BACKGROUND: Patients with fibromyalgia have a high risk of temporary and permanent work disability. Little is known about the effects of fibromyalgia rehabilitation on work disability.
OBJECTIVE: To determine whether a specific fibromyalgia rehabilitation programme is superior to a non-specific musculoskeletal rehabilitation of patients with fibromyalgia in terms of work disability.
METHODS: A prospective observational study of 215 local government employees with a 6-year post-intervention follow-up to monitor the occurrence of long sick-leave and disability pensions among the participants of two different fibromyalgia rehabilitation programmes.
RESULTS: Specific fibromyalgia rehabilitation was not superior to a non-specific musculoskeletal rehabilitation, with the corresponding hazard ratios (95% confidence intervals) after adjustments being 1.02 (0.75–1.40) for long sick-leave, 1.18 (0.75–1.87) for very long sick-leave, and 1.07 (0.63–1.83) for disability pension.
CONCLUSION: The results suggest that in reducing work disability among patients with fibromyalgia a specific multidisciplinary fibromyalgia rehabilitation programme practised in Finland provides no benefit compared with non-specific multidisciplinary musculoskeletal rehabilitation. Further research is needed to develop an optimal programme (or several different programmes) to control the burden of work disability related to fibromyalgia.
Key words: fibromyalgia, rehabilitation, sick-leave, disability pension.
J Rehabil Med 2009; 41: 66–72
Correspondence address: Heikki Suoyrjö, Department of Rehabilitation Medicine, Hospital District of South Ostrobotnia, Hanneksenrinne 7, FI-60220 Seinäjoki, Finland. E-mail: hsuoyr@utu.fi
Submitted January 18, 2008; accepted July 9, 2008
INTRODUCTION
Fibromyalgia syndrome (FM) is a disorder characterized by chronic widespread musculoskeletal pain and the presence of at least 11 out of 18 specific muscle-tendon tender sites (1). Fatigue and disturbed sleep are commonly associated with this pain syndrome. The precise aetiology of FM is unknown, but peripheral or central hyperexcitability and sensitization in the nervous system have been hypothesized (2, 3). The estimated prevalence of FM in the general population is 2–5%, and females are over-represented compared with men, with ratios varying between 8:1 and 20:1 (4–6). FM is presented as a chronic condition where remissions are rare and the prevalence of the disorder increases with age (7). Since the symptoms often begin in early adulthood, FM causes essential losses in working capacity (8). In a recent population-based cross-sectional study, 15.9% of the respondents with self-reported FM showed permanent disability to work (9). In another recent occupational cohort study, FM was associated with a substantial burden of recorded medically certified sickness absence (10). A study based on a health-insurance database in the USA indicated that patients with FM utilize pain-related pharmacotherapy almost twice as much as age- and gender-matched subjects without FM (11).
Education and physical exercise have been proposed as the cornerstones in the non-pharmacological treatment of FM (12, 13). A multidisciplinary approach combining patient education, physical exercise, cognitive behavioural therapy, relaxation training and pharmacotherapy has been suggested to be effective in reducing the symptoms of FM (14, 15). However, a recent review on the non-pharmacological treatment of FM showed that the effects of interventions are limited and positive outcomes frequently disappear in the long run (16). Existing studies have reported diverging results. A major limitation is the relatively short duration of the follow-up periods after the interventions. To our knowledge, there is only one study with a follow-up of 4 years (17). Thus, there is a lack of knowledge on what type of rehabilitation intervention is the most effective in reducing work disability among patients with FM.
We were interested in comparing the effects of 2 multidisciplinary rehabilitation programmes on work disability among patients with FM. We conducted an observational study with a follow-up period of 6 years among local government employees who had been diagnosed with FM and who participated in either of the two rehabilitation programmes: a specific multidisciplinary inpatient FM rehabilitation course, designed according to the recommendations presented in many reviews, or a non-specific inpatient rehabilitation course, designed for subjects with musculoskeletal disorders and without any FM-specific content. Both rehabilitation interventions were provided by the Social Insurance Institution (SII) of Finland. We hypothesized that participation in the rehabilitation course designed specifically for patients with FM would be more effective in reducing work disability, as indicated by the risk of long-term sickness absence and disability pension, than participation in a non-specific musculoskeletal rehabilitation programme.
