Anke I. R. Kottink, PhD1, Martin J. B. Tenniglo, PT1,2, Wiebe H. K. de Vries, MSc1, Hermie J. Hermens, PhD1 and Jaap H. Buurke, PhD1,2
From the 1Roessingh Research and Development and 2Roessingh Rehabilitation Centre, Enschede, The Netherlands
Anke I. R. Kottink, PhD1, Martin J. B. Tenniglo, PT1,2, Wiebe H. K. de Vries, MSc1, Hermie J. Hermens, PhD1 and Jaap H. Buurke, PhD1,2
From the 1Roessingh Research and Development and 2Roessingh Rehabilitation Centre, Enschede, The Netherlands
OBJECTIVE: The aims of this study were: (i) to compare the neuroprosthetic effect of implantable peroneal nerve stimulation to the orthotic effect of a standard of care intervention (no device, shoe or ankle foot orthosis) on walking, as assessed by spatiotemporal parameters; and (ii) to examine whether there is evidence of an enhanced lower-limb flexion reflex with peroneal nerve stimulation and compare the kinematic effect of an implantable peroneal nerve stimulation device vs standard of care intervention on initial loading response of the paretic limb, as assessed by hip, knee and ankle kinematics.
DESIGN: Randomized controlled trial.
SUBJECTS: A total of 23 chronic stroke survivors with drop foot.
METHODS: The intervention group received an implantable 2-channel peroneal nerve stimulator for correction of drop foot. The control group continued using a conventional walking device. Spatiotemporal parameters and hip, knee and ankle kinematics were measured while subjects walked with the device on using a 3-dimensional video camera system during baseline and after a follow-up period of 26 weeks.
RESULTS: Peroneal nerve stimulation normalized stance and double support of the paretic limb and single support of the non-paretic limb, in comparison with using a conventional walking device. In addition, peroneal nerve stimulation is more effective to provide ankle dorsiflexion during swing and resulted in a normalized initial loading response.
CONCLUSION: Although peroneal nerve stimulation and ankle foot orthosis are both prescribed to correct a drop foot in the same patient population, spatiotemporal parameters, dorsiflexion during swing and loading response are influenced in a functionally different way.
Key words: stroke; gait; drop foot; peroneal nerve; electrical stimulation.
J Rehabil Med 2012; 00: 00–00
Correspondence address: Anke I. Kottink, Roessingh Research and Development, PO Box 310, NL-7500 AH, Enschede, The Netherlands. E-mail: a.kottink@rrd.nl
Submitted August 30, 2010; accepted September 19, 2011
INTRODUCTION
One of the primary goals in the rehabilitation of a hemiplegic subject is to regain the ability to walk and to develop a safe and efficient gait pattern (1). Hemiparesis due to stroke often results in pre-tibial muscle weakness. When the weakness is mild, the paretic foot will slap during the loading response. When the dorsiflexion weakness is more severe, foot drop and toe drag will be observed during the swing phase of gait, causing the need for a compensated gait pattern and an increased risk of falling. Several strategies are available to compensate for a drop foot, such as circumduction of the ipsilateral leg, increased ipsilateral hip flexion and hip hiking to allow the weak ankle to clear the floor during the swing phase of gait (2). Over time, these compensation strategies can cause secondary complications, for example shortening of the calf muscles, arthritic changes of the hip or knee, and further deterioration of balance leading to falls and reduced confidence (2).
The most traditional and most often applied device to correct a drop foot is the ankle-foot orthoses (AFO) (3). An alternative treatment is peroneal nerve stimulation (PNS), firstly introduced by Liberson et al. (4). Both devices support the ankle joint during a different phase of the gait cycle. An AFO provides mediolateral stability at the ankle joint during stance, facilitates toe clearance during swing and promotes heel strike (5). PNS stimulates the dorsiflexors that lift the foot in (pre-)swing, allowing the foot to clear the ground, and results in a safe initial loading response during stance. There is also evidence in spinal cord injured (SCI) subjects that PNS may trigger the lower-limb flexion reflex and thus facilitate the flexion pattern needed for foot clearance during swing (6).
