OBJECTIVE: To compare the benefits of home physiotherapy, institution-based physiotherapy and no physiotherapy following hip fracture surgery.
DESIGN: Systematic review and meta-analysis of randomized controlled trials.
METHODS: Two reviewers independently extracted data from 5 included studies. Standardized mean differences were pooled for health-related quality of life and performance-based outcomes. Review Manager Version 5 was used for data analysis.
RESULTS: Analysis of the 5 included studies indicated that home physiotherapy was better than no physiotherapy and similar to outpatient physiotherapy in improving patient-reported health-related quality of life. Performance-based outcomes were marginally better following outpatient physiotherapy compared with home physiotherapy 3 and 6 months after surgery. The risk of bias was high for most outcomes due to methodological issues in the included studies.
Discussion: There was a trend of better results with increasing intensity of physiotherapy intervention, but this did not convert into significant effect sizes. The results of this review do not build a strong consensus for recommending one mode of physiotherapy over the others. The quality of evidence was low mainly due to the high risk of bias in the included studies.
CONCLUSION: In light of no strong consensus, physiotherapists should continue to follow their current workplace practice policies for determining suitable discharge settings.
Key words: hip fracture; home physiotherapy; health-related quality of life; rehabilitation.
J Rehabil Med 2011; 43: 477–480
Correspondence address: Saurabh P. Mehta, School of Rehabilitation Science, McMaster University, Hamilton, Ontario, Canada, L8S 1C7. E-mail: mehtas8@mcmaster.ca
Submitted November 10, 2010; accepted March 2, 2011
introduction
Hip fracture usually results from a fall and is common in older adults (1). Surgical interventions following hip fracture are known to enhance the recovery process, reduce hospital stays and lead to improved outcomes, and therefore are preferred over conservative management (2).
Physiotherapy (PT) is an essential aspect of care following hip fracture surgery; the goals of PT are to improve mobility, strength, balance, and achieve independence in functioning. PT interventions are provided in either inpatient, outpatient, or home settings. Previous studies that examined the advantages of different PT settings following hip fracture surgery have yielded conflicting results, in that some recommend intensive outpatient PT (3), whereas others find that intensive outpatient PT is beyond the capacity of certain individuals (4). PT services provided at home have many benefits over institutionalized care and fit well within the context of “aging at home” as a healthcare policy option (5). However, it is not clear whether home PT is equally effective compared with other modes of PT services following hip fracture surgery. The aim of this meta-analysis was to examine the benefits of home PT compared with other modes of delivery of PT (inpatient, outpatient, and no treatment) following hip fracture surgery.
Methods
Only parallel design randomized control trials (RCTs) were included in this review. The intervention of interest was home PT monitored by physiotherapists following hip fracture surgery. Inpatient PT, outpatient PT, and no intervention were the comparators. Patient-reported health-related quality of life (HRQOL) and performance-based measures such as ambulatory capacity, lower limb muscle strength, and balance were the outcomes of interest. Studies were excluded if the home intervention was multidisciplinary in nature or patients had elective hip surgery. Trials that recruited patients 5 months or more after hip fracture surgery were excluded since patients may have previously received other interventions that could impact the final outcome.
MEDLINE, CINAHL, EMBASE, and the Cochrane Central Register of Controlled Trials databases were searched using a combination of keywords and Medical Subject Headings. Hand searching of reference lists of the included studies was used to identify other potential studies. Citations obtained from the search were screened by two independent reviewers (SM and J-SR). Disagreements between the reviewers were resolved by discussion to reach a consensus. Agreement between the two reviewers was determined using the unweighted kappa (κ).
Relevant details for participants, intervention, comparators, and outcomes were collected using a standardized data collection form. Criteria described by the Cochrane Collaboration for assessing risk of bias in domain-based evaluation were used. Generation of randomization sequence, concealment of treatment allocation, blinding, completeness of outcome data, and selective outcome reporting were the domains assessed. Risk of bias in each domain was classified as low, unclear, and high (6). I square (I2) was used to assess inconsistency between the included studies; I2 < 60% was considered to be acceptable for pooling the data (7).
