OBJECTIVES: To quantify the reaction forces exerted under the hands, feet and buttocks when individuals with spinal cord injury performed sitting pivot transfers.
DESIGN: Twelve men with paraplegia completed 3 transfers between seats of the same height (0.5 m high) and 3 transfers to a high target seat (0.6 m high).
RESULTS: Greater mean and peak vertical reaction forces were always recorded under the hands compared with the feet (p < 0.001) during the transfers. Mean vertical reaction forces were similar between the leading and trailing hands (p > 0.088) for the 2 transfers studied. However, the mean vertical reaction force underneath the leading hand was greater when transferring between a seat of the same height compared with one of a higher height (p = 0.021) and vice-versa for the trailing hand (p = 0.0001). The peak vertical reaction force always occurred earlier (p < 0.0001) and was greater underneath the trailing hand compared with the leading one (p < 0.02), and reached its highest value when transferring to the high target seat (p = 0.003). Peak and mean horizontal reaction forces were always higher underneath the trailing hand compared with the leading hand (p < 0.001).
CONCLUSION: These results provide evidence-based data to better understand transfers and strengthen clinical practice guidelines targeting the preservation of upper extremity integrity.
Key words: biomechanics, kinetics, rehabilitation, technology, upper extremity, weight-bearing.
J Rehabil Med 2008; 40: 468–476
Correspondence address: Dany Gagnon, School of Rehabilitation, University of Montreal, Pavillon 7077 Avenue du Parc, PO Box 6128, Station Centre-Ville, Montreal, Quebec, Canada H3C 3J7. E-mail: dany.gagnon.2@umontreal.ca
Submitted July 28, 2007; accepted January 22, 2008
INTRODUCTION
Individuals who sustain a spinal cord injury (SCI) generally experience severe axial skeleton and lower extremity (LE) sensory-motor impairments, which reduce their ability to ambulate (1). To overcome this disability and reach an optimal level of social participation, most of these individuals will become long-term manual wheelchair users (1, 2). Their upper extremities (UEs) consequently become highly involved during manual wheelchair propulsion and many other basic functional mobility activities, such as overhead reaching, weight-lift manoeuvres and transfer tasks (3). Among these activities, transfer tasks rank among the most strenuous wheelchair-related activities, especially for the skeletal, muscular, neurological and vascular UE structures (3–6). Surprisingly, there is a paucity of biomechanical studies focusing on transfer tasks among individuals with SCI.
Individuals with complete motor paraplegia, as well as those with low-level tetraplegia (C7–C8), generally develop the ability to transfer themselves in a seated position from an initial surface to a target surface of even or uneven height, without human or physical assistance (7). To transfer, individuals with SCI predominantly rely on their UEs to lift their buttocks off the initial surface and almost simultaneously pivot themselves to the target surface (7). While doing so, the hand generally placed beside the upper thigh on the initial seat is referred to as the trailing hand, whereas the leading hand is positioned on the target seat, far enough away to leave adequate space for the buttocks at the end of the transfer (7). Typical sitting pivot transfer examples include transferring from a wheelchair to a regular bed, a bath-tub/shower bench, a toilet seat, a treatment table, a car seat and vice versa. Interestingly, individuals with SCI on average perform 14–18 of these transfers per day (8, 9) and frequently encounter height differences between seating surfaces while doing so (10). Such a great number of transfers performed daily, along with the elevated forces transmitted through the wrist, elbow and shoulder joints while carrying out these tasks, may increase the risk of developing secondary UE musculoskeletal impairments over time (3). This belief is further supported by the high prevalence of shoulder (30–60%), elbow (5–16%) and wrist (40–66%) joint complaints documented among individuals with SCI (3).
Comprehensive assessment of the reaction forces during sitting transfers towards even and uneven surfaces would definitively represent a key advancement in an effort to better assess sitting pivot transfers. To date, only Forslund et al. (10) have reported recording peak vertical forces, representing approximately 50% of the total body weight of men with SCI, under the leading hand at seat-off and then under the leading hand during sitting transfer. Moreover, they noticed a tendency for the trailing arm to be exposed to a greater mean vertical force (32% of body weight) than the leading arm (24.5% of body weight) (10). To our knowledge, neither the antero-posterior and medio-lateral reaction forces generated during sitting transfers performed independently by individuals with SCI, nor the percentage of bodyweight supported by the LEs have ever been described. Knowledge gained from a better understanding of the external forces acting on the body segments may enhance the current knowledge regarding sitting pivot transfers, and strengthen clinical practice guidelines targeting the preservation of UE integrity among individuals with SCI.