Studies on the effect of PNS on the hemiplegic gait pattern and the compensation strategies used by these patients are scarce. Ring et al. (7) examined the effect of PNS on gait stability and symmetry in comparison with an AFO. Users of the neuroprosthesis showed better balance control and symmetry during walking. However, some of the limitations of their study were the short period of follow-up, being 8 weeks, the lack of a baseline measurement with the AFO and no addition of a control group. Recently, a case study showed that both a surface-based and an implanted FES system resulted in a near-normal gait pattern in chronic stroke in comparison with an AFO, resulting in adequate foot elevation, increased hip and knee angles, increased ankle push-off power and an almost symmetrical and less variable gait pattern (8). The authors stated that further research including these outcome measures is needed to study the superiority of PNS over an AFO with respect to walking ability. This would allow clinicians to make better recommendations regarding these technical aids.
The first aim of the present randomized controlled trial (RCT) therefore was to explore the orthotic effect of an implantable 2-channel PNS in comparison to a conventional walking device. Since both walking devices support the ankle joint during a different phase of the gait cycle, PNS is expected to result in an improved swing phase, resulting in a better dynamic balance. The second aim of this study was to examine whether the use of PNS improved the lower-limb flexion reflex and resulted in a normalized initial loading response of the paretic limb.
METHODS
Study design
The present study reported one of the outcome parameters that were measured in a RCT. In this RCT all subjects were assessed 5 times. The baseline measurement took place approximately 1 week before the randomization procedure and the follow-up measurements were performed 4, 8, 12 and 26 weeks after implanting the 2-channel peroneal nerve stimulator in the intervention group. Subjects assigned to the control group were measured in the same weeks as subjects assigned to the intervention group. All assessments were performed by the same experienced examiners (AK, MT). Three weeks after implantation subjects received the transmitter, and instructions were given on the proper use of the peroneal nerve stimulator. The use of the stimulator was gradually increased over 2 weeks to prevent severe muscle pain and fatigue. After this period patients were allowed to use the system all day. Instructing the subjects in the intervention group on the proper use of the peroneal nerve stimulator and assessment of stimulation levels of the 2 output channels took place on the same day as the outcome assessments. If problems were experienced by the patients they were instructed to report them immediately, so that they could be resolved as soon as possible. In order to assess the orthotic effect of an implantable 2-channel peroneal nerve stimulator vs a conventional walking aid on the gait pattern of chronic hemiparetic subjects, measurements were performed at baseline and at week 26. Blinding of both the outcome testers and participants was not possible due to the surgical procedure.
Subjects
Most subjects were recruited in response to an article in a local Dutch newspaper describing the first results on the implantable stimulator in stroke survivors. Some subjects were recruited through consultant and general practitioner referrals and in some cases on the advice of the physiotherapist treating the subject. Both recruitment strategies resulted in a selected sample of well-motivated stroke survivors. Because of the invasive nature of the treatment, selection of the most appropriate subjects is very important. Therefore subjects that were most likely to experience treatment success were selected. All included subjects were outdoor walkers and had a drop foot as a result of a first hemiplegia of at least 6 months’ duration. For further details about inclusion and exclusion criteria, see Kottink et al. (9). Subjects who fulfilled the selection criteria were admitted to the trial. One week after the baseline assessment they were randomly allocated to either the intervention or control group. Random allocation was performed in blocks of two subjects, to ensure a close balance of the numbers in each group. The randomization procedure was performed by an independent individual. Each time two suitable subjects were included their names were given to the person who was responsible for randomization. After the baseline measurement, this person informed the examiner which subject was allocated to the intervention and which subject was allocated to the control group.
The study protocol was approved by the local medical ethics committee and the subjects gave their informed consent before participation.
Stimulation system
The implantable 2-channel peroneal nerve stimulator (Finetech Medical Ltd, Welwyn Garden City, UK) consists of an external transmitter with a built-in antenna, a foot switch, and an implantable part consisting of the stimulator, the two leads and the bipolar intra-neural electrodes (10, 11).
The transmitter weighs approximately 0.1 kg and is attached with a strap on the lateral side of the lower leg, over the site of the implant, just below the knee. A footswitch placed under the heel of the subject’s foot inside the shoe determines the on-and-off switching of the stimulation. The transmitter battery is charged overnight.
