or to compensation (12) because the term “limitation in activity” refers to one’s difficulty in completing a given task. Thus, the activity scales should be accompanied by quality of movement assessment, as previously discussed (12).
Furthermore, the activity recovery may not be necessarily correlated with improvements in ADLs, because an individual may improve in the activity domain with a scarce impact in their level of ADL independence in their social environment. In this context, the assessment of activity should be associated with participation scales, a crucial issue that should be considered in future studies (7).
The most commonly used scales to evaluate at the activity level in ERAGTT were the FAC, 10MWT, 6MinWT, RMI, and BBS.
The 10MWT is widely used to evaluate speed of walking (22). Velocity, in fact, is a component of walking that allows an individual to move within the home environment and the community (e.g. cross a street). Many individuals post-stroke are sedentary, which, when combined with normal ageing, predisposes them to increased functional deficits and declined activity tolerance (82).
Many studies used the 6MinWT to evaluate endurance of walking. Patients after stroke have shown a reduction in both strength and cardiorespiratory fitness (83). Thus, improving endurance of gait is one of the most important aims that should always be considered during ERAGTT. Correlations between improved walking endurance and decreased disability post-stroke are reported in several trials (4).
With regards to the assessment of mobility, the most widely used scale was the RMI. Mobility is one of the most important objectives in rehabilitation because its impairment has deleterious effects on ADLs and quality of life. A recent study showed that RMI can be used to predict the length of institutional stay for people with stroke within 5 days after stroke onset (84).
Finally, the BBS was the scale mainly used to evaluate balance, which is a very important skill in order to prevent falls and improve gait performance.
Participation. The participation domain, which represents one of the most challenging research issues in neurorehabilitation, has been partially neglected when selecting ERAGTT scales. Up to now, few studies have analysed the impact of the ERAGTT on improving individuals’ involvement in real-life situations, defined as participation (12).
During the rehabilitation period, robotic devices can be used to improve body functions/activities and to provide a quantitative assessment. Furthermore, the therapist should use these functional improvements to promote generalization processes in order to increase independence in ADLs. Future studies should consider this aspect as the ultimate goal of stroke rehabilitation, to discharge patients as functional community-dwelling adults.
It is noteworthy that this review process highlighted other important issues that require further discussion. In particular, (i) the time needed to perform the assessment, (ii) the psychometric properties of the scales, (iii) the phase of disease in which they were administered; and, finally, (iv) a proposal of battery of tests for future studies.
Time of scale administration
Our findings showed that the most commonly used scales are simple and do not require more than 20 min to administer (Table IV). The time required to administer a scale is an important feature. Indeed, many scales often require a long administration time, rendering them inappropriate in some contexts, such as in busy outpatient clinics (85).
Psychometric properties
The psychometric properties, such as reliability, validity, responsiveness, sensibility and MCID (10), represent important factors when selecting the most appropriate outcome measures (Table IV). They are no fixed scale properties, but they depend on the type of disease, on the phase of illness and on the population studied (10).
Almost all scales use in ERAGTT, except for the MI, are reliable. Reliability is a very important property for patient-based outcome measures in clinical trials. It is essential to establish that any change observed could be due to the intervention itself and is not related to any other problem in the measuring process. However, it does not yield any information about scale validity (10), such as, for instance, construction validity that refers to whether a scale measures or correlates with another measure to provide a basis for comparison (16). It is important to note that all of the most commonly used outcome measures have good construct validity.
As for responsiveness, the FAC, BBS, RMI, and 10MWT presented a large responsiveness value, while it was not reported for 6MinWT and MI. Responsiveness is the sensitivity of a scale to change within patients over time. One of the main limitations on the responsiveness of an instrument regards to the ceiling and floor effects. These data are not reported for FAC, 6MinWT and MI (Table IV).
MCID, which is defined as the smallest difference score in the domain of interest, which the individual feels as beneficial, was found only for the 6MinWT and 10MWT.
To conclude, the results showed that several properties of the scales are not currently available. Further studies are needed to obtain the missing properties during different phases of disease.
The most-used outcome measures according to the severity and phase of disease
A further analysis of these studies was performed to evaluate the severity and phase of disease where the scales were used. Our intention is to provide an overall perspective of the scales used in ERAGTT, classified according to the ambulation independence by the FAC scale as a benchmark, due to its large diffusion. We believe that such classification could help clinicians to choose the most appropriate scale during clinical practice.
Based on the scale’s clinical significance, we considered patients who received a score ≤ 2 (the individual is not able to ambulate independently) as severely impaired, whereas those who received a FAC score ≥ 3 (the individual is able to ambulate with verbal supervision, without physical contact) as moderately impaired (54). The results showed that the most widely used outcome measures were administered in every phase of disease. Therefore, walking independence, velocity, endurance, balance, mobility and muscle strength, are important components of walking that should be considered from early to late phases of disease to maximize gait recovery (Table VI).