Standardized mean differences (SMD) were used to compare the outcomes. Data for all the outcomes was pooled and analysed for the included studies. In the study in which SMD was not reported (8), the values were either imputed from one of the included studies (9) or derived from the age-adjusted normative values described in the literature (10). These strategies for imputing SMD are recommended by the Cochrane Collaboration. Of the 3 comparators, the inpatient and outpatient PT are clearly more intensive compared with no PT. Therefore, it would have introduced a bias had we kept them in the same group while comparing them with the home PT. Subgroup analyses (e.g. institution-based physiotherapy (inpatient or outpatient PT) or no PT) were planned a priori to avoid this bias.
Inverse-variance random effects model was used considering the differences in the nature of PT intervention, treatment frequency, and type of exercises across the included studies. Review Manager Version 5 was used for data analysis. Confidence intervals (CI) at 95% were calculated for pooled estimates for each outcome and Z test was used for determining the treatment effect. The statistical significance was considered at p ≤ 0.05.
Results
Of the 952 studies retrieved after the preliminary search, 935 studies were excluded after abstract review. Seventeen studies were included for the full-text review. Five met the pre-determined inclusion/exclusion criteria and were included (8, 9, 11–13). An unweighted κ of 0.81 (excellent agreement) was obtained between the reviewers in identifying the relevant studies.
Of 5 studies included, the comparator group was outpatient PT in 2 studies (8, 9), inpatient PT in 1 (11) and no PT in 2 (12, 13). Home PT was provided as a control intervention in 2 studies (8, 9) and as the treatment intervention in 3 (11–13). A description and the characteristics of the included studies are shown in Table I.
|
Table I. Characteristics of included studies
|
|
Study
|
Participants
|
Intervention/Comparison
|
Outcomes
|
Results
|
|
Binder 2004 (9)
|
n = 90 (46 outpatient PT; 44 home PT)
|
Home PT – flexibility exercises performed 3 ×/week or more
Outpatient PT – strength, flexibility, balance, and coordination exercises in phase 1; progressive resistance training in phase 2
|
SF-36, Hip Rating Questionnaire, FSQ, BADL, Berg Balance Scale, maximum walking speed, and modified PPT
|
Outpatient therapy group had greater improvement in most of the outcomes
|
|
Carmeli 2006 (8)
|
n = 63 (34 outpatient PT; 29 home PT)
|
Home PT – 50 min exercise sessions performed 3 ×/week
Outpatient PT – same exercise, but supervised by physiotherapists
|
SF-36, Functional reach test, basic PPT
|
Though both groups showed improvement in functions and self-reported health status, class-based group had slightly better outcomes
|
|
Kuisma 2002 (11)
|
n = 81 (41 institution PT; 40 home PT)
|
Home-based PT and inpatient PT. No clear description of exercises
|
Ambulatory ability measured across 5 categories
|
Ambulatory ability was better in the home PT
|
|
Mangione 2005 (12)
|
n = 41 (13 ATE; 17 RTE; 11 no PT)
|
Home PT – one group received aerobic exercises and the other received resistance training exercises
No PT control – bi-weekly mailings of the National Institutes of Health “Age Pages” for non-exercise topics
|
SF-36 physical function scale, gait speed, 6MWT, strength
|
Endurance, gait speed, and self-reported functions improved in both the groups, but muscle strength improved more in the home PT groups.
|
|
Tsauo 2005 (13)
|
n = 54, (28 no PT; 26 in home PT)
|
Home PT – exercises to improve muscle strength, balance, ROM, functions, transfers, and adaptation to home setting
No PT – patients advised to continue exercise programme given at bedside before discharge
|
WHOQOL – BREF, Harris Hip Score, gait speed, ROM, and strength
|
HRQOL and functions improved for the home physiotherapy group, whereas muscle strength, ROM, and walking speed remained same for both the groups
|
|
PT: physiotherapy; SF-36: Short Form 36; HRQOL: Health-related Quality of Life; FSQ: Functional Status Questionnaire; BADL: basic activities of daily living; PPT: Physical Performance Test; ATE: aerobic training exercise; RTE: resistance training exercise; ROM: range of motion; 6MWT: 6-minute walk test; WHOQOL – BREF: World Health Organization Quality of Life Measure – Abbreviated version.
