OBJECTIVE: To associate the short-term effects of the Handmaster® orthosis on disabling symptoms of the affected upper extremity with long-term Handmaster® orthosis use after stroke.
DESIGN: Historic cohort study.
Patients: Patients with chronic stroke.
METHODS: The Modified Ashworth Scale (0–5) for wrist (primary outcome) and elbow flexor hypertonia, visual analogue scale (0–10) for pain, oedema score (0–3), and passive range of wrist flexion and extension (pROM, degrees) were assessed prior to Handmaster® orthosis prescription (T0), after 6 weeks try-out (T1) and a subsequent 4 weeks withhold period (T2). Long-term use was evaluated using a questionnaire. Non-parametric analyses and predictive values were used for statistical analyses.
RESULTS: Of the 110 included patients 78.2% were long-term Handmaster® orthosis users. Long-term users showed significant short-term (T0–T1) improvements on all impairment scores and a significant relapse of wrist and elbow Modified Ashworth Scale (T1–T2). Non-users showed significant short-term effects on elbow Modified Ashworth Scale and visual analogue scale only. Positive predictive values of short-term effects for long-term use varied between 75% and 100%, with 85% (95% confidence interval (CI) 0.72–0.93) for wrist Modified Ashworth Scale. Negative predictive values were low (11–27%).
CONCLUSION: Short-term Handmaster® orthosis effects were generally beneficial for hypertonia, pain, oedema, and pROM, especially in long-term users. Short-term beneficial effects were highly predictive for long-term use, but not for non-use.
Key words: therapeutic electrical stimulation, long-term use, hypertonia, pain, stroke, cerebrovascular accident, utilization, upper extremity, spastic hemiplegia.
J Rehabil Med 2009; 41: 157–161
*This paper was presented as an abstract on the 16th European Congress on Physical and Rehabilitation Medicine, 4–7 June 2008 in Brugge, Belguim.
Correspondence address: J.-W. G. Meijer, Department of Rehabilitation Medicine, HP nr F00.810, University Medical Centre Utrecht, PO Box 85500, NL-3508 GA Utrecht, The Netherlands. E-mail: j.w.g.meijer@umcutrecht.nl
Submitted March 9, 2008; accepted September 24, 2008
INTRODUCTION
Neuromuscular electrical stimulation (NMES) of the upper limb has received considerable attention recently as a therapeutic modality in post-stroke rehabilitation (1, 2). Several commercially available NMES devices have been introduced, of which the Handmaster® orthosis (HMO) (NESS, Ra’anana, Israel) is probably one of the most widespread. This hybrid orthosis with built-in electrodes has been developed specifically to stimulate the extensor and flexor muscles of the paretic forearm as well as the thenar muscles of the hand in patients with central neurological disorders. Its primary application has been focused on patients who have sustained a stroke.
Several studies in this patient population have reported positive outcomes of NMES on muscle hypertonia, while improvements have also been reported for pain, oedema, and passive range of motion (pROM) in patients with severe paresis or paralysis of the affected upper extremity (3–7). In a systematic review, De Kroon and colleagues (2) concluded that NMES may have a beneficial effect on motor control and strength of the affected upper limb, although mainly in patients with mild residual motor function. Sheffler & Chae (1) arrive at a similar conclusion in their review, although the effect of NMES on arm-hand abilities and dexterity remains ambiguous. As for the reduction in disabling symptoms in more severely affected patients, published studies are relatively scarce and are based on small and heterogeneous samples of stroke patients (3–7). Yet, in clinical practice, long-term NMES is applied particularly in more severely affected patients to achieve symptom reduction, although little is known about which patients can be expected to become long-term users.
