OBJECTIVE: This pilot study investigated whether a home exercise video programme could improve exercise tolerance and breathlessness in patients with moderate to severe chronic obstructive pulmonary disease.
METHODS: Twenty subjects completed the study after being randomized to intervention or control. The intervention group (n = 10), watched a 19-min video on the benefits of exercise for patients with chronic obstructive pulmonary disease and were given a 30-min exercise video, an illustrated exercise diary and an educational booklet about chronic obstructive pulmonary disease, for use at home. They were advised to follow the exercise video programme 4 times a week for 6 weeks. The control group (n = 10) received the chronic obstructive pulmonary disease educational booklet only. Exercise tolerance was measured using the Incremental Shuttle Walk Test and breathlessness by the self-reported Chronic Respiratory Questionnaire.
RESULTS: The median change in the Incremental Shuttle Walk Test and breathlessness score significantly improved in the intervention group compared with the control (+45 m vs –15 m, p = 0.013 and +0.5 vs –0.1 Chronic Respiratory Questionnaire units, p = 0.042). The other findings for the self-reported Chronic Respiratory Questionnaire showed significant improvements in the intervention group for emotion (p < 0.001) and fatigue (p = 0.012), but not mastery (p = 0.253).
CONCLUSION: This pilot study suggests that participation in a home exercise video programme may benefit people with chronic obstructive pulmonary disease.
Key words: exercise, breathlessness, pulmonary disease, chronic obstructive, rehabilitation, video.
J Rehabil Med 2009; 41: 195–200
Correspondence address: Julie Moore, Pulmonary Rehabilitation Team, Dulwich Hospital, East Dulwich Grove, London, SE22 8PT, UK. E-mail: pulmonary.rehab@kch.nhs.uk
Submitted May 2, 2008; accepted September 30, 2008
INTRODUCTION
Pulmonary rehabilitation (PR) has been shown to deliver cost-effective improvements in dyspnoea, exercise tolerance and health-related quality of life in people with chronic obstructive pulmonary disease (COPD) (1, 2). PR programmes in the UK are typically delivered on an outpatient basis, either at a hospital or at a suitable site in the community. It is not always possible, however, for patients to access outpatient programmes due to lack of local availability or adequate transport from isolated locations. Severe breathlessness may reduce activity levels to such a degree that, for many, leaving the house is an ordeal. A British Lung Foundation (BLF) survey reported that less than 2% of UK patients with COPD had access to a rehabilitation exercise programme (3), despite National Institute for Health and Clinical Excellence (NICE) and British Thoracic Society (BTS) recommendations that PR be made available to all patients who are functionally limited by dyspnoea.
Access to the benefits of PR may be broadened if effective exercise could be administered at home. Current evidence suggests that home-based rehabilitation interventions result in smaller benefits as judged by exercise tolerance and quality of life when compared with supervised programmes (4–6). The impact of home-based rehabilitation may be limited by multiple factors, including lack of healthcare supervision and support from fellow COPD sufferers. This may lead to poor adherence to prescribed exercise intensity and frequency in home programmes (5, 7, 8).
One-to-one supervision on an individual basis is unlikely to be feasible or cost-effective; however, use of a home exercise video could enhance adherence to prescribed exercise programmes. Video media can be an effective means of delivering exercise instruction (9). No published research to date has investigated the effectiveness of a home exercise video for patients with COPD. We hypothesized that an exercise programme based on video instruction at home could improve walking ability, breathlessness and quality of life.
METHODS
Patients
Patients with a clinical and spirometric diagnosis of COPD, with a Forced Expiratory Volume in one second divided by Force Vital Capacity (FEV1/FVC) < 70% and %predicted FEV1 < 60%, were recruited from a PR programme waiting list. Referrals to the PR programme were from hospital respiratory physicians, community-based general practitioners and other healthcare professionals. All referrals were screened for co-morbid conditions that would preclude safe exercise training at home, including significant cardiac disease and cognitive impairments (10). Patients who had not previously attended PR and who had access to a Video Home System (VHS) or Digital Video Disc (DVD) player at home were recruited. All patients gave informed consent and the study protocol was approved by the University of Brighton School of Health Professions Ethics Panel and King’s College Hospital Research Ethics Committee. All patients were offered standard PR at the end of the study period.