METHODS
Study population
This study is a part of the ongoing 10-town study examining work-related determinants of health among all full-time local government employees working in 10 Finnish towns (18). From the employers’ records, we identified the eligible population, i.e. 67,106 local government employees who had been employed for at least 10 months in one year between 1994 and 2002. The data on participation and primary indication for rehabilitation (diagnoses) were retrieved from the SII register by using the employees’ personal identification codes. From the eligible population, a total of 7440 employees had participated in some type of rehabilitation provided by the SII between 1994 and 2002 (19). Of them, 124 employees participated in a specific FM inpatient rehabilitation programme and 94 employees with FM diagnosis as the primary indication for rehabilitation in a non-specific inpatient musculoskeletal rehabilitation course or individual inpatient rehabilitation. The mean follow-up period was 5.5 (standard deviation (SD 0.9)) years for the participants of the FM courses and 5.4 (1.1) years for the participants of the non-specific musculoskeletal rehabilitation.
The ethics committee of the Finnish Institute of Occupational Health approved the study.
Two rehabilitation programmes for patients with FM
In Finland, the SII is the provider of certain disease- or disorder-specific rehabilitation interventions that are discretionary for the SII and based on the annual budget confirmed by the Finnish Parliament (19). The interventions are often called “courses” because they take place at rehabilitation centres on an inpatient basis, in groups of 8–10 people, and are divided to 2 or 3 periods. The purpose of rehabilitation is to provide the rehabilitees with means for active self-care and to maintain or restore their work ability. A common goal is also to reveal symptoms of musculoskeletal origin and to instruct and motivate individuals in physical exercise.
The participants of the specific FM courses were selected by the local SII offices, and to verify the diagnosis, a statement by the treating physician or specialist was warranted. The courses were implemented on an inpatient basis and divided into 2 separate periods within 6 months, totalling 15 days. The programme of the FM courses was multidisciplinary in character, with contributions from a physician, a psychologist, a physiotherapist, an occupational therapist, an exercise adviser, a nurse, and a social worker. The aim of the FM courses was, in compliance with the SII guidelines, to “promote an active rehabilitation process by providing information about the disorder, encouraging rehabilitees in coping with symptoms and helping rehabilitees to find, develop and utilize different means of self-care in order to enhance self-efficacy”. For the content, the FM course programme followed the recommendations described by many authors (12–15). As it is recommended that the exercise has to be individually designed, at the beginning of every course the aerobic capacity of all participants was measured and the level of exercise matched up accordingly. Also, in line with the recent recommendations for treatment of FM that cognitive behavioural approach should be included; the practical sessions on coping in daily life were based on such an approach.
The participants of non-specific musculoskeletal rehabilitation were offered one of the 3 possible rehabilitation interventions provided by the SII: a course for patients with symptoms related to several parts of the musculoskeletal system (n = 18), a course for elderly employees with notable functioning disability (n = 40), or individual medical rehabilitation (n = 36). The last-mentioned was possible when, on medical grounds, individual rehabilitation was preferable to group-based courses (19). All of these non-specific musculoskeletal rehabilitation interventions lasted longer than FM courses and the time-spans of the whole rehabilitation process were also longer. Courses for patients with multifocal musculoskeletal symptoms and individual rehabilitation periods lasted a total of 17 days in 2 periods within 6 months. The courses for elderly employees with notable functional disability were carried out in 4 periods totalling 33 days within 18 months. The selection to non-specific musculoskeletal courses took place at the SII offices similarly to FM courses, and was likewise based on the statements from the treating physicians with verified diagnosis of FM. While the number of rehabilitation centres offering FM courses was limited, employees with FM diagnosis and a need for non-pharmacological treatment were offered participation to non-specific musculoskeletal rehabilitation.
Both types of intervention were based on a multidisciplinary programme, but the emphases diverged. The FM courses focused more on education, with a low level of physical strenuousness. In non-specific musculoskeletal rehabilitation, on the other hand, the proportion of education was smaller, and the emphasis was on aerobic exercise and muscle strength. The participants of non-specific musculoskeletal rehabilitation were not given any information about FM-specific issues and they did not have educational small-group discussions or practical sessions on finding suitable coping strategies and integrating theoretical knowledge to practical measures. Instead, they were instructed and motivated to gradually increase strenuous aerobic exercise and to apply active self-management for musculoskeletal symptoms. The main similarities and differences between the programmes of the specific FM courses and non-specific musculoskeletal rehabilitation are shown in Table I.