In the Netherlands, national guidelines have been developed by the Dutch Working Group of Rehabilitation Physicians for Stroke to assess the short-term effects of NMES on various disabling symptoms of the affected upper extremity in order to better support the clinical decision-making process for long-term prescription of this device in chronic stroke patients (i.e. at least 6 months post-onset), in which no NMES had been used in the (post-) acute phase. The development of these guidelines was requested by healthcare insurers, when the HMO was introduced on the Dutch market as the first readily applicable NMES device for home-based treatment, in order to obtain reimbursement on a case by case basis. The guidelines indicate that, during a try-out period of 6 weeks, individual responses should be monitored with regard to hypertonia, pain, oedema and pROM. After a withhold period of another 4 weeks, these short-term effects should again be evaluated and a definitive decision with regard to long-term prescription is made based on a positive response during the try-out period and a possible relapse in the withhold period. No specific follow-up instructions are given. Although these guidelines have been used for several years in the Netherlands, a formal evaluation has not yet been made. The goal of this study was therefore to evaluate the short-term effects of the HMO on disabling symptoms of the affected upper extremity in patients after severe stroke, and to associate these findings with the actual long-term use of this device in these patients. Insight into this association may improve the efficiency and cost-effectiveness of chronic NMES application for the upper extremity after stroke.
METHODS
Procedure
This historical cohort study made use of a database that emerged from the nationwide application of guidelines for the long-term prescription of the HMO in patients with chronic stroke, developed by the Dutch Working Group of Rehabilitation Physicians for Stroke in 2001. These guidelines comprise a fixed protocol for the assessment of muscle hypertonia, pain, oedema and pROM of the affected upper extremity before (T0) and immediately after a 6-week try-out period (T1), and subsequently after a 4-week withhold period (T2). In the first week of the try-out period, the size of the HMO and its electrode positions were individually adjusted as well as the intensity, duration and frequency of the electrical stimuli to obtain optimal alternating responses of the extensor and flexor muscles of the forearm. These adjustments were made by a local physical or occupational therapist, who had been trained specifically for this purpose. After the first week, the frequency and duration of the stimulation were gradually increased up to 2–3 times, 30–45 min per day, 7 days per week, depending on individual goals, tolerance, and compliance. At T1, the device was returned to the therapist until T2.
The applied HMO is a hybrid wrist-hand orthosis with integrated surface electrodes for the extensor and flexor muscles of the forearm and for the thenar muscles of the hand. It is attached to a control unit through a cable. Individual stimulation parameters (duration, frequency and type of pulses) are set and stored in the control unit, but the patients can turn the device on and off themselves, and increase the intensity of stimulation to a fixed maximum, when necessary. Three pre-programmed exercise modes and 3 functional modes provide stimulation to the targeted muscles: extensor digitorum communis, extensor pollicis brevis, flexor digitorum superficialis, flexor pollicis longus and thenar muscles (in the present study, only the exercise modes were used). The spiral design allows for wrist stabilization and maintains the wrist in a functional position of 10–20° dorsiflexion. Due to its design, patients are able to put on and take off the device themselves, maintaining reliable and effective electrode placement.
At T0, T1, and T2, each of the following impairments were evaluated by the local physical or occupational therapist:
• Muscle hypertonia was evaluated with the Modified Ashworth scale (MAS) (8) for both the affected elbow and wrist flexor muscles. With the patient in a sitting position, the therapist moved the elbow or wrist from full flexion to extension at a high velocity and observed the resistance to passive movement, which was classified from 0 (no resistance) to 5 (no movement possible). Despite debate in the literature, the MAS is a reliable tool for assessment of post-stroke hypertonia when raters follow strict protocols and are well instructed (9). Yet, the MAS was not regarded sufficiently reliable to assess finger hypertonia
• Pain in the forearm and/or hand was evaluated with an 11-point (vertical) visual analogue scale (VAS). Although a horizontal VAS is more common in general pain assessment (10), the vertical alternative is more appropriate for patients after stroke to prevent bias due to visuospatial hemi-neglect (e.g. 11). A score of 0 indicated “no pain” and a score of 10 indicated “intractable pain”
• Oedema of the hand was scored by clinical judgement on a 4-point scale (0: absent, 1: minimal, 2: moderate, 3: severe). Because there are currently no validated clinical oedema scores available, this ordinal scale, which is simple and straightforward, was used.