The implantable part is a passive device, receiving information carried by the radio frequency signals and converting that information into the stimulation pulses of the desired amplitude and frequency. One electrode is placed below the epineurium of the superficial peroneal nerve (eversion) and one below the epineurium of the deep peroneal nerve (dorsiflexion). For a more detailed description of the implantable stimulator see Kottink et al. (9).
Assessment of spatiotemporal parameters and kinematics
Both the baseline and follow-up assessment were performed in the gait laboratory of Roessingh Research and Development. The experiment started with collecting the anthropometric data of the subjects. The gait pattern was recorded by using a 3-dimensional video camera system, consisting of 6 stationary cameras (Vicon®, version 370, Oxford, UK) (12). The model used in the present study was based on the Davis-Kadaba model (13–17). In total 17 markers were placed on both legs and pelvis (first and fifth head of the metatarsal, lateral malleolus of the ankle, heel, lateral epicondyle of the femur, anterior superior iliac spine, sacrum and 4 reflective markers on the lateral aspect of the upper and lower legs). During an initial calibration measurement extra markers were placed on the medial epicondyle of the femur and the medial malleolus of the ankle on both legs. All ankle angles were adjusted for the angle in sagittal plane between foot orientation and the horizontal plane of the floor as obtained in this measurement by adding this angle. This procedure corrected for differences in ankle angle due to differences in shoes worn, or walking aids used over the course of the experiment. All markers were labelled by means of the Vicon Bodybuilder programme version 3.55 and the gait data were analysed with the Vicon model output viewer. First initial contact (IC) and toe off (TO) were detected using a threshold algorithm on the vertical height of the markers on the foot, which indicated foot contact consistently when the markers were within a constant distance from the floor. Concurrently, the gait data were normalized to a 0–100% gait cycle and then averaged.
The subjects walked at their natural speed. At baseline, both the intervention and control group used their conventional walking device. At week 26, the intervention group was measured during walking with PNS, while the control group was measured during walking with their conventional walking device again. When possible, subjects walked without a walking stick. If this was not the case, subjects had to use the same assistive device at week 26 as during baseline and this was recorded. The condition during baseline was the standard for the follow-up measurement. To exclude the influence of acceleration and deceleration at the beginning and end of the walkway, subjects started walking far before the field of and stopped far behind the view of the cameras. Four trials were analysed and averaged for each subject to obtain all parameters.
To explore the effect of PNS and an AFO on walking, different spatiotemporal parameters of both the paretic and non-paretic limb, such as stride time, stride length, stride width, step length, duration of stance phase, first double support phase (IC first foot till TO second foot) and first single support phase (TO second foot till IC second foot) were derived. With the intention of keeping walking speed consistent, walking speed was measured at baseline and at week 26.
To examine if PNS resulted in an increased lower-limb flexion reflex during swing and if PNS resulted in a normalized initial loading response also hip-, knee and ankle kinematics of the paretic leg were measured by the Vicon® system. Ranges of motion (ROM) of these joints were determined by comparing calculated angles at predefined points in the gait phase of interest. These phases, defined in Table I, were based on both IC and TO events of the paretic and non-paretic leg. To show the specific joint angles that are taken in the analysis, Fig. 1 shows a typical example of the hip, knee and ankle kinematics in the sagittal plane of a subject with right hemiplegia.
| Table I. Definitions of gait phases | |
| Phase | Description |
| Pre swing | Opposite IC–TO |
| Swing | TO–IC |
| Initial swing | First 30% of the swing phase |
| Mid-swing | 30–70% of the swing phase |
| Terminal swing | 70–100% of the swing phase |
| IC: initial contact; TO: toe off. | |
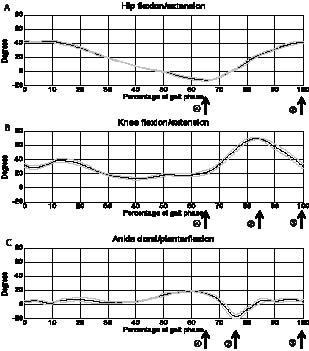
Fig. 1. A typical example of the kinematics in the sagittal plane of the non-paretic limb of a subject with right hemiplegia: hip flexion/extension, knee flexion/extension and ankle dorsi/plantarflexion. The bands represent the mean (standard deviation 1). The arrows reflect the joint angles taken in the analysis: (A) arrow 1 indicates minimum hip angle (stance); arrow 2 indicates maximum hip angle (swing); (B) arrow 1 indicates minimum knee angle (stance); arrow 2 indicates maximum knee angle (initial/mid swing); arrow 3 indicates knee angle (initial contact (IC)); (C) arrow 1 indicates maximum ankle angle (stance); arrow 2 indicates minimum ankle angle (swing); arrow 3 indicates ankle angle (IC).