| Table I. Main similarities and differences between the programmes of the specific FM courses and non-specific rehabilitation for musculoskeletal disorders, both provided by the Social Insurance Institution of Finland |
| | Specific FM course | Non-specific rehabilitation for musculoskeletal disorders |
| Duration Time-span of the process | 15 days 6 months | 17–33 days 6–18 months |
| Accommodation | Inpatient | Inpatient |
| Multidisciplinary approach Testing of aerobic capacity | Yes Yes | Yes Yes |
| Exercise, in groups under instruction |
| Aerobic endurance | Yes | Yes |
| Muscular strength | No | Yes |
| Swimming-pool exercise | Yes | Yes |
| Lectures about health-related issues |
| Healthy lifestyle | Yes | Yes |
| Medical and psychological information about FM | Yes | No |
| Practical sessions on coping in daily life | Yes | No |
| FM: fibromyalgia syndrome. |
Assessment of baseline health status
Details concerning the participants’ age, gender and occupational status (manual, lower-grade non-manual, higher grade non-manual) were obtained from the employers’ records.
To assess any prevalent severe and/or chronic diseases at baseline, we obtained, from the SII prescription register, data on special medication reimbursements paid out during the intervention year. In Finland, the national sickness insurance scheme provides reimbursement up to 72–100% of the costs of special medication for many chronic and severe diseases, such as hypertension, asthma, coronary heart disease, cancer, diabetes and epilepsy. As regards psychiatric diseases, people with psychotic disorders are entitled to special medication reimbursement.
To measure the consumption of analgesics and antidepressants, we used data obtained from the prescription register of the SII. The national sickness insurance scheme covers the entire population, and provides reimbursement for all outpatient prescriptions classified according to the World Health Organization Anatomical Therapeutic Chemical (ATC) classification code (20). The defined daily dose (DDD) is the assumed average maintenance dose per day for a drug used for its main indication in adults. To obtain and accurate estimate of annual analgesic and antidepressant consumption, we used the SII prescription register and calculated DDDs for the purchases of prescribed analgesics (ATC code N02 and M01A) and antidepressants (ATC code N06A) for the participants of each intervention group in the rehabilitation year and for all the employees in the same organizations in the year 1999. The annual purchases of these drugs were divided into 3 categories: none, < 100 DDDs, and ≥ 100 DDDs.
Data on annual sick-leave days were collected from the employers’ records (by using the personal identification codes) for each rehabilitee in the rehabilitation year (between 1994 and 2002) and for all employees in the cohort (n = 45, 837) in 1999. The employers participating in the 10-Town study are obliged to record each period of sick-leave for every employee, including the dates when each period of sick-leave starts and ends. In accordance with the regulations, each sick-leave certificate must be forwarded for recording.
Assessment of post-intervention sick-leave and disability pension
To measure the occurrence of sick-leave after the intervention, we obtained data from the national sickness insurance register of the SII. The national sickness insurance scheme provides compensation for all sick-leave longer than 10 days. The compensation is 60% of the salary and it is paid to an employee (or to the employer in case an employee is paid salary during the sick-leave) for one year at maximum. From the SII register, we retrieved the start and end dates of all those sick-leaves entitling to the compensation and, separately, of very long sick-leave (≥ 90 days) between 1 January 1994 and 31 December 2006. Long-standing illnesses, such as musculoskeletal disorders, have been shown to be associated with sickness absences of longer duration (21, 22).
Data on disability pensions granted after the intervention (including full and partial disability pension, individual early retirement pension, fixed term disability pension, and pension because of injuries) were collected from the national pensions register maintained by the Finnish Centre of Pensions. This register provides virtually complete information on retirement at population level. The dates and causes of disability pensions granted for the subjects of this study between 1 January 1994 and 31 December 2006 were obtained.
Statistical analysis
Baseline differences between the groups in demographics, special medication reimbursements, and the purchases of analgesics and antidepressants were analysed by χ2 test. We used the Cox proportional hazard models to study the risk of medically certified sickness absence and disability retirement among the patients with FM participating in specific FM courses, compared with those participating in non-specific musculoskeletal rehabilitation, and calculated the corresponding hazard ratios (HR) with 95% confidence intervals (95% CI). The outcome measures were the first long (≥ 11 days) sickness leave, the first very long (≥ 90 days) sickness leave, and the incidence of disability pension. The HR were adjusted for age, gender, occupational status, and entitlement to any special medication reimbursement. The follow-up period was calculated starting from 1 January of the year following the intervention. The employees were censored on the date of the first long sick-leave, on the date of the first very long sick-leave, or on the date they were granted a disability pension, reached the age of 63 years (official age of retirement in Finland), or died, or on 31 December of the 6th year of follow-up, or on 31 December in the year 2006, whichever came first.