• pROM of the wrist was assessed in 2 directions by slowly moving the affected hand from maximal flexion to maximal extension using goniometry. pROM in both directions was assessed with an accuracy of 5°.
Participants
Each patient who had been prescribed the HMO between 1 July 2001 and 1 January 2003 according to the above-mentioned guidelines in 31 Dutch rehabilitation institutes was eligible for inclusion in the cohort. In early 2005, all these institutes were asked for their co-operation in this study. In the case of a positive answer, the patients who had received their HMO through this particular institute were approached by their treating physician and invited to participate. This procedure was approved by the local medical ethics committee and the patients who agreed to participate gave their written informed consent. For each patient, social demographics and the impairment scores at T0, T1, and T2 were collected. In addition, all patients were sent a questionnaire evaluating the actual use of the HMO (see Appendix 1), documenting frequency and duration of use or reasons for non-use. All questionnaires were filled in anonymously and returned in a stamped addressed envelope. Because it appeared that nearly all patients had baseline hypertonia of wrist flexor muscles, it was decided that the wrist flexor MAS was used as the primary outcome with regard to the short-term effects and the main determinant for predicting long-term use. As a consequence, patients with a MAS of 0 were excluded from the cohort in second instance. The data obtained with the questionnaire were used to categorize patients into long-term “users” or “non-users”. Users were defined as subjects who used the HMO on a daily basis for at least 15 min at the time of evaluation, whereas others were classified as non-users.
Statistical analysis
Non-parametric analyses were applied to evaluate all impairment scores because of their ordinal nature (hypertonia, pain, oedema) or non-normal distribution (pROM). First, the short-term effects of the HMO were evaluated using Friedman tests including data from all included subjects at T0, T1, and T2. Post-hoc Wilcoxon tests were applied to explore whether any significant changes in primary (hypertonia) and secondary (oedema, pain, and pROM) outcome measures occurred during the try-out and/or withhold periods. The same procedure was then followed with a split database for long-term users and non-users.
Secondly, it was investigated whether short-term clinical effects, i.e. improvements in hypertonia, pain, oedema, and pROM, were associated with long-term use by calculating positive and negative predictive values, including corresponding confidence intervals. To this end, a clinical relevant effect was defined as a reduction of at least 1 point for the MAS, the VAS pain score, and the oedema score, and an improvement of at least 15 degrees for the pROM. All statistics were computed with SPSS 11.5 and alpha was set at 0.05 for statistical significance.
RESULTS
Patient characteristics and long-term use
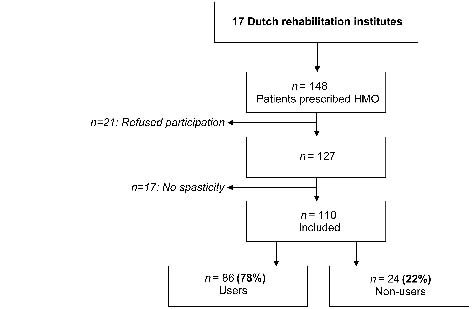
The patient inclusion and categorization process is shown in Fig. 1.
Fig. 1. Flow chart of patient inclusion and categorization process. HMO: Handmaster® orthosis.