Statistical analysis
Both within-group and between-group p-values for the spatiotemporal parameters and kinematics were calculated with SPSS version 18 for Windows (SPSS, Chicago, USA). Because of the small sample size for each group, the Wilcoxon signed-rank test was used to compare the spatiotemporal and kinematic data in both groups between baseline and week 26 (within-group analysis). An analysis of covariance (ANCOVA) was used to test if differences in all spatiotemporal parameters and kinematics were present between the intervention and control group at week 26 (between-group analysis). To correct for possible differences at baseline between the intervention and control group, the baseline scores were taken as covariate. Group was taken as the only fixed factor in the analysis. Normality plots of the residuals were made to examine whether the data were distributed according to a normal distribution. The significance level α was set at 0.05 for all tests.
RESULTS
Subjects
Fig. 2 shows the flow of participants throughout the RCT. In total, 29 subjects with drop foot due to stroke participated in the RCT, of which 14 subjects were allocated to the intervention group and 15 subjects were allocated to the control group. Both the orthotic and therapeutic effect of the implantable peroneal nerve stimulator on walking speed and some other parameters were previously described (9, 18). The current study, which aims to make a comparison between walking with PNS and a conventional walking aid, is based on a subset of the included subjects. Since 4 subjects of the intervention group did not use a conventional walking aid to correct their drop foot, they were excluded from analysis in the present study. In the past these subjects were all advised by their therapist/doctor to use a conventional walking aid, but at the time of inclusion they no longer used it. Two subjects in the control group were excluded since their gait pattern was not recorded at baseline. Table II shows the characteristics of the included participants of the present study. Subject characteristics were not significantly different between both groups, with the exception of mean time after stroke, which was longer for the intervention group.
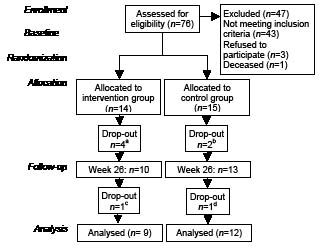
Fig. 2. Flow of patients through the study. Reasons for lost to follow-up: ano conventional walking device; bno gait pattern recorded; cdefective implant; dpsychological issues not related to the study.
| Table II. Subject characteristics | ||
| Characteristics | Intervention group | Control group |
| Subjects (drop outs), n | 10 (1) | 13 (1) |
| Men/women, n | 7/3 | 8/5 |
| Age, years, mean (SD) | 55.6 (13.16) | 53.31 (10.55) |
| Time after stroke, years, mean (SD) | 9 (10.04) | 6.15 (4.81) |
| Affected side, left/right, n | 6/4 | 8/5 |
| SD: standard deviation. | ||
In the intervention group (n = 10) 3 subjects wore orthopaedic shoes at baseline, 4 subjects used a polypropylene, non-articulated AFO with 2 crossed posterior steels and an open heel (Ottobock, Otto Bock Benelux bv, Son en Breugel, The Netherlands), 2 subjects used a custom made polypropylene, non-articulated AFO with a large posterior steel (Camp, Basko Healthcare, Zaandam, The Netherlands) and 1 subject used a polypropylene, non-articulated AFO with a small posterior steel (Dynafo, Ortho-Medico, Herzele, Belgium). In the control group (n = 13), all subjects wore an AFO at baseline and at week 26. Three subjects used a polypropylene, non-articulated AFO with two crossed posterior steels and an open heel, 4 subjects used a custom-made polypropylene, non-articulated AFO with a large posterior steel, 4 subjects used a polypropylene, non-articulated AFO with a small posterior steel, and two subject used a non-custom made polypropylene, non-articulated AFO with a large posterior steel. Two subjects dropped out of the study, 1 woman in the intervention and 1 man in the control group. The implant of the drop-out in the intervention group failed after functioning properly for approximately 10 weeks. An investigation of the explanted system showed that the failure was caused by a technical defect in the epineural electrode responsible for the dorsiflexion movement. One subject in the control group dropped out in week 11, because of psychological issues not related to the study. The remaining 9 subjects in the intervention group did not report any technical failure of the stimulation system and continued to use the stimulator during the entire follow-up period.