Study design
Patients were assessed by a senior physiotherapist who decided whether they were safe to participate in the study. To ensure that all patients were safe to exercise at home alone, any patient with high blood pressure (> 180/100), high heart rate (> 100) or low oxygen saturations (< 88%) were excluded from the study. An Incremental Shuttle Walk Test (ISWT) was performed by all patients as described by Singh et al. (10). One practise walk was undertaken to allow familiarization. Dyspnoea associated with daily function and disease-specific quality of life was assessed through the Self-Reported Chronic Respiratory Disease Questionnaire (CRQ-SR) (11).
Patients were randomized to either intervention or control using a concealed minimization strategy to match the groups for age (≤ 65 or > 65 years) and airway obstruction (≤ FEV1 40% or > FEV1 40%). The randomization was sent to the chief investigator via sealed envelopes and was not revealed until patients had completed baseline assessment.
Intervention
Patients randomized to the intervention group participated in a home exercise video programme. This programme consisted of watching a 19-min video (Video A) about the benefits of exercise in COPD. Video A showed patients with COPD describing their own experiences of exercising, highlighting their anxieties and the benefits of exercise. The video also utilized members of the multidisciplinary rehabilitation team to deliver education about the benefits of exercise in COPD, provide motivation and alleviate concerns about exercising. Patients watched the video alongside a physiotherapist with whom they could discuss any questions that arose. They were then given a 30-min exercise video or DVD (Video B) to take home and use 4 times a week for a period of 6 weeks. All patients in the intervention group were shown how to perform the exercises on the video. They were advised to stop if they experienced any pain, dizziness or generally feeling unwell while performing the exercise video and to contact the study physiotherapist at the earliest availability or a doctor in an emergency. The exercise video is designed so that the patient could watch it and perform the exercises in front of a television. The video consisted of a warm-up, high-intensity interval exercises (upper and lower-limb strengthening and aerobic exercise) and a cool-down including stretches (Table I). Instruction and demonstration of the exercises on the video were provided by a physiotherapist assisted by 2 patients with COPD (one male and one female; the female patient required supplemental oxygen therapy).
| Table I. Exercises included in video B |
| Exercise video regime | Exercise | Repetitions or time | Intensity |
| Warm up (joint mobilizer) Warm up (circulatory) | Shoulder shrugs | 2 | Borg 2–3 “Slightly to moderately breathless“ |
| Head turns | 2 |
| Side bends | 2 |
| Shoulder shrugs | 2 |
| Head turns | 2 |
| Side bends | 2 |
| Marching on spot* | 45 sec |
| Heel digs* | 45 sec |
| Marching on spot* | 45 sec |
| Side step taps* | 45 sec |
| Marching on spot* | 45 sec |
| Back step taps* | 45 sec |
| Rest 30 sec |
| Main exercise regime | Arm raise to the side with weights | 1 min | Borg 4 “Somewhat severely breathless or tired” |
| Squats | 1 min |
| Marching on spot† | 1 min |
| Rest (forward leaning) | 30 sec |
| Upright row with weights | 1 min |
| Heel raises | 1 min |
| Modified star jumps | 1 min |
| Rest (forward leaning) | 30 sec |
| Wall push offs | 1 min |
| Sit to stand | 1 min |
| Marching on spot† | 1 min |
| Rest (forward leaning) | 30 sec |
| Bicep curls with weights | 1 min |
| Seated knee extension | 1 min |
| Modified star jumps | 1 min |
| Rest (forward leaning) | 30 sec |
| Cool down (circulatory) | Marching on spot | 30 sec | Borg 3 “Moderately breathless“ |
| Heel digs | 30 sec |
| Marching on spot | 30 sec |
| Side step taps | 30 sec |
| Marching on spot | 30 sec |
| Back step taps | 30 sec |
| Rest 30 sec |
| Stretches | Shoulders | 30 sec | |
| Triceps | 30 sec |
| Pectorals | 30 sec |
| Back | 30 sec |
| Thoracic | 30 sec |
| Lumbar | 30 sec |
| Hamstrings | 30 sec |
| Gastrocnemius | 30 sec |
| *Bicep curls optional. †Forward punches optional. |
The videos used in this study were designed by the Pulmonary Rehabilitation Team from King’s College Hospital, Southwark Primary Care Trust (PCT) and Lambeth PCT and were made by Realta Productions (London, UK). A short version of Video A and details for accessing Video B are available on the Internet (www.kch.nhs.uk/services/general-medicine/therapy-services/physiotherapy/pulmonary-rehabilitation).
