OBJECTIVE: Mortality, cause of death and risk indicators for death among patients with traumatic spinal cord injury were investigated over a 30-year period.
DESIGN: A cross-sectional study with retrospective data.
SUBJECTS: All patients (n = 1647) aged 16 years and over who had sustained traumatic spinal cord injury during the period 1976–2005, who were admitted to Käpylä Rehabilitation Centre, Helsinki, Finland, participated in the study.
METHODS: Demographic and clinical data were collected from the registers of Käpylä Rehabilitation Centre. Cause-specific mortality was assessed using Statistics Finland’s official cause-of-death register.
RESULTS: During the observation period (1976–2007) 419 patients died. The main causes of death were respiratory disease (28%), cardiovascular disease (21%), suicide (10%) and external causes (9.5%). The mean age at death was 55.5 years for men and 58.2 years for women. Ten-year survival was 97.9%. Mortality was significantly affected by age at onset of injury, neurological level and extent of lesion. Survival of traumatic spinal cord injury patients was approximately 50% that of the general population, and survival of the general population was 80% during the follow-up period.
CONCLUSION: These results support the need for improvements in long-term rehabilitative care and regular follow-up of patients with traumatic spinal cord injury. The importance of psychosocial follow-up services must be emphasized.
Key words: traumatic spinal cord injury mortality; cause of death; risk indicator; epidemiology.
J Rehabil Med 2011; 43: 481–485
Correspondence address: Eija Ahoniemi, Käpylä Rehabilitation Centre, Finnish Association of People with Mobility Disabilities, Nordenskiöldinkatu 18 B, FI-00251 Helsinki, Finland. E-mail:eija.ahoniemi@invalidiliitto.fi
Submitted August 30, 2010; accepted March 17, 2011
Introduction
The incidence of traumatic spinal cord injury (TSCI) in Finland is 13.8/1,000,000 persons per year (1). Approximately 60–70 new cases of spinal cord injury (SCI) emerge in Finland each year. Acute care of patients with trauma of the spinal column with or without neurological deficit takes place in regional university and central hospitals. Since the 1960s, the rehabilitation of patients with TSCI has been centralized to the Käpylä Rehabilitation Centre, Helsinki, which is the only national, specialized centre for SCIs in Finland. There has been no regular follow-up during the first 20 years in Finland. However, most TSCI patients have been re-rehabilitated yearly.
Despite earlier medical care and specialized rehabilitation, the life expectancy of persons with SCI is lower than of the general population (2–5). The most common causes of death are lung disease, cardiovascular disease, and complications of respiratory disease and urinary tract disease (2, 3, 6–8). Several studies have shown that important risk indicators for death include neurological level, extent of lesion, higher age at injury (2, 6, 7, 9), pre-injury cardiovascular disease, alcohol or substance abuse, and psychiatric diagnosis (4, 10, 11).
Previous studies on survival of TSCI in Finland are lacking. The aims of our study were: to examine survival in 1647 persons with TSCI admitted to Käpylä Rehabilitation Centre; to compare their survival with that of the general population; to evaluate causes of death; and to explore predictors of eventual early death in SCI.
Methods
Materials
During 1976–2005 a total of 1647 persons with TSCI were admitted to Käpylä Rehabilitation Centre. Of these patients, 51% had tetraplegia and 49% paraplegia. The mean age at the time of injury was 37.6 years for men and 37.8 years for women. The majority of injuries were the result of falls (41.2%) and traffic accidents (39.5%).
Data collection
Information was extracted from each patient’s medical records at Käpylä Rehabilitation Centre. Data included demographic characteristics of patients, cause of injuries, admission and discharge from the rehabilitation centre, and injury-related data, including associated injuries caused by the accident and neurological level of injury grouped into tetraplegia, i.e. cervical spinal cord lesions, or paraplegia, i.e. thoracic and lumbar-sacral lesions. The median length of follow-up was 12.5 years (interquartile range (IQR) 5.5–19.8 years). Dates of deaths were registered until 31 March 2007.