Of the 31 rehabilitation institutes, 17 were willing to participate in this study. In these 17 institutes, 148 patients had been prescribed the HMO during the assigned 18 month period, of which 127 (86%) agreed to participate and returned the informed consent. Seventeen patients appeared to have no wrist flexor hypertonia, so that 110 patients could eventually be included. These patients were on average 6.5 years (standard deviation (SD) 4.5, range 2.8–25.0) after stroke and 2.7 years (SD 0.6, range 1.2–4.0) post HMO prescription (see Table I for patient demograhics). Eighty-six patients (78.2 %) were defined as users. The HMO was used once a day by 37 patients (41.2%), twice a day by 42 patients (49.4%), and 3 times a day by 6 patients (7.1%). The mean duration of use was 39 min (SD 10, range 15–60 min). All 24 non-users (21.8%) had completely stopped using the HMO. The mean duration of HMO treatment in the users group was 2.7 years (SD 0.6), whereas the non-users had stopped HMO treatment on average 0.8 years (SD 0.7) after prescription. Reasons for non-use as reported by these patients (available for 18 of the 24 patients) were insufficient benefit (44%), side-effects (17%), epilepsy (11%), no reimbursement (11%), surgery of the arm (11%), and lack of time (6%). Users and non-users were comparable with regard to gender, age, hemisphere of stroke, time post-onset, as well as MAS, VAS pain, oedema, and pROM at T0.
| Table I. Patient characteristics before the start of the study (n = 110) |
| | Entire group | Users | Non-users |
| Gender, men/women, % | 51/49 | 51/49 | 50/50 |
| Age, years, mean (SD) | 57.7 (11.8) | 59.5 (11.7) | 56.3 (12.1) |
| Location stroke, left/right hemisphere, % | 57/43 | 59/41 | 50/50 |
| SD: standard deviation. |
Short-term effects
For all patients together, the MAS for wrist flexors (χ2 = 43.8, p < 0.01), the MAS for elbow flexors (χ2 = 39.7, p < 0.01), the VAS pain score (χ2 = 22.6, p < 0.01), the oedema score (χ2 = 13.7, p < 0.01), and the passive range of wrist flexion (χ2 = 25.3, p < 0.01) and extension (χ2 = 18.9, p < 0.01) significantly changed from T0 to T2. Post-hoc analysis revealed that for both the primary and secondary outcomes an improvement was observed between T0 and T1, but not between T1 and T2 (see Table II).
When differentiating between users and non-users, significant short-term effects were more present in users compared with non-users. The MAS for wrist flexors (χ2 = 42.1, p < 0.01), the MAS for elbow flexors (χ2 = 32.6, p < 0.01), the VAS pain score (χ2 = 15.8, p < 0.01), the oedema score (χ2 = 16.1, p < 0.01), and the passive range of wrist flexion (χ2 = 23.3, p < 0.01) and extension (χ2 = 22.5, p < 0.01) all improved in the user group between T0 and T2. Post-hoc analysis indicated that for the users, the MAS scores for the wrist and elbow flexors were reduced between T0 and T1 with a significant relapse between T1 and T2. All other impairment scores showed a significant change only between T0 and T1. As for the non-users, only the MAS for the elbow flexors (χ2 = 9.7, p < 0.01) and the VAS pain score (χ2 = 7.8, p = 0.02) improved. Post-hoc analysis showed that these changes occurred between T0 and T1 (see Table II).