The intervention group were also provided with supporting literature, including an illustrated BLF exercise diary to monitor exercise frequency and an educational booklet about COPD produced by King’s College Hospital. The topics included in this booklet were; an explanation of COPD, diagnosing and treating COPD, medications for COPD, oxygen therapy, managing chest infections, how to manage breathlessness, stress and relaxation, exercise and smoking cessation.
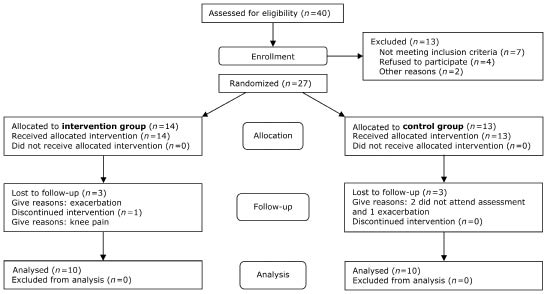
The control group received the educational COPD booklet only. All patients received individual consultation with the study physiotherapist, allowing equal opportunity for discussion relating to COPD management. Any patient that experienced an exacerbation of their respiratory symptoms during the study period was advised to telephone the study physiotherapist and was excluded from the study (Fig. 1).
Exercise intensity and monitoring of adherence
Patients were familiarized with the Borg breathlessness scale and this was referred to throughout the exercise regime, to encourage the patient to work towards a symptom-limited intensity (12). Consistent and specific instructions were given to the subject to get “somewhat severely out of breath” and “somewhat severely tired”, corresponding to a Borg score of 4, which has been shown to be an appropriate training intensity (13–17). For the limb strengthening exercises, patients were given advice at the baseline assessment about household items that could be used as a weight to provide resistance, for example filled water bottles, and further advised on how to increase workload in a progressive manner to achieve the required training intensity. Additional advice was given on breathlessness management techniques, for example, leaning forward to assist recovery from dyspnoea (18). Adherence to the intervention was recorded prospectively in self-reported patient diaries. No minimum period of use was predefined as “completion” for inclusion in the final analysis, and all patients randomized to intervention were included regardless of how often the video was used.
Statistical methods
Comparisons were made between the intervention and control group for baseline characteristics (age, FEV1, ISWT and CRQ data) using Mann-Witney tests. Changes in CRQ and ISWT over the study period were analysed within intervention and control groups using Wilcoxon signed-rank tests and between groups by Mann-Witney U-test. All calculations were performed using SPSS Version 14© (SPSS Inc.).
RESULTS
Subject characteristics
Twenty-seven patients were randomized, of whom 20 completed the study. Fig. 1 shows the flow of patients through the study. In the control group, 2 patients did not attend the follow-up assessment and one had an exacerbation. In the intervention group, 3 subjects had an exacerbation and one withdrew due to aggravation of knee pain. Of the 20 patients who completed final assessment, 10 were allocated to intervention and 10 to control; their baseline characteristics are shown in Table II. At baseline, groups did not differ significantly for age, sex, FEV1, %predicted FEV1, ISWT, CRQ dyspnoea score or Hospital Anxiety and Depression HAD score. At baseline, 2 patients in the control group and 4 in the study group had HAD scores suggestive of depression. Five patients in each group had scores suggestive of anxiety. The mean (standard deviation (SD)) follow-up time for the control group was 7 (1) weeks compared with 8 (3) weeks for the intervention group.