|
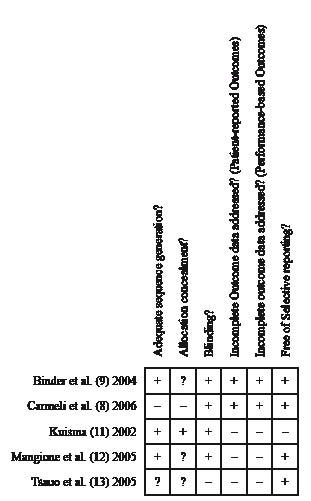
Agreement between reviewers was excellent (unweighted κ = 0.86) in assessing risk of bias across studies. Fig. 1. provides a pictorial representation of risk of bias assessment for the included studies. Overall methodological quality assessment indicated that risk of bias was unclear in 1 study (9) and high in the other 4 (8, 11–13).
Fig. 1. Methodological quality of included studies. +: low risk of bias; –: high risk of bias; ?: unclear risk of bias.
Outcomes at 3 months
For the HRQOL, there was no difference between the outpatient PT and home PT groups (SMD 0.2; 95% CI: –0.53, 0.13; p = 0.23; I2 = 0). Conversely, effect size was moderate and significant in favour of home PT compared with the no PT group (SMD 0.68; 95% CI: 0.12, 1.24; p = 0.02; I2 = 0). There was no difference in the walking speed between the home PT and no PT groups (SMD 0.15; 95% CI: –0.39, 0.69; p = 0.58; I2 = 0) (12, 13). Only 1 study in the outpatient PT group assessed walking speed, which showed moderate and statistically significant effect size in favour of outpatient PT compared with the home PT group (SMD –0.44; 95% CI: –0.85, –0.02; p = 0.04) (9). There was no difference between the home PT and no PT groups in lower extremity muscle strength (SMD 0.0; 95% CI: –0.54, 0.54; p = 0.99; I2 = 0) (12, 13). Balance was similar in the outpatient PT and the home PT groups (SMD 0.05; 95% CI: –0.58, 0.47; p = 0.84; I2 = 59) (8, 9).
Outcomes at 6 months
One study in each subgroup reported HRQOL at 6 months (9, 13). Therefore meta-analysis was not possible. Binder et al. (9) indicated that HRQOL was better in outpatient PT compared with the home PT group (SMD –0.47; 95% CI: –0.89, –0.05; p = 0.03). Those in the home PT group had significantly better HRQOL compared with the no PT group (SMD 1.01; 95% CI: 0.17, 1.85; p = 0.02) (13). Walking speed at 6 months was reported in two studies: 1 (9) reported a moderate but significant effect on walking speed in those who received outpatient PT (SMD –0.56; 95% CI: –0.98, –0.14; p = 0.009), while the other (13) concluded that home PT was no different from no PT (SMD –0.04; 95% CI: –0.74, 0.83; p = 0.92). One study reported lower extremity muscle strength at 6 months (13). A small but insignificant effect size was observed favouring home PT compared with no PT (SMD –0.24; 95% CI: –0.55, 1.03; p = 0.55). Balance was assessed in one study, which reported significant effect size favouring outpatient PT compared with home PT (SMD –0.60; 95% CI: –1.02, –0.17; p = 0.006) (9).
Study excluded from meta-analysis
The study conducted by Kuisma (11) met the inclusion/exclusion criteria, but was not included for several reasons. The study had proposed to assess the ability to walk with or without assistive devices on the scale of 0–4 in 5 conditions, but selectively reported data for only 2 (11). Furthermore, the outcome used in the study for assessing walking ability was developed by the authors for the purposes of the study without investigating the psychometric properties of the outcome.