The main objective of this study was to quantify the 3 orthogonal components of the reaction forces exerted under the hands, feet and buttocks when individuals with SCI performed sitting pivot transfers to a target seat of both the same and higher heights. The study design also allowed the researchers to compare the magnitude of the reaction forces between the leading and trailing hands and to investigate the effect of target seat height on these reaction force outcomes (mean and peak values) during the lift phase of the transfers. The influence of SCI level on the reaction force outcomes was also investigated. Substantially more elevated vertical reaction force was anticipated underneath the hands (leading and trailing hands combined) in comparison to the one recorded underneath the feet during the lift phase of the sitting pivot transfers, since individuals with complete motor paraplegia experience severe LE impairments. Yet, the magnitude of the vertical reaction force recorded underneath feet during the lift phase of the sitting pivot transfer was expected to be representative of the weight of the LEs. Sitting pivot transfers from an initial seat to a target seat of the same height was also expected to generate lower reaction forces underneath the leading and trailing hands compared with the transfer to a higher target seat, as transferring to a higher target surface may require supplementary UE efforts, as previously demonstrated during a comparable task (11). Moreover, higher reaction forces were also anticipated underneath the trailing hand compared with the leading hand during sitting transfers, as recently reported (10). Lastly, the reaction forces were expected to increase as the level of SCI led to improved sensory-motor capability (lower level of SCI) among the participants as their abdominal and trunk muscles may have an increased capability to generate and counteract axial skeletal accelerations (head and trunk segments combined), especially around seat-off during the sitting pivot transfers (12).
METHODS
Participants
A convenience sample of 12 right-handed men (mean age 41.5 years, age range 21–54 years) with complete traumatic sensory-motor thoracic SCI volunteered for this study (Table I). Subjects were eligible to participate if they had the ability to independently perform sitting transfers between seats of various heights without technical aids, and they routinely used sitting transfers in daily life. Participants presented no subjective or objective signs or symptoms of musculoskeletal impairments affecting the trunk or UEs or any other condition limiting their ability to perform sitting transfers. Ethical approval was obtained from the Research Ethics Committee of the Centre for Interdisciplinary Research in Rehabilitation of Greater Montreal (CRIR). Participants reviewed and signed an informed consent form before entering the study.
| Table I. Description of participants |
| Subjects | Age (years) | Height (m) | Weight (kg) | Time since injury (years) | ASIA- Motor (/100) | ASIA- Sensory (/224) | Level of injury | Number of transfers (/day) | Transfer tasks* |
| Same height | High height |
| 1 | 39.0 | 1.85 | 105.2 | 5.3 | 50 | 112 | T7 | 22 | * | * |
| 2 | 44.8 | 1.73 | 105.3 | 5.0 | 50 | 144 | T11 | 18 | * | * |
| 3 | 49.3 | 1.78 | 86.1 | 4.8 | 50 | 88 | T4 | 24 | * | * |
| 4 | 54.1 | 1.70 | 63.8 | 31.7 | 50 | 104 | T6 | 22 | * | * |
| 5 | 51.7 | 1.88 | 88.7 | 33.5 | 50 | 144 | T11 | 11 | * | * |
| 6 | 33.8 | 1.83 | 80.7 | 2.4 | 50 | 92 | T4 | 24 | * | * |
| 7 | 27.5 | 1.75 | 64.4 | 3.6 | 50 | 100 | T5 | 16 | * | * |
| 8 | 38.1 | 1.73 | 51.3 | 6.9 | 50 | 92 | T4 | 22 | * | * |
| 9 | 31.8 | 1.68 | 75.0 | 2.8 | 50 | 88 | T4 | 35 | * | * |
| 10 | 37.5 | 1.58 | 63.3 | 3.5 | 50 | 128 | T9 | 7 | * | |
| 11 | 48.7 | 1.85 | 104.6 | 6.4 | 50 | 111 | T6 | 20 | * | |
| 12 | 41.6 | 1.72 | 93.6 | 3.2 | 50 | 96 | T5 | 20 | * | * |