Fig. 1. Flow-chart showing patient participation throughout the study.
| Table II. Subject characteristics of the intervention (home exercise video) and control groups at baseline. Values given as median and inter-quartile range; p-values generated using Mann-Witney U-test |
| Variable | Control (n = 10) | Intervention (n = 10) |
| Age, years | 70.5 (57.5 to 78.5) | 70 (13) |
| Gender, male/female | 4/6 | 6/4* |
| % predicted FEV1 | 41.5 (30 to 55) | 40 (36.5 to 49) |
| FEV1, l | 0.96 (0.77 to 1.31) | 0.94 (0.66 to 1.17) |
| SaO2, % | 96 (93 to 97) | 96 (93 to 97) |
| MRCDS, 1–5 | 3.5 (2–4 to 25) | 4 (2.75 to 4) |
| HAD-ANX, 0–21 | 11.0 (3.5 to 13) | 7.5 (4 to 11) |
| HAD-DEP, 0–21 | 9 (1.5 to 12) | 5.5 (2.5 to 9.5) |
| Baseline ISWT, m | 160 (45 to 85) | 110 (30 to 270) |
| Baseline CRQ dyspnoea score (domain mean) | 2.7 (2 to 4.8) | 3.3 (1.8 to 4.1) |
| *p = 0.656 using Fisher’s exact test. ISWT: Incremental Shuttle Walk Test; CRQ: Chronic Respiratory Disease Questionnaire; HAD-ANX: Hospital Anxiety and Depression – Anxiety score; HAD-DEP: Hospital Anxiety and Depression – Depression score; FEV1, l: Forced expiratory volume in one second in litres; MRCDS: Medical Research Council Dyspnea Score. |
Change in walking capacity and self-reported symptoms
The group changes between baseline and follow-up assessment are summarized in Table III. Exercise tolerance, as measured by the ISWT and 3 domains of the CRQ (dyspnoea, fatigue and emotion), showed statistically significant improvements within the intervention group. No significant difference was observed in the mastery score of the CRQ (p = 0.06). None of these assessed outcomes improved in the control group. The changes in ISWT and CRQ dyspnoea, fatigue and emotion scores were significantly greater in the intervention group when compared with control. At follow-up, the number of subjects with HAD scores suggestive of depression was unchanged in either group; 2 subjects had scores suggestive of anxiety in the study arm. Mean HAD anxiety scores were unchanged in the exercise video group (–2.3 points, 95% confidence interval: –4.9 to 0.3, p = 0.078) or when compared with control (p = 0.211).
| Table III. Incremental Shuttle Walk Test (ISWT) distances and Chronic Respiratory Disease Questionnaire (CRQ) scores at baseline and follow-up, and within-group change, are expressed as median (inter-quartile range). For the within-group change, Wilcoxon signed-rank tests were used; differences between groups were examined using Mann-Witney U-tests. ISWT values are to nearest metre; CRQ values are presented as domain means and to the nearest 0.1 unit. Higher scores on the ISWT and CRQ domains denote improvement |
| | Control group | Intervention group | Between-group difference (p-value) |
| Baseline | Follow-up | Within-group difference | Baseline | Follow-up | Within-group difference |
| ISWT, m | 160 (48–288) | 175 (39–215) | –15 (–20–9) p = 0.256 | 110 (35–265) | 200 (69–333) | 45 (15–88) p = 0.021 | 0.013 |
| CRQ Dyspnoea | 2.7 (2.1–4.8) | 2.5 (2.0–3.2) | –0.1 (–1.5–0.3) p = 0.326 | 3.3 (1.8–4.1) | 3.6 (2.6–4.4) | 0.5 (0.2–0.6) p = 0.027 | 0.042 |
| CRQ Fatigue | 2.5 (2–4.6) | 2.5 (1.9–4.5) | 0.0 (–1.4–0.75) p = 0.74 | 2.9 (2–4.4) | 4.9 (4–5.1) | 1.7 (0.6–2.4) p = 0.004 | 0.012 |
| CRQ Emotion | 4 (2.4–5.8) | 4 (2.9–5.9) | 0.2 (–0.3–0.5) p = 0.73 | 4.4 (3.2–5) | 5.4 (4.8–6) | 0.8 (0.6–2.1) p = 0.002 | < 0.001 |
| CRQ Mastery | 3.5 (2.9–5.6) | 4.5 (3–5.4) | 0.8 (–0.9–1.1) p = 0.64 | 4.8 (4.1–5.5) | 5.4 (4.6–5.9) | 0.6 (–0.1–1.4) p = 0.06 | 0.253 |
Use of the home video intervention
The mean number of times that the video was used during the study period was 33 (range 8–70, SD 20). This data was self-reported and collected from patients’ diaries. Improvement in either ISWT or CRQ score was not correlated with the frequency of video use or any other baseline factor.