Spatiotemporal parameters
Table III shows the spatiotemporal parameters of the paretic and non-paretic limb for the intervention and control group during walking with either PNS or conventional walking aid.
| Table III. Spatiotemporal parameters | |||||||
| Parameters | Intervention group (n = 9) | Control group (n = 12) | Within-group p | Between-group p | |||
| Baselinea Mean (SD) | Week 26b Mean (SD) | Baselinea Mean (SD) | Week 26a Mean (SD) | Intervention group | Control group | ||
| Walking speed, m/s | 0.92 (0.1) | 0.95 (0.13) | 0.75 (0.21) | 0.83 (0.24) | 0.14 | 0.03 | 0.17 |
| Stride time, s | 1.3 (0.1) | 1.2 (0.1) | 1.4 (0.3) | 1.4 (0.3) | 0.02 | 0.29 | 0.35 |
| Stride length, cm | 114 (9.9) | 114 (15.4) | 98 (16.1) | 104 (20.9) | 0.95 | 0.1 | 0.21 |
| Stride width, cm | 18 (6.6) | 14 (6.3) | 17 (5.2) | 15 (6.1) | 0.14 | 0.02 | 0.44 |
| Step length, cm Paretic side | 64 (11.6) | 63 (14.3) | 55 (9.4) | 57 (16.1) | 0.59 | 0.88 | 0.31 |
| Non-paretic side | 49 (8) | 51 (7.9) | 43 (8.9) | 47 (10.5) | 0.68 | 0.09 | 0.78 |
| Stance phase, % Paretic side | 63 (3.8) | 60 (5.4) | 66 (5.4) | 66 (4.4) | 0.37 | 1.0 | 0.03 |
| Non-paretic side | 74 (3.7) | 71 (3.1) | 76 (5.5) | 74 (5.9) | 0.05 | 0.07 | 0.18 |
| First double support phase, % Paretic side | 16 (2.9) | 11 (3.3) | 17 (3.5) | 17 (5.7) | 0.05 | 1.0 | 0.03 |
| Non-paretic side | 22 (2.8) | 19 (4.4) | 23 (5.1) | 22 (4.4) | 0.11 | 0.22 | 0.1 |
| First single support phase, % Paretic side | 25 (3.6) | 29 (2.7) | 25 (5.4) | 26 (5.9) | 0.05 | 0.21 | 0.13 |
| Non-paretic side | 36 (2.9) | 41 (5.1) | 35 (4.4) | 35 (4.7) | 0.07 | 0.88 | 0.02 |
| aWalking with conventional walking aid. bWalking with PNS. SD: standard deviation. | |||||||
Within-group differences. Although the intention was to keep walking speed constant during both evaluations, the control group walked significantly faster at week 26. Also, stride width decreased significantly within the control group over time.
For the paretic limb, although a trend towards significance was found for an improved first double and single support phase in the intervention group, none of the spatiotemporal parameters changed significantly within both groups over time.
For the non-paretic limb, although a trend towards significance was found for an improved stance phase in both groups and an improved first single support phase in the intervention group, none of the spatiotemporal parameters changed significantly within both groups over time.
Between-group differences. For the paretic limb, stance and first double support changed significantly between both groups over time. The intervention group showed a reduced stance and first double support phase at follow-up, while the control group did not change. None of the other spatiotemporal parameters changed significantly between both groups.
For the non-paretic limb, first single support phase changed significantly between both groups over time. In the intervention group a longer first single support was found, while the control group did not change. None of the other spatiotemporal parameters changed significantly between both groups.