To determine cause of death, information was collected from the official cause of death register of Statistics Finland. The register is based on medical death certificates. The classification of cause of death was taken from International Statistical Classification of Diseases and Related Health Problems (ICD-9) for the period 1976–1995 and from ICD-10 for the period 1996–2005. There were many cases (n = 124) for which the underlying causes of death were specified by an initial trauma (classed as E801A–B, E8120, E8162, E880A, E881A, E883A, E889A, E929E, F–H–I, V484,V485, W01, –06, –10, –11, –12, –13, –16, –18, W24, Y31, Y850, Y859, Y86, Y870, –1, –2). The causes of death in these cases were determined by using the direct causes of death.
Neurological status was determined using the American Spinal Injury Association (ASIA/AIS) grading scale.
Statistical analysis
Standardized mortality ratios (SMRs), survival rates and life expectancy were calculated for the complete sample and according to age group, sex and severity of injury. A Cox proportional hazards regression model was used to explore risk indicators for mortality.
The study protocol was approved by the ethics committee of Käpylä Rehabilitation Centre in Helsinki.
Results
Study population
Table I presents the study population (1647 patients) divided into tetraplegia and paraplegia groups. A sex difference was present in both groups. Persons with tetraplegia were significantly older at injury than those with paraplegia. In addition, a higher proportion of functionally incomplete SCI was evident in persons with tetraplegia than in those with paraplegia.
| Table I. Study population divided into tetraplegia and paraplegia groups |
| | Tetraplegia n = 836 | Paraplegia n = 811 |
| Male, n (%) | 721 (86) | 641 (79) |
| Complete | 238 (33) | 316 (49) |
| Incomplete | 483 (67) | 325 (51) |
| Female, n (%) | 115 (14) | 170 (21) |
| Complete | 33 (29) | 72 (42) |
| Incomplete | 82 (71) | 98 (58) |
| Mean age (SD), years | | |
| Male | 40.3 (16.7) | 34.5 (13.9) |
| Complete | 34.1 (14.9) | 32.6 (12.7) |
| Incomplete | 43.5 (16.7) | 36.3 (14.7) |
| Female | 44.4 (16.3) | 33.2 (12.8) |
| Complete | 38.0 (14.7) | 31.5 (12.2) |
| Incomplete | 47.0 (16.3) | 34.6 (13.0) |
| SD: standard deviation. |
At the end of follow-up 419 (25.4%; 59 women and 360 men) of the 1647 persons had died. The mean age at death was 55.5 years for men and 58.2 years for women.
Causes of death
Table II shows the number and percentages for underlying causes of death. The predominant underlying causes of death were cardiovascular disease (20.7%), suicide (10.3%), external causes (9.5%), respiratory disease (8.6%), cancer (7.6%), digestive disease (7.6%) and urological disease (1.4%). The mean time from injury to death was approximately 10 years. Mortality generally declined during the whole study period, but mortality for suicide was approximately 10% throughout the study period. Suicide was more common among persons with paraplegia, both female and male, than among those with tetraplegia. Time from injury to suicide varied during the study, from 14.2 years in the first 10 years to 3.5 years in the last 10 years.