DISCUSSION
This study reports the impact of a home video led exercise programme in patients with COPD. The data suggest that such a programme can improve exercise capacity and breathlessness. The possible physiological mechanisms for the increase in exercise capacity observed in the home exercise group were not investigated. Limb strengthening exercises have been shown to increase peripheral strength in patients with COPD (19) and greater quadriceps muscle strength is associated with increased incremental shuttle walk performance (20). Although quadriceps muscle strength was not measured in this study, increased leg strength may contribute to the increased walking distance observed. The CRQ domain changes for dyspnoea, emotion and fatigue observed in the intervention group reached or exceeded accepted minimum clinically important differences (21, 22). Previous work has suggested that limb strengthening exercise generates larger improvements in disease-specific quality of life than aerobic training (23). Limb strengthening exercise was an important component of this home-based video programme and may have contributed to the improved CRQ domain scores as well as exercise capacity.
Regarding dyspnoea specifically, respiratory mechanics were not measured in this study and it is unclear whether delayed dynamic hyperinflation (14), for example, resulted from the exercise training programme. Conversely, more general advice given at the study outset regarding breathlessness management strategies, may have itself in part, contributed to the improved CRQ dyspnoea score. Parallel improvement in both CRQ dyspnoea and emotion scores is not surprising; a causal relationship between the development of symptoms of anxiety and breathlessness has been proposed (24). No significant change in anxiety scores was observed, although 3 out of the 5 patients in the intervention group, that had a positive score for anxiety at baseline, did show a clinically significant drop in anxiety score. The number of subjects is too small to make conclusive judgements on the intervention’s impact on anxiety or depression; further investigation is required in larger studies. No qualitative questioning of patients was performed to make further judgements as to why the emotional state of the home video group improved. Interestingly, the mastery component did not show a significant improvement in either group, which may be due to the lack of self-management strategies offered or a lack of sufficient exercise training.
Results are generally comparable to traditional PR programmes (22), but the aerobic exercises incorporated in the video (for example modified star jumps and marching on the spot) differ from those traditionally employed, such as walking or cycling. Exercises were chosen that could be performed within a confined indoor space with minimal equipment. It may be inferred that the exercises performed were largely responsible for the improved walking capacity; however, the effectiveness of the individual components needs further evaluation.
Proof of effective exercise intensity is a major challenge for home-based programmes. Patients had no direct supervision during the exercise other than the standardized guidance provided by the physiotherapist on the video, which largely relied on the Borg breathlessness scale alongside friendly encouragement. Although patients were given instruction on how to use the Borg scale, individual interpretation of the scale may differ over time and between patients. Similarly, weights selected for resistance-type exercises were self-determined by the patients. No formal progression of intensity or performance was prospectively recorded during training. The video-led exercise session (30 min) was relatively short compared with those described in many PR studies. Sessions were designed to exercise patients at a high intensity with short periods of recovery to achieve an effective training benefit (23).