| Table II. Mean scores (SD) of the impairments |
| | Entire group | Users | Non-users |
| T0 | T1 | T2 | T0 | T1 | T2 | T0 | T1 | T2 |
| MAS wrist, 0–5 | 2.4 (1.1) | 1.8 (1.1)** | 2.0 (1.2)* | 2.4 (1.1) | 1.8 (1.1)** | 2.0 (1.2)* | 2.0 (1.0) | 1.8 (1.1) | 1.9 (1.1) |
| MAS elbow, 0–5 | 2.3 (1.1) | 1.7 (1.0)** | 1.8 (1.1) | 2.2 (1.1) | 1.6 (1.0)** | 1.9 (1.1)* | 2.5 (1.1) | 1.9 (1.0)* | 1.8 (1.1) |
| Oedema, 0–3 | 0.4 (0.7) | 0.3 (0.5)** | 0.3 (0.5) | 0.5 (0.7) | 0.3 (0.5)** | 0.3 (0.5) | 0.3 (0.5) | 0.3 (0.5) | 0.4 (0.5) |
| VAS, 0–10 | 1.8 (2.5) | 0.9 (1.7)** | 1.5 (2.4)* | 1.8 (2.5) | 1.0 (1.7)** | 1.4 (2.4) | 1.9 (2.6) | 0.8 (1.7)* | 1.6 (2.6) |
| Wrist flexion, ° | 80.6 (16.8) | 85.8 (14.2)** | 83.2 (12.7) | 79.8 (17.5) | 85.1 (15.2)** | 81.8 (13.1) | 83.5 (14.2) | 88.2 (9.9) | 87.1 (10.8) |
| Wrist extension, ° | 62.8 (22.1) | 69.7 (20.0)** | 67.9 (21.6) | 61.5 (20.4) | 69.9 (17.1)** | 69.4 (17.9) | 67.3 (26.9) | 69.1 (28.4) | 63.4 (30.3) |
| *Compared with T0, p < 0.01, **Compared with T0, p < 0.001. T0: before study; T1: immediately after a 6-week try-out period; T2: subsequently after a 4-week withhold period; MAS: Modified Ashworth scale; VAS: visual analogue scale; SD: standard deviation. |
Associations between long-term use and short-term effects
The positive predictive value of a short-term effect (between T0 and T1) of at least 1 point on the wrist flexor MAS with regard to long-term use was 85% (95% confidence interval (CI) 0.72–0.93).
As for the secondary outcomes, a decrease in oedema score and VAS pain score of at least 1 point showed positive predictive values of 100% (95% CI 0.40–1.0) and 80% (95% CI 0.62–0.91), respectively, and an increase in passive wrist extension and flexion of at least 15° showed positive predictive values of 86% (95% CI 0.72–0.94) and 75% (0.43–0.93), respectively. Negative predictive values, based on the absence of symptom improvement between T0 and T1, were generally low (between 11% and 27%).
DISCUSSION
This study evaluated the short-term effects of the HMO on the disabling symptoms of the affected upper extremity in patients with chronic stroke and associated these effects with long-term use of the HMO in an historic cohort of 110 subjects with initial wrist flexor hypertonia. In all patients, HMO prescription was based on the short-term effects observed during a 6-week try-out period and a subsequent 4-week withhold period. In those patients (78%) who continued using the device in the long term, the expected pattern of a decrease in muscle hypertonia during the try-out phase and a relapse of hypertonia during the withhold phase was found for both the wrist and elbow flexors. In the non-users (22%), only a reduction in elbow flexor hypertonia was found during the try-out phase. As for the secondary outcomes, the long-term users showed an improvement in upper extremity pain, hand oedema and wrist passive range of motion, whereas the non-users only showed a reduction of pain. Apparently, the applied protocol was able to predict long-term use based on a short-term reduction in the various symptoms, with positive predictive values varying between 75% and 100%, but it could not predict non-use based on absence of symptom reduction. The criterion for long-term HMO use was consciously set at 15 min per day, since experience has learned that many patients tend to seek the shortest duration of stimulation that is still effective to control their symptoms. Yet, when the lower limit would have been set at, for example, 30 min per day, 80 (72.7%) of the included patients would still have been classified as long-term users.
The results of the present study support the literature indicating the potentially beneficial effect of NMES on both muscle hypertonia, pain, oedema, and pROM in severely affected stroke patients (3–7). The added value of the current study is the inclusion of a large number of patients, the use of a predefined prescription protocol, and the observed strong association of short-term beneficial effects with a high percentage of long-term use. The association between long-term use and short-term effects suggests that patients benefited from the HMO in the long-term as well. The observed 78% long-term use has not been reported before for any NMES device. Besides to a standardized selection of patients with measurable short-term effects, this result can probably be attributed to the unique design of the HMO that allows independent putting on and taking off the device and reproducible electrode placement even by severe stroke patients. No patient was specifically followed up to promote long-term use.