Adverse events
Binder et al. (9) reported 3 adverse events directly related to outpatient PT: two patients sustained fractures (rib fracture resulting from a fall during exercise session and metatarsal bone fracture that became symptomatic after few days following exercise session) and one patient developed ecchymosis resulting from weight-training exercises. The other studies did not report any adverse events.
DISCUSSION
Results of this meta-analysis indicate that patient-reported HRQOL in home PT was better compared with no PT and similar compared with outpatient PT at 3 months. Performance-based outcomes were better in outpatient PT compared with home PT based on one study (9). Similar trends were observed at 6 months; however, meta-analysis of the data at 6 months was not possible. No study examining inpatient PT vs home PT was deemed appropriate to be included in the review.
All outcomes pointed towards better results with increasing intensity of PT intervention (outpatient PT > home PT > no PT), but few significant effect sizes were observed. However, home PT should be recommended over no PT based on the improvement in HRQOL. Though outpatient PT yielded better results for performance-based outcomes, it should be carefully recommended for those who are frail as they may have difficulties tolerating the intensive nature of such intervention (4) and could be more prone to injuries (9). The results of this review did not build a strong consensus in favour of one PT intervention over the others, given that the completeness of the evidence was affected by the small number of studies, the availability of data for only short-term outcomes, and the small-to-moderate effect sizes observed.
The quality of evidence was assessed using criteria recommended by GRADE Working Group (14). The quality of evidence was also affected by the poor methodological qualities of the studies. In particular, allocation concealment and incomplete reporting of outcome affected the quality of evidence emerging from this review. Overall quality of evidence was moderate to very low for all outcomes.
A comprehensive search strategy, duplication in literature search and eligibility assessment, and agreement in selecting studies and assessing risk of bias are some of the strengths of this review. Data dictionary and data extraction forms were developed for consistency between reviewers.
However, there were some limitations of our review. The number of PT sessions provided, nature and frequency of exercises, adherence to the exercises, duration between surgery and the start of PT intervention, and the expertise/skills of physiotherapists providing the intervention are some of the variations observed between the included studies. The current review did not consider these variations while estimating the treatment effect; thus it could have introduced bias. This is even more critical when it appears that the intensity of PT intervention could have influenced outcomes. However, these studies were pragmatic in nature and simulated the routine approach adopted while delivering home PT or outpatient PT. Therefore, the variations in the nature, frequency, and intensity of PT were disregarded for a realistic comparison between the intervention groups.
To our knowledge, no previous review has examined the benefits of home PT following hip fracture surgery. Our results are in agreement with a different, but related, review conducted by Handoll et al. (15), suggesting that the intensity of PT intervention is important in achieving better outcomes following hip fracture surgery. Conversely, intensive PT may not be suitable for certain patients and can result in adverse events and poor compliance (4). However, optimal strategies and intensity of PT intervention need to be investigated. In particular, it needs to be ascertained whether properly designed home PT can yield comparable outcomes to those resulting from outpatient or inpatient PT.
In conclusion, our results support home PT compared with no PT in improving patient-reported HRQOL outcomes following hip fracture surgery. When making a comparison between home PT and outpatient PT for HRQOL, our results do not lead to the recommendation of one approach over the other. Therefore, physiotherapists should continue to follow the current practice policies employed at their workplace for determining the suitable discharge setting. The low-quality evidence emerging from this review suggests the need for well-designed and pragmatic RCTs to examine the benefits of home PT with direct comparison with institution-based PT and no PT. In particular, future studies should give importance to allocation concealment and complete data reporting while conducting the trial and reporting the results. Although it was not a part of our review, future studies should also compare cost-effectiveness across different PT interventions.
ACKNOWLEDGEMENTS
Funded by Quality of Life Training Program, Canadian Institutes of Health Research and Musculoskeletal Pain Grant, Canadian Institutes of Health Research, Literature Review Grant from Community Rehab, Ontario, Canada.
References