Most studies of PR advocate 3 exercise sessions per week (19, 22, 25). UK recommendations advise that 2 supervised sessions and at least one other unsupervised session should be employed (10). The video-led exercise session (30 min) was relatively short; for this reason, 4 sessions per week were chosen in this study. However, the reported frequency of completed sessions each week varied widely and, there was no relationship between the amount of exercises reported and the degree of change in the outcome measures. The introductory video (Video A) given to the home video group may have led patients to perform more exercise outside of the video sessions but any additional exercise was not recorded in this study. Independent verification of how many exercises were truly performed was not possible in this study. The use of activity monitors may provide a more objective measurement of exercise frequency in future studies.
In addition to points already raised, the success of any unsupervised intervention at home is reliant on patient motivation: those who consented to participate in a study such as this may have been highly motivated. Additionally, participating patients were of moderate to severe severity: patients with less severe COPD may not achieve sufficient exercise intensity (above their usual level of physical function) when using an exercise video. Researchers were unable to remain blind to patient allocation during the study and at follow-up assessment. The impact of this is unknown; however, the CRQ is self-reported whilst the ISWT is a standardized, reproducible test (11, 26); results are certainly consistent with data from other types of unsupervised programmes (27–29). Larger studies including blinded follow-up assessment and a broader range of participant COPD severity would be insightful.
In conclusion, this pilot study shows that a home exercise video programme, following a single patient education session on the importance of exercise, can result in clinically meaningful improvements in walking distance, dyspnoea and other quality of life measures. Assuming that future studies are carried out to corroborate the effect of similar exercise video interventions (compared with a control group), we suggest that 25 cases per group will provide 90% power to detect a mean ISWT difference of 47 m, assuming a standard deviation of 50 m. These results are encouraging and the potentially cost-effective nature of this intervention is of interest. Patients who are unable to access a conventional outpatient PR programme may benefit from this approach. Patients wishing to maintain improvements after conventional PR may also benefit from home video led exercise in order to achieve this goal. Home-based video led exercise interventions represent an area suitable for further investigation and larger controlled studies with assessor blinding and longer follow-up periods are required to establish their efficacy. Comparison with traditional PR programmes in terms of clinical and cost effectiveness would also be informative.
ACKNOWLEDGEMENTS
We would like to thank the patients for their participation in making the videos and Realta Productions for directing them. We would also like to thank Southwark Primary Care Trust for funding the videos.
REFERENCES
1. American Thoracic Society/European Respiratory Society Statement on Pulmonary Rehabilitation. Am J Respir Crit Care Med 2006; 173: 1390–1413.
2. British Thoracic Society. Pulmonary rehabilitation. Thorax 2001; 56: 827–834.
3. British Lung Foundation. 2002. Pulmonary Rehabilitation Survey. http://www.lunguk.org/downloads/BLF_pul_rehab_survey.pdf
4. Cambach W, Chadwick-Straver R, Wagenaar RC, Van Keimpema ARJ, Kemper HCG. The effects of a community-based pulmonary rehabilitation programme on exercise tolerance and quality of life: a randomized controlled trial. Eur Respir J 1997; 10: 104–113.
5. Garrod R. The pros and cons of pulmonary rehabilitation at home. Physiotherapy 1998; 12: 603–607.
6. Wijkstra PJ, Altena R, Otten V, Kraan J, Postma DS, Koeter G.H. Effects of home rehabilitation on physical performance in patients with chronic obstructive pulmonary disease. Eur Respir J 1996; 9: 104–110.
7. Reardon J, Casaburi R, Morgan M, Nici L, Rochester C. Pulmonary rehabilitation for COPD. Resp Med 2005; 99: 19–27.
8. Spruit MA, Troosters T, Trappenburg JC, Decramer M, Gosselink R. Exercise training during rehabilitation of patients with COPD: a current perspective. Patient Educ Couns 2004; 52: 243–248.
9. Schoo A, Morris M E. The effects of mode of exercise instruction on correctness of home exercise performance and adherence. Physiotherapy Singapore 2003; 6: 36–43.
10. Singh S, Morgan M, Scott S, Walters D, Hardman A. Development of a shuttle walking test of disability in patients with chronic airways obstruction. Thorax 1992; 47: 1019–1024.