| Table II. Underlying causes of death |
| Cause of death | Tetraplegia (n = 256) | Paraplegia (n = 163) |
| Male n = 223 n (%) | Female n = 33 n (%) | Male n = 137 n (%) | Female n = 26 n (%) |
| Cardiovascular disease | 47 (21.0) | 6 (18.2) | 31 (23) | 3 (11.5) |
| Ischaemic heart disease | 30 (13.5) | 3 (9.1) | 20 (14.6) | 1 (3.9) |
| Other heart disease | 3 (1.35) | 1 (3.0) | 4 (2.9) | 0 (0) |
| Cerebrovascular disease | 14 (6.3) | 2 (6.1) | 7 (5.1) | 2 87.7) |
| Suicide | 13 (5.8) | 0 (0) | 23 (17) | 7 (27) |
| External cause | | | | |
| Poisoning | 15 (6.7) | 1 (3.0) | 11 (8.0) | 1 (3.8) |
| Violence | 5 (2.2) | 1 (3.0) | 6 (3.7) | 0 (0) |
| Respiratory disease | 21 (9.4) | 2 (6.1) | 11 (8.0) | 2 (7.7) |
| Pneumonia | 16 (7.7) | 1 (3.0) | 8 (5.8) | 1 (3.9) |
| Lung disease | 5 (2.2) | 1 (3.0) | 3 (1.8) | 1 (3.9) |
| Cancer | 18 (8.1) | 1 (3.0) | 10 (5.8) | 3 (11.5) |
| Digestive disease | 10 (4.5) | 7 (21.2) | 13 (9.5) | 2 (7.7) |
| Urinary tract infection | 3 (1.4) | 1 (3.0) | 2 (1.5) | 0 (0) |
| Miscellaneous SCIa | 14 (6.3) | 0 (0) | 0 (0) | 3 (11.5) |
| | 77 (34.5) | 14 (42.4) | 30 (21.9) | 3 (11.5) |
| aE801A–B, E8120, E8162, E880A, E881A, E883A, E889A, E929E, F–H–I, V484, V485, W01, –06, –10, –11, –12, –13, –16, –18, W24, Y31, Y850, Y859, Y86, Y870, –1, –2. SCI: spinal cord injury. |
The underlying causes of death (E801A–B, E8120, E8162, E880A, E881A, E883A, E889A, E929E, F–H–I, V484,V485, W01, –06, –10, –11, –12, –13, –16, –18, W24, Y31, Y850, Y859, Y86, Y870, –1, –2) were coded by the injuries causing the SCI in 29.6% of cases.
Table III presents the causes of these 124 deaths.
| Table III. Underlying causes of death by initial trauma (n = 124) |
| Direct cause of death | Tetraplegia, n = 91 | Paraplegia, n = 33 |
| Male n = 77 n (%) | Female n = 14 n (%) | Male n = 30 n (%) | Female n = 3 n (%) |
| Pneumonia | 38 (17) | 8 (24) | 7 (5.1) | 0 (0) |
| Emboli | 8 (3.6) | 0 (0) | 3 (2.2) | 0 (0) |
| Septicaemia | 5 (2.2.) | 1 (3.0) | 5 (3.6) | 2 (7.7) |
| Urology | 3 (1.3.) | 0 (0) | 3 (2.2) | 1 (3.8) |
| Miscellaneous | 23 (10.3) | 5 (15.2) | 12 (8.6) | 0 (0) |
There were 13 cases of pressure sores (PU) in the miscellaneous group. Eleven cases of PU were documented to be a first or second contributing factor and only two cases were determined to be a direct cause of death.
Survival
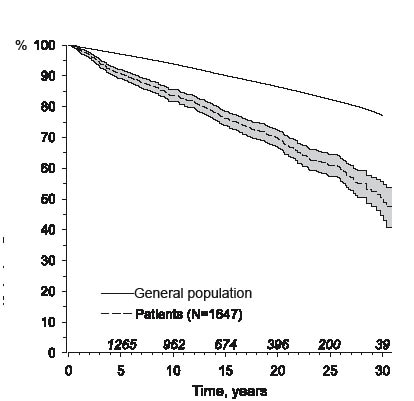
Fig. 1 presents survival curves for the study population and the general population. The survival rate for persons with SCI was 40% and for the general population 84%.
Fig. 1. Survival of persons with spinal cord injury admitted to Käpylä Rehabilitation Centre and survival of general population. Gray band gives the 95 per cent confidence interval for the patients survival.
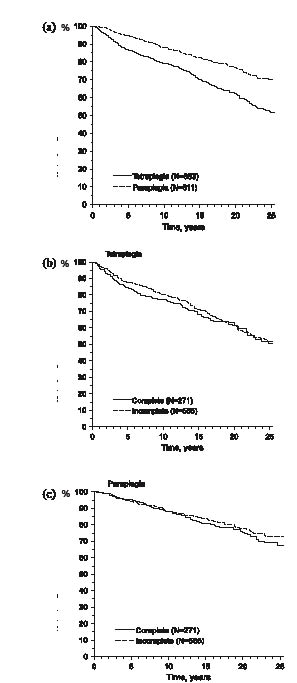
Survival rates for persons with paraplegia and tetraplegia are shown in Fig. 2a. Over a 25-year period, the survival rate for persons with paraplegia was 71% and for those with tetraplegia 54%. Fig. 2b shows the survival of persons with tetraplegia and Fig. 2c the survival of persons with paraplegia with complete or incomplete SCI.