Kinematics
The joint angles in the sagittal plane of the paretic limb for the intervention and control group are shown in Table IV.
| Table IV. Joint angles in sagittal plane of paretic limb | |||||||
| Variables | Intervention group (n = 9) | Control group (n = 12) | Within-group p | Between-group p | |||
| Baselinea Mean (SD) | Week 26b Mean (SD) | Baselinea Mean (SD) | Week 26a Mean (SD) | Intervention group | Control group | ||
| Hip flexion-extension ROM, º | 32.34 (7.90) | 32.81 (9.59) | 35.89 (9.24) | 38.25 (9.41) | 0.86 | 0.23 | 0.38 |
| Minimum hip angle during stance, º | –7.42 (6.17) | –7.38 (6.02) | –9.94 (7.43) | –11.96 (9.59) | 0.68 | 0.18 | 0.36 |
| Maximum hip angle during swing, º | 24.92 (6.73) | 25.43 (7.17) | 25.94 (7.83) | 26.29 (10.45) | 0.59 | 1.0 | 0.99 |
| Knee flexion-extension ROM, º | 30.95 (11.15) | 28.35 (14.93) | 38.18 (13.92) | 42.93 (16.95) | 0.55 | 0.06 | 0.09 |
| Minimum knee angle during stance, º | 2.84 (8.55) | 4.32 (9.44) | –1 (7.07) | –4.46 (6.76) | 0.12 | 0.07 | 0.03 |
| Maximum knee angle during initial/mid swing, º | 33.79 (8.59) | 32.68 (11.49) | 37.18 (12.39) | 38.47 (13.32) | 0.95 | 0.91 | 0.46 |
| Ankle dorsi-plantarflexion ROM, º | 18.91 (8.44) | 13.36 (5.08) | 14.10 (7.07) | 15.54 (5.40) | 0.07 | 0.33 | 0.04 |
| Maximum ankle angle during stance, º | 14.58 (7.11) | 14.05 (6.03) | 8.63 (8.15) | 10.31 (6.87) | 0.77 | 0.27 | 0.94 |
| Minimum ankle angle during swing, º | –4.32 (6.81) | 0.69 (5.82) | –5.48 (4.34) | –5.24 (5.21) | 0.05 | 0.67 | 0.03 |
| Knee angle at IC, º | 13.92 (6.84) | 16.94 (5.93) | 12.41 (5.81) | 10.18 (7.98) | 0.14 | 0.39 | 0.04 |
| Ankle angle at IC, º | –1.14 (5.50) | 2.89 (6.46) | –4.38 (5.29) | –4.56 (7.47) | 0.26 | 0.76 | 0.08 |
| aWalking with conventional walking aid. bWalking with PNS. SD: standard deviation; ROM: range of motion; IC: initial contact. Positive values indicate hip/knee flexion or ankle dorsiflexion; negative values indicate hip/knee extension or ankle plantarflexion. | |||||||
Within-group differences. Although a trend towards significance was found in the intervention group for an improved ankle ROM and minimum ankle angle during swing, none of the joint angular parameters changed significantly within the intervention group over time. For the control group a trend towards significance was found for a worsened knee extension during stance and knee ROM; however, none of joint angular parameters changed significantly within the control group over time.
Between-group differences. Minimum knee angle in stance changed significantly between both groups over time. The intervention group showed more knee flexion, while the control group showed more knee extension during stance at follow-up. Also, a significant change in minimum ankle angle during swing was found. The intervention group changed from 4.32º ankle plantarflexion to 0.69º ankle dorsiflexion during swing at follow-up, while ankle plantarflexion of the control group did not change (5.48º to 5.24º). Consequently, ankle ROM changed significantly over time between both groups. The intervention group showed a significant reduction of 5.5º in ankle plantarflexion at follow-up, while the control group showed a small increase in ankle plantarflexion of 1.4º. With regard to knee flexion at IC, a significant increase of 3.02º was found in the intervention group over time when compared with the control group, who showed 2.23º less knee flexion at follow-up. Also, a trend towards significance was found for ankle plantarflexion at IC between both groups over time. The intervention group showed 2.89º ankle dorsiflexion at IC at follow-up, while the plantarflexion angle of the control group remained constant at IC (4.38º to 4.56º). None of the other joint angular parameters changed significantly between both groups.
DISCUSSION
The present study made a comparison between walking with PNS and walking with a conventional walking device to correct a drop foot.