| Mean | 41.5 | 1.76 | 81.8 | 9.1 | 50 | 108.3 | | 20 | | |
| SD | 8.4 | 0.09 | 18.5 | 11.1 | 0 | 20.3 | | 7 | | |
| *Successfully completed the experimental task. ASIA: American Spinal Injury Association; SD: standard deviation. |
Reaction force recording
A force-sensing system was developed to continuously record reaction forces underneath the feet, buttocks and leading and trailing hands during transfers (Fig. 1). This system is comprised of 2 instrumented chairs positioned beside one another with a 25° angle separating the 2 seats, as illustrated in Fig. 2. The initial seat is build with a unique Advanced Medical Technology Inc (AMTI) force plate, whereas the target seat is equipped with 4 separate AMTI strain gauge transducers (13, 14). Both sitting surfaces are mounted on an aluminium plate and supported by a large steel structure. A slide-guide rail system is embedded into each structure and allows for height-adjustments using manual cranks. In fact, a scissor jack-type crank is attached underneath the sitting surface of each chair and is also connected to the steel structure. Moreover, a manual locking mechanism is integrated to the structure to further secure the selected seat height. Both instrumented chairs were anchored to the concrete floor to optimize their natural frequency and dissipate vibrations during data collection. High-density foam (thickness 0.01 m) covered the seating surfaces to preserve skin integrity during the experiment. To monitor the reaction forces generated under the hands, 2 additional custom-made width- and height-adjustable hand force plates, each equipped with 3 AMTI strain gauge transducers, were mounted laterally to square steel shafts fixed underneath the chairs, with additional steel supports projecting to the floor to optimize the rigidity of the system. For each participant, the hand force plates were adjusted to ensure that the width of the seats corresponded to that of their own wheelchair. Finally, 2 additional AMTI force plates embedded into the floor recorded forces transmitted through the feet. This innovative experimental set-up allowed for continuous recording, amplifying and storing of the x, y and z components of the resulting external reaction forces at a sampling frequency of 600 Hz during the entire duration of the transfers using a custom-made Labview program. Subsequently, forces recorded during transfers were filtered using a fourth-order Butterworth zero-lag filter, with a cut-off frequency of 10 Hz and sampled at 60 Hz. The x, y and z components of the reaction forces corresponded to the antero-posterior (Fx), vertical (Fy) and medio-lateral (Fz) directions, respectively, within the global coordinate framework of the laboratory (Fig. 2). The x, y and z components of the reaction forces underwent static (y component) and quasi-static (x and z components) accuracy tests, which confirmed measurement errors of less than 2% for each instrumented surface (15). Additional methodological details on the instrumented transfer assessment system have been presented in a previous report (15). Remember that all external reaction forces recorded during the proposed experimental tasks, especially those recorded underneath the hands that are of key interest, are representative of the external loading sustained by the body segment and thus only to some extent indicative of the mechanical strain experienced.
Fig. 1. Force-sensing system developed to continuously record reaction forces underneath the feet, buttocks, leading and trailing hands during transfers in a laboratory environment.
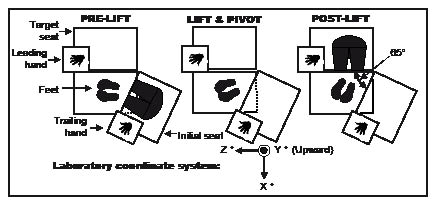
Fig. 2. Laboratory set-up and the pre-lift, lift and post-lift phases of the sitting pivot transfers. Note that the 5 force-sensing surfaces illustrated were continuously recording reaction forces during the completion of the experimental tasks.