11. Williams J, Singh S, Sewell L, Guyatt G, Morgan M. Development of a self-reported chronic Respiratory Questionnaire (CRQ-SR). Thorax 2001; 56: 954–959.
12. Borg GAV. Psychological basis of perceived exertion. Med Sci Sports Exerc 1982; 14: 377–381.
13. Mejia R, Ward J, Lentine T, Mahler DA. Target dyspnoea ratings predict expected oxygen consumption as well as target heart rate values. Am J Respir Crit Care Med 1999; 159: 1485–1489.
14. Casaburi R, Porszaasz J, Burns MR, Carithers ER, Chang RS. Physiological benefits of exercise training in rehabilitation of patients with severe chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1997; 155: 1541–1551.
15. Horowitz MB, Littenburg B, Mahler DA. Dyspnoea ratings for prescribing exercise intensity in patients with COPD. Chest 1996; 109: 1169–1175.
16. Ries AL. Effects of pulmonary rehabilitation on physiological and psychological outcomes in patients with chronic obstructive pulmonary disease. Ann Intern Med 1995; 122: 823–832.
17. Wilson RC, Jones PW. Long-term reproducibility of Borg scale estimates of breathlessness during exercise. J Clin Science 1991; 80: 309–312.
18. Gigliotti F, Coli C, Bianchi R, Romagnoli I, Lanini B, Binazzi B, et al. Exercise training improves exertional dyspnoea in patients with COPD. Evidence of the role of mechanical factors. J Clin Invest 2003; 123: 1794–1802.
19. O’Shea SD, Taylor NF, Paratz J. Peripheral muscle strength training in COPD: a systematic review. Chest 2004; 126; 903–914.
20. Steiner MC, Singh SJ, Morgan MDL. The contribution of peripheral muscle function to shuttle walk performance in patients with COPD. J Cardiopulm Rehab 2005; 25: 43–49.
21. Jones PW. Interpreting thresholds for a clinically significant change in health status in asthma and COPD. Eur Respir J 1992; 19: 398–404.
22. Lacasse Y, Brosseau L, Milne S, Martin S, Wong E, Guyatt GH, et al. Pulmonary rehabilitation for chronic obstructive pulmonary disease. The Cochrane Database of Syst Rev 2001 (4): Art. No.: CD003793.DOI: 10.1002/14651858.CD003793.
23. Puhan MA, Schuemann Frey M, Scharplatz M, Bachmann LM. How should patients with COPD exercise during respiratory rehabilitation? Comparison of exercise modalities and intensities to treat skeletal muscle dysfunction. Thorax 2005; 60: 367–375.
24. Neuman A, Gunnbjornsdottir M, Tunsater A, Nystrom L, Franklin KA, Norrman E, et al. Dyspnea in relation to symptoms of anxiety and depression: a prospective population study. Respir Med 2006; 100: 1843–1849.
25. Mador MJ, Bozanat E, Aggarwal A, Shaffer M, Kufel TJ. Endurance and strength training in patients with COPD. Chest 2004; 125: 2036–2045.
26. Campo LA, Chilingaryan G, Berg K, Paradis B, Mazer B. Validity and reliability of the modified shuttle walk test in patients with chronic obstructive pulmonary disease. Arch Phys Med Rehab 2006; 87: 918–922.
27. Ferrari M, Vangelista A, Vedovi E, Falso M, Segattini C, Brotto E, et al. Minimally supervised home rehabilitation improves exercise capacity and health status in patients with COPD. Am J Phys Med Rehabil 2004; 83: 337–343.
28. Hernandez MTE, Rubio TM, Ruiz FO, Riera HS, Gil RS, Gomez JC. Results of a home-based training program for patients with COPD. Chest 2000; 118: 106–114.
29. Puente-Maestu L, Sanz ML, Sanz P, Cubillo JM, Mayol J, Casaburi R. Comparison of effects of supervised versus self monitored training programmes in patients with chronic obstructive pulmonary disease. Eur Respir J 2000; 15: 517–525.