How NMES contributes to symptom reduction after severe stroke is not yet fully understood. On a peripheral and spinal level, reciprocal and recurrent inhibition may reduce involuntary stimulation of spastic muscles (12, 13). Indirectly, pain and pROM may be improved when muscles become more relaxed, whereas oedema may be reduced by deep venous compression due to the repetitive muscle contractions induced by NMES. On a supraspinal level, NMES may induce neuroplasticity and modulate pain perception as well. Indeed, changes in (sensory) cortical activation as measured by functional magnetic resonance imaging (fMRI) have been shown due to NMES application to the extensors muscles of the hemiparetic forearm in patients with stroke (14). Such results suggest that the beneficial effects of NMES may be even more pronounced when applied in the subacute rather than the chronic phase of stroke (5).
According to clinical expectation, short-term effects were strongly associated with long-term HMO use. However, somewhat counter-intuitively, many patients without short-term beneficial effects turned out to be long-term users as well. Several explanations can be given for this result. First, the applied outcome measures may not have been sufficiently sensitive to detect subclinical improvements (of the assessed or of a different kind) that may still be relevant for the subjective evaluation by some patients. These patients (and their therapists) probably decided to nevertheless continue HMO use and await stronger effects. In the same line of reasoning, measurable beneficial effects might have occurred over a longer period than 6 weeks of stimulation. Secondly, the low negative predictive values for all outcome measures are probably confounded by the fact that most patients and therapists valued the improvement (and possible relapse) on one particular symptom important enough to continue HMO use as long as its use did not worsen other symptoms. Thus, lack of improvement on one particular symptom will not predict non-use, as long as improvement on another symptom is strongly associated with long-term use.
Limitations
The outcome measures applied in this study may be criticized for their clinimetric properties. In particular the sensitivity and validity of the MAS and the oedema scale may be questioned. As for the MAS, it is well known that it cannot discriminate between hypertonia induced by neural activation (“spasticity”) and increased resistance to passive movement due to muscle stiffness and contracture. Hence, it might have been preferable when a velocity-dependent measure of hypertonia would have been used, since NMES may have an effect on spasticity rather than on stiffness and contracture. Still, the MAS is widely applied in clinical practice and its clinimetric properties for the upper extremity, the elbow in particular, have been shown to be quite satisfactory as long as assessors adhere to a strict protocol and are well instructed (9). With regard to oedema, there is currently no well-accepted and validated alternative. The retrospective design of this study may have affected the information (by recollection bias) about when non-users had stopped using the HMO. A prospective cohort study would be more appropriate to predict and monitor actual use, but would take many more years to conduct. In addition, the data obtained with the questionnaires might have been biased with regard to both frequency and duration of HMO use due to social desirability. However, since all participants were informed that their responses would be handled anonymously, this is not very likely. The percentages of long-term users and non-users might have been different in the patients who were approached, but who were not willing to participate. For instance, these patients might be largely non-users who were dissatisfied or disappointed by the effects of the HMO. Because this study had only 14% “non-responders”, the effect of this possibility is probably limited. Lastly, this study may have included the most motivated patients as it was conducted during the introduction period of the HMO in the Netherlands. This notion may also explain the rather low prescription rate. Hence, although this was a nationwide study, the results cannot be readily generalized to other populations.
In conclusion, significant short-term effects of the HMO are present in chronic stroke patients with regard to various disabling symptoms of their affected upper extremity. When based on an initial reduction of hypertonia, approximately 78% of the patients will continue using the HMO for more than 2 years. Although short-term beneficial effects are strongly associated with long-term use, many patients without such short-term effects may become long-term users as well, which suggests the possibility of subclinical beneficial effects that remain undetected during a 6-week try-out period. Although the results were obtained using a well thought-out national guideline, extended use of this precise guideline is not recommended. Instead, the guideline should be improved by using more sensitive outcome measures, including some at the level of activities and participation, for example by using the goal attainment scale.