The time-dependent interaction term between the intervention and the follow-up period was non-significant for the first long sick-leave (p = 0.826), the first very long sick-leave (p = 0.295), and disability pension (p = 0.356), thus confirming that the proportional hazard assumption was justified. We then calculated Kaplan-Meier hazard curves to illustrate the associations of medically certified sickness absences and disability pensions for the rehabilitees participating in each of the rehabilitation programmes.
All the analyses were performed with SAS 9.1.3 statistical software (SAS Institute, Inc., Cary, North Carolina, USA).
RESULTS
Baseline health indicators
The comparison of baseline health indicators of the participants in the specific FM courses (n = 124) and non-specific musculoskeletal rehabilitation (n = 94) showed that there were no significant differences between the groups in terms of gender distribution, occupational status, type of work contract, special medication reimbursements, or purchases of analgesics and antidepressants (Table II). However, the participants in the specific FM courses were younger than the participants in non-specific musculoskeletal rehabilitation (mean age 48.6 vs 51.0 years) and they were less frequently entitled to special medication reimbursement for the treatment of chronic or severe disease (32% vs 43%). Prescribed analgesics were used by half (54%) of all patients with FM, and antidepressants by 28–40% of all patients with FM. Compared with all permanently employed employees working in the service of the 10 towns, the patients with FM had a significantly higher prevalence of chronic and severe diseases (37% vs 17%), and a 5-fold quantity of annual analgesic and antidepressant purchases calculated in DDDs. The mean annual number of sickness absence days for the patients with FM was 58.0 (SD 71.0), while the corresponding figure for all employees was 14.9 (SD 30.5).
| Table II. Baseline characteristics of the fibromyalgia (FM) rehabilitees participating in two different rehabilitation interventions. Figures are given as percentages, unless otherwise stated |
| | Specific FM course (n = 121) | Non-specific musculoskeletal rehabilitation (n = 94) | p |
| Gender, men/women | 5/95 | 3/97 | 0.521 |
| Mean age, years (SD) | 48.6 (7.0) | 51.0 (5.4) | 0.007 |
| Age group |
| < 40 years | 9 | 3 | |
| 40–50 years | 48 | 38 | |
| > 50 years | 43 | 59 | 0.039 |
| Occupational status |
| Non-manual | 69 | 57 | |
| Manual | 31 | 43 | 0.060 |
| Work contract |
| Permanent | 92 | 91 | |
| Temporary | 8 | 9 | 0.949 |
| Special medication reimbursement for a chronic disease*, yes/no | 32/68 | 43/57 | 0.119 |
| Purchases of prescribed analgesics* |
| None | 48 | 45 | |
| < 100 DDD | 31 | 38 | |
| ≥ 100 DDD | 21 | 17 | 0.544 |
| Mean DDDs/year (SD) | 56.0 (96.1) | 50.3 (104.3) | 0.678 |
| Purchases of prescribed antidepressants* |
| None | 60 | 72 | |
| < 100 DDD | 19 | 12 | |
| ≥ 100 DDD | 21 | 16 | 0.167 |
| Mean DDDs/year (SD) | 67.0 (152.4) | 44.1 (125.8) | 0.240 |
| Annual sickness absence days*, mean (SD) | 58.0 (71.0) | 69.2 (83.5) | 0.312 |
| *In the year of intervention. p = for difference between the groups. FM: fibromyalgia; SD: standard deviation; DDD: defined daily dose. |
Sickness absence after rehabilitation
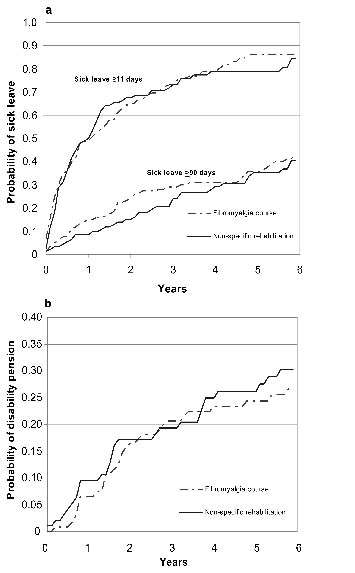
Fig. 1 shows that there was no difference in the risk of sickness absence between the rehabilitation groups during the 6-year follow-up. Fifty percent of the patients with FM had a sick-leave spell during the first year following the rehabilitation, and 80–82% by the end of the follow-up. The percentages for very long sick-leave were 10–15% and 40%, respectively. Table III shows the HR of sickness absence for the participants in the specific FM courses compared with the participants of non-specific musculoskeletal rehabilitation, adjusted for age, occupational status, and special medication reimbursements.