Fig. 2. (a) Survival of persons with paraplegia and tetraplegia. Age- and sex-adjusted hazard ratio (HR) = 1.51 (95% confidence interval (CI) 1.24–1.85), p < 0.001. (b) Survival of persons with tetraplegia with incomplete and complete spinal cord injury. Age and sex adjusted HR = 2.11 (95% confidence interval (CI) 1.61–2.77), p < 0.001. (c) Survival of persons with paraplegia with incomplete and complete spinal cord injury. Age and sex adjusted HR = 1.40 (95% CI 1.02–1.91), p = 0.036.
Standardized mortality ratios
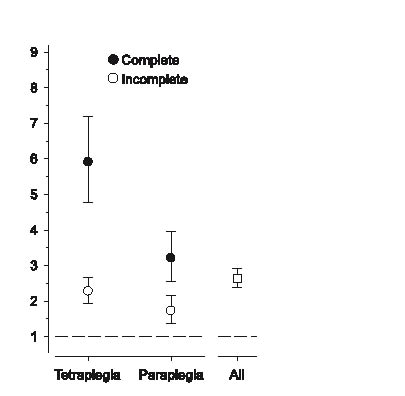
SMRs are presented in Fig. 3. The mean SMR was 2.65 (95% confidence interval (CI) 2.40–2.92). SMRs were higher for women and persons with tetraplegia. The ratio for women was 3.56 (95% CI 2.71–4.60) and for men 2.54 (95% CI 2.29–2.82). The SMR for persons with tetraplegia was 2.97 (95% CI 2.62–3.35) and for persons with paraplegia 2.27 (95% CI 1.93–2.64).
Fig. 3. Standardized mortality ratios for persons with complete and incomplete spinal cord injury.
Table IV shows a Cox regression model for risk indicators for death.
| Table IV. Cox regression model for risk indicators for death |
| Variable | Hazard ratio (95% CI) | p-value |
| Male | 1.36 (1.03–1.79) | 0.032 |
| Age at onset of injury, years | 1.06 (1.05–1.07) | < 0.001 |
| Aetiology of injury Traffic Fall Diving Violence Other | 1.00 (ref.) 1.35 (1.08–1.68) 0.78 (0.46–1.31) 1.52 (0.80–2.90) 1.01 (0.71–1.44) | 0.030 |
| Neurological level Paraplegia Tetraplegia | 1.00 (ref.) 1.75 (1.42–2.16) | < 0.001 |
| Completeness of traumatic spinal cord injury Incomplete Complete | 1.00 (ref.) 1.81 (1.45–2.23) | < 0.001 |
| 95% CI: 95% confidence interval. | | |
Discussion
Mortality and long-term survival among patients with TSCI who had entered the rehabilitation phase were evaluated. The study was based on a national TSCI population. Since the 1960s, the Käpylä Rehabilitation Centre has been the only national rehabilitation centre in Finland providing care to patients with SCI immediately after the acute hospital phase. This is in accordance with the official recommendation of the Finnish Ministry of Social Affairs and Health.
The results of this study supplement those of previous studies on mortality among TSCI patients, by showing that determinants of survival are influenced by several multivariate factors. Age at injury, gender, neurological level, and extent of lesion were important predictors of mortality. Other authors (2–6, 9,11, 12) report similar findings. Survival was better for persons with incomplete lesions, for paraplegic patients and for women.
Mortality in the study population was very high. Every fourth patient with TSCI had died by the end of follow-up. The overall survival rate in TSCI was approximately half that of the general population and was also lower than seen in some other studies (3, 5). The causes of deaths that had the greatest impact on reduced life expectancy for the study population were pneumonia, cardiovascular disease and suicide/poisoning, which is consistent with other published findings (3, 4, 7, 8, 12).
Our data showed markedly elevated SMRs for tetraplegic patients and for women. The 25-year survival was 1.3 times higher in paraplegia than in tetraplegia. These findings indicate that approximately 3 times as many deaths occurred in tetraplegic patients and more than 3 times as many deaths occurred in TSCI females than were expected in the general population. Lidal et al. (4) and Hagen et al. (12) also documented higher SMRs in women than men.