The proposal of battery of tests according to ICF domains and 3-Dimensional Model
The development of a standardized protocol would permit comparison between different studies, allowing the best rehabilitation approaches to be identified. For example, a Cochrane review showed interesting results emerging from the analysis of effects of robot-assisted therapy to improve gait function. However, the authors could not perform a comparison because of the difference in outcome measures used (4).
Sivan and collaborators (7) performed a similar review, identifying the scales used during robot-assisted upper limb rehabilitation trials in stroke patients. They did not arrive to a shared consensus about the clinical outcome examinations; however, they concluded that the ICF is an appropriate framework to use when choosing an outcome measure. Our results are confirmed by existing literature in neurological rehabilitation of patients with stroke (86).
The choice of the most appropriate clinical scales could be improved, taking into account the following items (7): (i) ICF model to identify the main domains of outcome measures; (ii) analysis of essential psychometric properties (reliability, validity, responsiveness and sensibility), along with MCID and levels of measurement; (iii) identification of the aim of the measurement (ADL, impairment); (iv) distinction of the different clinical histories of stroke and severity and, subsequently, choice of the optimal scale; (v) nature of the study (effectiveness or efficacy); and (vi) modality of test administration (e.g. interview, questionnaire, phone, or self-report). Future studies should also consider the recovery processes mentioned previously (12).
With this in mind, a specific protocol based on the ICF domain and on a 3-Dimensional Model could be proposed in order to evaluate ERAGTT effects on walking in the clinical setting (10) (Table VII). It is important to note, that this proposal is the result of this extensive review of the literature and it is aimed at satisfying discriminative, evaluative and predictive purposes (Table VII). According to this proposal, the examiner may be guided when choosing the most appropriate scales regarding both the type of measurement (discriminative, evaluative or predictive) and the ICF domain. For instance, the MI, MAS, FAC, 10MWT and 6MinWT could be chosen for discriminative measurements of patients features with reference to body function and structure, and activity domain, respectively. In contrast, if an assessor desires to predict a specific ability that the patient may be able to perform after treatment, the RMI and PASS scales may be used (Table VII).
It is important to note that the BBS could be replaced by the Postural Assessment Stroke Scale (PASS) (87). Furthermore, the MAS and Stroke Impact Scale (SIS) (88) could be considered for inclusion, to evaluate body function and structure, and participation respectively.
|
Table VII. Proposed battery of tests according to the International Classification of Functioning, Disability and Health (ICF) domains and 3-Dimensional Model (10). The tests are listed according to the measurement aim, as discriminative, evaluative or predictive. The discriminative scales can be used to divide the patients into homogeneous groups for experimental design. The evaluative scales can be used to evaluate the effects of treatment between the beginning and end of therapy. The predictive scales can be used to predict a specific ability the patient will be able to perform |
|||||
|
Type of measurement |
Level of assessment (ICF) and domains of assessment |
||||
|
Body function and structures |
Activity |
Participation, health-related and quality of life |
Contextual factors |
||
|
Environmental factors |
Personal factors |
||||
|
Discriminative |
MI, MAS |
FAC, 10MWT, 6MinWT, |
|
|
|
|
Evaluative |
MI, MAS |
FAC, 10MWT, 6MinWT, RMI PASS |
SIS |
Patientand carer impression |
|
|
Predictive |
MI |
FAC, 10MWT, 6MinWT, RMI, PASS |
SIS |
|
|
|
SIS: Stroke Impact Scale; PASS: Postural Assessment Stroke Scale. For other abbreviations, see Table II. |
|||||
Finally, personal and environmental factors could be included in a specific section (“contextual factors” in Table VII) in order to evaluate the patients’ and caregivers’ impressions of ERAGTT. Both patient and caregiver perception have an important influence on any intervention in rehabilitation, and especially when robot-assisted training is performed. As a whole, the time required to administer this proposed protocol is approximately 56 min (i.e. PASS 10 min; MAS 1 min; SIS 9 min), hence a cost-effective and quick tool.
With respect to the importance of evaluating gait impairment, as well as gait improvements, from a qualitative point of view, instrumental analysis, such as EMG, should be associated with this clinical evaluation protocol. This is particularly relevant when a distinction between recovery of function and compensation needs to be clarified. However, a distinction between clinical and research settings should be also considered. Specific information or analysis methods may be predominantly suitable or relevant in a research setting instead of a clinical setting.
The main limitation of this review is that robotic orthotic devices were excluded. Secondly, this review attempts to be as comprehensive as possible, but it is likely that some articles were missed. Thirdly, it is possible that other outcome measures, more accurate than those found in the ERAGTT, could be suitable.
In conclusion, we propose a strategy to support researchers and clinicians in the selection of outcome measures in order to evaluate the effects of robotic devices for gait rehabilitation. We believe that a shared evaluation protocol based on ICF domains may provide information to detect changes in the basic components of walking and patient’s involvement in real-life situations.
Finally, the selection of common outcome measures could implement research in this important field of rehabilitation by promoting clinical trials and multicentre studies. Future investigations should take into account these considerations, in order to achieve homogeneity among clinical studies and thus allow their results to be compared.
References