Fig. 1. Cumulative hazard functions of the first long (≥ 11 days) and very long (≥ 90 days) sick-leave (a), and disability pensions (b) among the rehabilitees participating in specific fibromyalgia courses and non-specific musculoskeletal rehabilitation.
Disability pensions
No difference was found in the occurrence of disability pensions between the 2 groups. During the 6-year follow-up, 26% (31 / 121) of the rehabilitees in the specific FM courses and 29% (27 / 94) of the rehabilitees in non-specific musculoskeletal rehabilitation were granted disability pension (Fig. 1, Table III). In addition, the proportions of musculoskeletal or non-musculoskeletal diagnoses as the primary indication for disability pension did not differ between the rehabilitation groups.
| Table III. The risk of the participants of the specific FM courses compared with the participants of non-specific musculoskeletal rehabilitation for all long (≥ 11 days) sick-leave, very long (≥ 90 days) sick-leave due to all causes, musculoskeletal and non-musculoskeletal causes, for all disability pensions, and disability pensions due to musculoskeletal and non-musculoskeletal causes. Adjusted for age, occupational status, and entitlement to special medication reimbursement |
| | Cases in specific FM courses | Cases in non-specific FM rehabilitation | Hazard ratio | 95% CI |
| Sick-leave ≥ 11 days | 99/121 | 75/94 | 1.02 | 0.75–1.40 |
| Sick-leave ≥ 90 days, all causes | 46/121 | 33/94 | 1.18 | 0.75–1.87 |
| Sick-leave ≥ 90 days, musculoskeletal cause* | 20/94 | 15/81 | 1.40 | 0.71–2.78 |
| Sick-leave ≥ 90 days, non-musculoskeletal cause* | 15/94 | 12/81 | 0.99 | 0.45–2.17 |
| Disability pension, all causes | 31/121 | 27/94 | 1.07 | 0.63–1.83 |
| Disability pension, musculoskeletal cause | 13/121 | 19/94 | 0.68 | 0.33–1.39 |
| Disability pension, non-musculoskeletal cause | 18/121 | 8/94 | 2.07 | 0.85–5.03 |
| *Diagnoses for sick-leave are available from 1997 onwards. FM: fibromyalgia; CI; confidence interval. |
We also compared work disability after intervention between the rehabilitees with a diagnosis of FM (n = 94) and with other musculoskeletal diagnosis (n = 2423) in the non-specific musculoskeletal rehabilitation courses. After adjustments for age, occupational status and special medication reimbursements, the risk of work disability was not significantly different among the FM rehabilitees compared with the non-FM rehabilitees in the same non-specific musculoskeletal rehabilitation courses: HRs (95% CI) for sick-leave > 11 days, for sick-leave > 90 days and for disability pension were 1.22 (0.96–1.53), 1.30 (0.92–1.85) and 1.12 (0.76–1.67), respectively.
DISCUSSION
Contrary to our hypothesis, the rehabilitation course specifically designed for patients with FM was not superior to non-specific rehabilitation for patients with musculoskeletal disorders in this observational study of 215 patients with FM. In line with previous studies (4, 6, 10) co-morbidity was common among the FM rehabilitees, as indicated by the high proportion of special medication reimbursements. Co-morbidity is a possible explanation for the very high incidence of temporary and permanent disability found among the FM rehabilitees at baseline and through the 6-year follow-up after the intervention.
The two interventions
The two intervention programmes differed with respect to the content and proportion of education and with respect to the strenuousness of physical exercise. Many studies have suggested a combination of education and exercise to be more effective in revealing symptoms and disability than education alone (23–25).