In the present study PNS, which supports the swing phase of gait, normalized the total stance (60%) and single stance phase due to the earlier TO of the paretic limb, caused by the start of the PNS in pre-swing. On the non-paretic side a significantly longer single support was found as a result of PNS, caused by the longer swing phase of the paretic limb. PNS also improved double support of the paretic limb, indicating an improved dynamic balance. This effect is likely to be caused by an improved loading response while walking with PNS, resulting in a more stable position of the paretic limb during the first double support phase. These results suggest that, although PNS and AFO are prescribed to correct a drop foot in the same patient population, spatiotemporal parameters are influenced in a functionally different way.
Literature about the effect of a PNS on the gait pattern of stroke subjects is scarce; most studies focused on outcome measures such as walking speed (19). An uncontrolled study has examined the effect of surface-based PNS in comparison with an AFO on postural control in 15 patients with chronic stroke or traumatic brain injury (7). The results show a shorter stride time, a less asymmetrical gait pattern and a less variable and more consistent single support of the paretic limb after 8 weeks use of PNS. These results do not correspond with the current findings, probably caused by the more affected subjects included by Ring. Their subjects walked, for example, with a speed of 0.58 m/s with an AFO at baseline, measured with the 6-min walk test.
Hemiplegic subjects usually have less dorsiflexion during mid-swing and heel strike due to loss of motor control, spasticity of the gastrocnemius-soleus group and ankle contracture (20). In healthy subjects, the increase in pre-tibial muscle action during terminal swing assures that the ankle and foot are adequately pre-positioned for IC (21).
Regarding the kinematics of the paretic limb, a significantly reduced ankle plantarflexion during swing was found as a result of PNS. Therefore PNS seems very effective to provide ankle dorsiflexion during swing. Also, a trend towards significance was found for reduced ankle plantarflexion at IC during walking with PNS. This adequate pre-positioning is likely to prevent stroke patients from stumbling or falling. Although no results for stroke subjects are described in the literature, these findings were confirmed in studies performed by other patient populations (22–24). In incomplete SCI foot clearance was improved with PNS and not with an AFO (22). Ladouceur & Barbeau (23) reported that ankle plantarflexion at IC decreased by 5.6º as a result of PNS in incomplete SCI subjects. In patients with multiple sclerosis PNS significantly increased ankle dorsiflexion at IC compared with an AFO (25).
No evidence was found that PNS may trigger hip and knee flexion, which is not in accordance with earlier results described in literature where surface-based PNS was used (6) (8). A possible explanation could be that in the present study an implantable PNS was used, which results in less exteroceptive stimuli. Also, less current is needed to obtain an adequate dorsiflexion with an implant, whereby no flexion of other segments took place. One study also reported a lower-limb flexion reflex with an implant; however, this was a case-study, so no control group was included (8). Therefore these results may be coincidental.
Limitations
When interpreting hemiplegic spatiotemporal data, the speed dependence of spatiotemporal characteristics must be considered (26). Unless efforts were made to maintain walking speed constant over time, the control group walked significantly faster at follow-up. The increased walking speed could have influenced the spatiotemporal parameters of the control group in a positive way, making the real effect of PNS on the spatiotemporal parameters smaller.
A limitation of this study was the small study population. When looking at the results often a trend towards significance was found, probably caused by a low power.
Another limitation may be the generalization of the present results to the broader population with stroke. The included subjects were selected primarily on their suitability for implantable PNS, which means that a subpopulation of less affected subjects was included.
Also, the non-uniformity of the conventional walking devices used by the included subjects could be a confounding factor. However, this situation will be most consistent with clinical practice, in which stroke survivors also use different devices for correction of their drop foot.
Furthermore, participants and investigators were not blinded. Participant blinding was not possible and investigators blinding was not possible because the peroneal nerve stimulator and the conventional walking aid could not be hidden from view during the measurement. To minimize this bias, the involvement of the investigators (e.g. instructions, encouragement) was kept consistent during data collection and the data analysis was performed by a person who was not involved in the present study.
In conclusion, PNS normalized stance and double support of the paretic limb and single support of the non-paretic limb. Also, PNS is more effective to provide ankle dorsiflexion during swing and resulted in a normalized initial loading response in comparison with a conventional walking device, which is likely to reduce the risk of stumbling or falling in chronic stroke survivors with a drop foot. No evidence was found that PNS may trigger hip and knee flexion.
REFERENCES