Surprisingly, the registry of causes of death revealed a high number of cases (30%) with inadequate descriptions of cause of deaths. In particular, the underlying cause was described by initial injury (the initial injury causing the spinal cord lesion). These cases were examined and the direct cause of death (e.g. pneumonia, septicaemia, emboli) was used to describe the cause of death in our analyses (Table III).
Of the total sample, the leading causes of death were respiratory disease (2, 3, 4, 6, 7), especially pneumonia, when underlying and all direct causes were considered together. Pneumonia was the most common cause of death, and contributed most to death in a recent study, but was the dominating underlying cause in only 8.6% of cases. Persons with tetraplegia died most frequently from pneumonia, a findings that was reported by other studies (2, 5, 6). Because of the predominance of pneumonia as a cause of death, more attention should be paid to the prevention and treatment of respiratory complications of SCI.
Cardiovascular disease was the second leading cause of mortality, accounting for 21% of deaths, which was consistent with previous findings (2, 3, 4, 6). The most common underlying cause of death was cardiovascular disease. In the general Finnish population, heart disease-related deaths account for 50% of all deaths.
Suicide (10.3%) and intoxication (6.7%) are prominent causes of death in this study. A surprising and significant finding was that suicide was the most common cause of death (27%) among female patients with paraplegia. Soden et al. (7) reported a greater risk of suicide for individuals with tetraplegia, whereas DeVivo et al. (6) showed that suicide was the second leading cause of death in individuals with paraplegia and in the youngest age group. It is noteworthy that suicides is the most common cause of death among non-disabled persons in the under-30 years age group in Finland, and mortality from suicide is approximately 0.02% in the general Finnish population. A few recent studies have reported suicides and unintentional injuries among patients with SCI to be considerably higher than in the general population (3, 4, 7, 12).
Approximately 60% of cases of intoxication were caused by alcohol and the rest were caused by various medicines. It may be that some cases of intoxication caused by medicines could also be suicides. In Finland, clinical interventions should be directed at prevention of suicides and accidental intoxication. One way is to improve community integration among patients with SCI. It is important to increase awareness of suicide following SCI and focus information about suicide among follow-up services, patients themselves and their family members.
Patients with SCI generally have a higher risk of urinary infection, but deaths from urinary diseases accounted for a small proportion of the causes of death in this study (only 3.1%, with underlying and direct causes combined). Urinary tract complications were a contributing factor in 13 cases of deaths. One reason for the very few urological deaths could be the use of antibiotics and intermittent catheterization over the decades. International comparisons also show that urinary complications leading to deaths have diminished (3, 6). We also found a low number of pressure sores as a cause of death, which can be explained by the good public healthcare and careful nursing available to all patients.
The importance of psychosocial and educational rehabilitation, including follow-up services and psychiatric evaluation, must be emphasized. Risk indicators, such as higher age, tetraplegia, complete SCI and alcohol, are found in our data. The causes of mortality in our study reflect the same trends as have been reported in previous studies (4, 12). Targeted strategies for identifying injury-related factors and evaluating lifestyle need to be developed. Pre-injury medical condition, secondary health conditions after SCI, a low quality of life and risk behaviours are known determinants of mortality among patients with SCI (4, 10, 11, 13). These factors can be treated and prevented.
Aetiology of injury was not found to be a significant risk factor for death, although the opposite findings have also been observed (6, 9).
There are some limitations of the present study. First, the study did not identify deaths occurring during transfer to an acute care and in hospitals. Secondly, we did not systematically gather information about secondary complications among TSCI patients. There is lack of detailed data on pre-existing medical co-morbidities. Thirdly, despite centralized rehabilitation for TSCI patients, some elderly or otherwise severely injured patients are probably not referred to the Käpylä Rehabilitation Centre. Therefore we were unable precisely to estimate the total number of TSCI patients.
Differences in analytical methods and study settings, such as time from injury and follow-up period, and limitations in the data available from death certificates, reflect a need for uniformity of data collection and methodologies to facilitate international comparisons.
Despite the above-mentioned limitations, our study confirmed previous findings that patients with SCI have a reduced life expectancy compared with the general population.
References