In rehabilitation provided for FM patients, education has been shown to enhance self-efficacy and promote self-management of symptoms (26). A Swedish qualitative study on coping strategies among working women with FM emphasized that a “grieving process” was a prerequisite for managing with chronic symptoms (27). The ability to grieve and to accept the situation is probably best achieved by providing information and education. In this long and difficult process a cognitive behavioural approach may also be important. More individualized educational interventions have been called for, but participation in a small group of 6–10 people is preferred (12). The results of the present study, using work disability-related outcome measures, do not suggest any additional benefit attributed to small-group education or other deepened FM-specific educational content of FM rehabilitation.
In a prospective study of patients with FM with a 4.5-year follow-up, an adequate physical activity level predicted positive outcome (16). A meta-analysis of aerobic exercise programmes suggested a substantial improvement in tender-point pain threshold and a reduction in pain rating among the FM participants; in the programmes the aerobic exercises were performed at 55–90% of the predicted maximum heart rate for a minimum of 20 min at least twice a week (28). This type of moderate to high intensity aerobic exercise programme is typical in the non-specific musculoskeletal rehabilitation, but not in the specific FM courses provided by the SII. However, the low to moderate level of aerobic exercise usually applied in the FM courses has also been suggested to improve symptom-related well-being (29). The present study provides no preference for lower or higher level aerobic exercise in FM rehabilitation in terms of reduced work disability as an outcome measure.
Bearing in mind the latest recommendations for the management of FM, the programme of FM courses provided by the SII may need some reconsidering. In a recent review article on EULAR1 evidence-based recommendations for management of FM, emphasis was put on a tailor-made content of the rehabilitation programme (30). While FM is a polysymptomatic disorder, perhaps having several mechanisms of pathogenesis, it may be impossible for a group of rehabilitees to benefit maximally from a single particular programme. In the same review article the authors state, based on expert opinion, that cognitive behavioural therapy may be beneficial for some patients with FM. In the FM courses the role of the cognitive behavioural approach was fragmental.
When comparing the 2 interventions, in addition to the content of the programmes, there was a considerable difference in the mean lengths of the rehabilitation periods and especially in the time-spans of the process between the groups. Considering the time needed to change coping mechanisms, the length of the rehabilitation process may be of crucial importance. It remains open as to whether FM courses with longer periods and a lengthened time-span would have been more beneficial for patients with FM.
Work disability
Many prior investigations have reported on substantial and long-term work disability among patients with FM (31–34). In an American study, patients with FM showed the lowest employment figures among the patients of a specialized chronic fatigue clinic (31). A Swedish study on female patients with FM at a university hospital pain and rheumatology clinic reported 50% of patients to be employed, 15% full-time. The employment status had changed for 58% of working women (32). The results of these studies are in line with our study.
In our study, both temporary and long-term work disability was common among the patients with FM. While all the employees of the same organizations had 14.9 (SD 30.5) days of sickness absence in a year, the patients with FM showed a 4-fold increase in the number of sick-leave days. After the intervention, long sick-leave accumulated rapidly among the patients with FM. The probability of any sick-leave was 2-fold and that of very long (≥ 90 days) sick-leave 3-fold for the patients with FM compared with all employees after adjustments for gender, age, occupational status, and entitlement to special medication reimbursement. During the 6-year follow-up period, the corresponding adjusted HR for permanent disability was also 3-fold for patients with FM in both intervention groups compared with all employees.
However, work disability was also very common among the employees with musculoskeletal disorder other than FM. We found no significant differences in the work disability outcomes when comparing the results of the FM rehabilitees and the non-FM rehabilitees of non-specific musculoskeletal rehabilitation of the SII.
While FM seems to be a serious work disability problem, evidence on the effects of rehabilitation programmes is scarce or lacking. In a German study with a 2-year observation period, the work disability status of patients with FM did not change, regardless of therapies received (34). A Finnish non-controlled study with a 1-year follow-up period on the effects of FM rehabilitation courses (similar to those examined in the present study) did not show any benefit in terms of work capacity (33). One-third of the rehabilitees who were employed at the baseline were granted disability pension by the end of the follow-up. Our results accord with those of the previous studies. We found no differences in the risk of future work disability between the 2 intervention programmes for patients with FM. In the present study, 26% of the specific FM course rehabilitees and 29% of the non-specific musculoskeletal rehabilitation rehabilitees were granted disability pension within 6 years after the intervention. The risk for disability pension with the main diagnosis other than a musculoskeletal disease appeared to be higher among the rehabilitees of the specific FM courses than among the non-specific musculoskeletal rehabilitation rehabilitees, but the difference was not significant.