ACKNOWLEDGEMENTS
This study was performed on request of the national Health Care Insurance Board (College Voor Zorgverzekeringen (CVZ)), an independent advisory board for health policymakers and insurance companies in the Netherlands.
We thank the participating members of the Dutch Working Group of Rehabilitation Physicians for Stroke (WCN) of the Dutch Society for Physical Medicine and Rehabilitation (VRA).
REFERENCES
1. Sheffler LR, Chae J. Neuromuscular electrical stimulation in neurorehabilitation. Muscle Nerve 2007; 35: 562–590.
2. de Kroon JR, van der Lee JH, IJzerman MJ, Lankhorst GJ. Therapeutic electrical stimulation to improve motor control and functional abilities of the upper extremity after stroke: a systematic review. Clin Rehabil 2002; 16: 350–360.
3. Weingarden HP, Zeilig G, Heruti R, Shemesh Y, Ohry A, Dar A, et al. Hybrid functional electrical stimulation orthosis system for the upper limb: effects on spasticity in chronic stable hemiplegia. Am J Phys Med Rehabil 1998; 77: 276–281.
4. Hendricks HT, IJzerman MJ, de Kroon JR, in ‘t Groen FA, Zilvold G. Functional electrical stimulation by means of the “Ness Handmaster Orthosis” in chronic stroke patients: an exploratory study. Clin Rehabil 2001; 15: 217–220.
5. Ring H, Rosenthal N. Controlled study of neuroprosthetic functional electrical stimulation in sub-acute post-stroke rehabilitation. J Rehabil Med 2005; 37: 32–36.
6. Santos M, Zahner LH, McKiernan BJ, Mahnken JD, Quaney B. Neuromuscular electrical stimulation improves severe hand dysfunction for individuals with chronic stroke: a pilot study. J Neurol Phys Ther 2006; 30: 175–183.
7. Sullivan JE, Hedman LD. Effects of home-based sensory and motor amplitude electrical stimulation on arm dysfunction in chronic stroke. Clin Rehabil 2007; 21: 142–150.
8. Bohannon RW, Smith MB. Interrater reliability of a modified Ashworth scale of muscle spasticity. Phys Ther 1987; 67: 206–207.
9. Gregson JM, Leathley M, Moore AP, Sharma AK, Smith TL, Watkins CL. Reliability of the Tone Assessment Scale and the modified Ashworth scale as clinical tools for assessing poststroke spasticity. Arch Phys Med Rehabil 1999; 80: 1013–1016.
10. Gift A. Visual analogue scales: measurement of subjective phenomena. Nursing Res 1984; 38: 286–288.
11. Pomeroy VM, Frames C, Faragher EB, Hesketh A, Hill E, Watson P, et al. Reliability of a measure of post-stroke shoulder pain in patients with and without aphasia and/or unilateral spatial neglect. Clin Rehabil 2000; 14: 584–591.
12. Eisen A. Electromyography in disorders of muscle tone. Can J Neurol Sci 1987; 14: 501–505.
13. Sehgal N, McGuire JR. Beyond Ashworth. Electrophysiologic quantification of spasticity. Phys Med Rehabil Clin N Am 1998; 9: 949–979.
14. Kimberley TJ, Lewis SM, Auerbach EJ, Dorsey LL, Lojovich JM, Carey JR. Electrical stimulation driving functional improvements and cortical changes in subjects with stroke. Exp Brain Res 2004; 154: 450–460.
| Appendix I. Patient questionnaire. |
| Do you still use the Handmaster? |
| • Yes, I still use the Handmaster. |
| How often a day (on average) are you using the Handmaster? …. a day. |
| How long (on average) are you using the Handmaster each time? …. minutes. |
| • No, I do not use the Handmaster any longer. |
| Why did you stop using the Handmaster? |