Strengths and limitations
The strengths of our study include reliable and pertinent data collected from the national registers and the employers´ records. The fact that the participants in each of the interventions were from the same work organizations decreases the likelihood of recording bias.
The main limitation of our study is the lack of a randomization in the intervention groups. For an assessment of treatment efficacy, a randomized controlled study design provides the best protection against bias and confounding. Our study was an observational one, conducted in a real-life setting, and the programmes of the two interventions were pragmatic, guided by the SII instructions. There were no disease- or symptom-specific criteria for the allocation of patients with FM to either the FM-specific intervention group or the non-specific musculoskeletal intervention group. A limitation is that we did not have data about the duration of symptoms or social situation other than work of the patients with FM. We assessed morbidity of the participants on the basis of data available from the registers and found no baseline differences between the two intervention groups. The only essential difference was age: the participants in the non-specific musculoskeletal rehabilitation programme were older than those participating in the FM-specific intervention. Because our analyses were adjusted for age, occupational status, and prevalence of special medication reimbursement (as a marker of common morbidity), the finding of a similar risk of sickness absence and work disability irrespective of the type of intervention is unlikely to result from major differences between the two groups.
In conclusion, work disability, both temporary and permanent, is high among patients with FM. Participation in a specific FM rehabilitation programme demonstrated no additional benefit over a non-specific musculoskeletal rehabilitation programme in preventing work disability. The contents of the specific FM courses provided by the SII may need reconsidering according to the recent recommendations about the non-pharmacological treatment of FM. More research is needed for the purpose of developing effective treatment and rehabilitation programmes in order to control the burden of work disability related to FM.
ACKNOWLEDGEMENTS
This study was supported by the Social Insurance Institution of Finland, the Academy of Finland (projects 117604, 124322 and 124271), and the participating towns.
REFERENCES
1. Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C, Goldenberg DL, et al. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum 1990; 33: 160–172.
2. Henriksson KG. Fibromyalgia – from syndrome to disease. Overview of pathogenetic mechanisms. J Rehabil Med 2003; 35 Suppl 41: 89–94.
3. Kosek E, Ekholm J, Hansson P. Sensory dysfunction in patients with fibromyalgia with implications for pathogenic mechanisms. Pain 1996; 68: 375–383.
4. Wolfe F, Cathey MA. Prevalence of primary and secondary fibrositis. J Rheumatol 1983; 10: 965–968.
5. White KP, Harth M. Classification, epidemiology, and natural history of fibromyalgia. Curr Pain Headache Rep 2001; 5: 320–329.
6. Nampiaparampil DE, Shmerling RH. A review of fibromyalgia. Am J Manag Care 2004; 10: 794–800.
7. Wolfe F, Ross K, Anderson J, Russell IJ, Hebert L. The prevalence and characteristics of fibromyalgia in the general population. Arthritis Rheum 1995; 38: 19–28.
8. Bruusgaard D, Evensen AR, Bjerkedal T. Fibromyalgia – a new cause for disability pension. Scand J Soc Med 1993; 21: 116–119.
9. Kassam A, Patten SB. Major depression, fibromyalgia and labour force participation: a population-based cross-sectional study. BMC Musculoskelet Disord 2006; 7: 4.
10. Kivimaki M, Leino-Arjas P, Kaila-Kangas L, Virtanen M, Elovainio M, Puttonen S, et al. Increased sickness absence among employees with fibromyalgia. Ann Rheum Dis 2007; 66: 65–69.
11. Berger A, Dukes E, Martin S, Edelsberg J, Oster G. Characteristics and healthcare costs of patients with fibromyalgia syndrome. Int J Clin Pract 2007; 61: 1498–1502.
12. Mannerkorpi K, Henriksson C. Non-pharmacological treatment of chronic widespread musculoskeletal pain. Best Pract Res Clin Rheumatol 2007; 21: 513–534.
13. Henriksson C, Carlberg U, Kjallman M, Lundberg G, Henriksson KG. Evaluation of four outpatient educational programmes for patients with longstanding fibromyalgia. J Rehabil Med 2004; 36: 211–219.
14. Karjalainen K, Malmivaara A, van Tulder M, Roine R, Jauhiainen M, Hurri H, et al. Multidisciplinary rehabilitation for fibromyalgia and musculoskeletal pain in working age adults. Cochrane Database Syst Rev 2000; CD001984.
15. Goldenberg DL, Burckhardt C, Crofford L. Management of fibromyalgia syndrome. JAMA 2004; 292: 2388–2395.
16. van Koulil S, Effting M, Kraaimaat FW, van Lankveld W, van Helmond T, Cats H et al. Cognitive-behavioral therapies and exercise programmes for patients with fibromyalgia: state of the art and future directions. Ann Rheum Dis 2007; 66: 571–581.
17. Wigers SH, Stiles TC, Vogel PA. Effects of aerobic exercise versus stress management treatment in fibromyalgia. A 4.5 year prospective study. Scand J Rheumatol 1996; 25: 77–86.
18. Vahtera J, Kivimaki M, Pentti J, Linna A, Virtanen M, Virtanen P, et al. Organisational downsizing, sickness absence, and mortality: 10-town prospective cohort study. BMJ 2004; 328: 555.
19. Suoyrjo H, Hinkka K, Kivimaki M, Klaukka T, Pentti J, Vahtera J. Allocation of rehabilitation measures provided by the Social Insurance Institution in Finland: a register linkage study. J Rehabil Med 2007; 39: 198–204.
20. Guidelines for ATC classification and DDD assignment. Oslo: WHO Collaborating Centre for Drug Statistics Methodology; 2006.
21. Marmot M, Feeney A, Shipley M, North F, Syme SL. Sickness absence as a measure of health status and functioning: from the UK Whitehall II study. J Epidemiol Community Health 1995; 49: 124–130.
22. Kivimaki M, Forma P, Wikstrom J, Halmeenmaki T, Pentti J, Elovainio M, et al. Sickness absence as a risk marker of future disability pension: the 10-town study. J Epidemiol Community Health 2004; 58: 710–711.
23. Hammond A, Freeman K. Community patient education and exercise for people with fibromyalgia: a parallel group randomized controlled trial. Clin Rehabil 2006; 20: 835–846.
24. Lemstra M, Olszynski WP. The effectiveness of multidisciplinary rehabilitation in the treatment of fibromyalgia: a randomized controlled trial. Clin J Pain 2005; 21: 166–174.
25. van Wilgen CP, Bloten H, Oeseburg B. Results of a multidisciplinary program for patients with fibromyalgia implemented in the primary care. Disabil Rehabil 2007; 29: 1207–1213.
26. Burckhardt CS. Educating patients: self-management approaches. Disabil Rehabil 2005; 27: 703–709.
27. Lofgren M, Ekholm J, Ohman A. “A constant struggle”: successful strategies of women in work despite fibromyalgia. Disabil Rehabil 2006; 28: 447–455.
28. Busch A, Schachter CL, Peloso PM, Bombardier C. Exercise for treating fibromyalgia syndrome. Cochrane Database Syst Rev 2002; CD003786.
29. Richards SC, Scott DL. Prescribed exercise in people with fibromyalgia: parallel group randomised controlled trial. BMJ 2002; 325: 185.
30. Carville S F, Arend-Nielsen S, Bliddal H, Blotman F, Branco J C, Buskila D, et al. EULAR evidence-based recommendations for the management of fibromyalgia syndrome. Ann Rheum Dis 2008; 67: 536–541.
31. Assefi NP, Coy TV, Uslan D, Smith WR, Buchwald D. Financial, occupational, and personal consequences of disability in patients with chronic fatigue syndrome and fibromyalgia compared with other fatiguing conditions. J Rheumatol 2003; 30: 804–808.
32. Henriksson C, Liedberg G. Factors of importance for work disability in women with fibromyalgia. J Rheumatol 2000; 27: 1271–1276.
33. Hyyppä MT, Kronholm E, Leino A, Viitanen J. Stability of chronic pain/fatigue and the effect of rehabilitation courses in fibromyalgia patients. The Social Insurance Institution, Finland, Turku 1998; Studies in Social Security and Health 30: 1–78 (English summary).
34. Noller V, Sprott H. Prospective epidemiological observations on the course of the disease in fibromyalgia patients. J Negat Results Biomed 2003; 2: 4.