Transfer assessment
Participants had to transfer from the initial instrumented chair to the target chair, initially set at a height of 0.5 m (transfer #1: same). This pre-selected height closely matches the height from which participants routinely initiate this type of transfer in daily life as it mimics the combined wheelchair and cushion heights calculated among all participants (mean 0.53 m (standard deviation (SD) 0.02)). The height of the instrumented chairs was not adjusted to specific body anthropometric parameters (e.g. lower leg length) since the combined wheelchair and cushion height was found to be relatively constant across individuals with SCI during a preliminary study (12) and since individuals with SCI are generally encouraged to place their feet firmly on the floor before initiating transfers, independently of the footrest’s height and LE anthropometrics. In addition, transfer surfaces are generally not adjustable in the natural environment (e.g. adapted toilet seat height). As for the width of the instrumented chair, each width-adjustable instrumented hand surface, that overlaps the instrumented seat to which it is laterally attached, was moved so that the width of the instrumented seats corresponded to that of the subject’s own wheelchair. After a familiarization period, 3 transfer trials were recorded for each participant, while the right UE acted as the leading one and the left as the trailing UE. Subsequently, the height of the target seat was positioned 0.1 m higher than the initial one to reach 0.6 m (transfer #2: high). Three additional transfer trials were recorded for each participant. Of importance, since only the height of the target seat was modified, the right UE always acted as the leading UE while the left UE acted as the trailing one. Prior to initiating these transfers, participants were instructed to place their buttocks, feet and hands in a position of preference over the instrumented surfaces, respectively. Initial hand, feet and buttock positions were marked to ensure similar starting positions across trials for each participant. Participants were encouraged to use their regular transfer strategies while transferring, especially in terms of movement amplitude and speed.
Data processing
Each sitting transfer trial was divided into 3 phases: pre-lift, lift and post-lift phases (11, 16, 17). The vertical forces recorded on the initial and target seats marked the start and end of the lift phase of the transfer. The lift phase started when the vertical force equalled zero at the initial seat (seat off) and ended when the impact force reached its maximum value on the target one (seat on). These time events were further validated by verifying the initial and final vertical displacements of the centre of mass of the pelvis. The start of the pre-lift phase corresponded to the start of the acceleration phase of the head and upper trunk segments which preceded the lift phase, while the end of the post-lift phase coincided with the end of the deceleration phase of these same segments. Note that to obtain these kinematic parameters, the co-ordinates of the skin-fixed light emitting diode triads attached to these segments (pelvis, trunk, head) were simultaneously recorded at a sampling frequency of 60 Hz using an Optotrak motion analysis system (Northern Digital Inc., Waterloo, ONT, USA) as previously described (12, 15). Thereafter, custom-made programs were used to quantify angular displacements, velocities and accelerations of the head and trunk segments within the laboratory coordinate frame (12, 15). Thereafter, the x, y and z components of the reaction forces were time-normalized to 100 data points per phase for a total of 300 data points for the entire transfer task. Each data point was thereafter normalized as a percentage of body weight (% BW = (reaction force recorded (N) / BW (N))* 100). The levels of SCI lesion were ranked according to an ordinal scale progressing from 1 (C6) to 15 (T12), based on the metameric level of sensory-motor SCI (18).
Statistical analysis
Descriptive statistics (mean, SD) were calculated for the demographic and clinical characteristics of the participants. For each participant (n = 12), the x, y and z components of the time-normalized reaction forces (300 data points) recorded over each instrumented surface when performing the 3 sitting pivot transfers to the target seat set at a height of 0.5 m (transfer #1: same) were averaged. Thereafter, a group mean (SD) pattern was generated for the x, y and z components of the reaction forces recorded at each of the 5 instrumented surface by averaging all participants’ averages for this experimental task (Fig. 3). A similar approach was also used to generate a group mean (SD) pattern for the x, y and z components of the reaction forces recorded over each instrumented surface when performing sitting pivot transfers to the target seat positioned 0.1 m higher than the initial one (transfer #2: high) for the participants who successfully complete this task (n = 10). The reaction force pattern similarity among the participants was analysed using the mean Pearson product-moment correlation coefficient (rmean) (19). To calculate the rmean, each participant’s pattern was first correlated against the group mean pattern. Then, a rmean was calculated by averaging the coefficient of correlation obtained for each participant for a given reaction force pattern (19). The rmean values were interpreted according to the guidelines proposed by Altman (20): poor agreement (r ≤ 0.20), fair (r = 0.21–0.40), moderate (r = 0.41–0.60), good (r = 0.61–0.80) and very good (r = 0.81–1.00). Then, mean and peak values of the vertical reaction forces were extracted for the lift phase of the transfers only for the participants who had completed both experimental tasks underneath the feet and hands (leading and trailing). As for the mean and peak values of the horizontal vertical forces distinctively reported underneath the leading and trailing hands, the magnitude of these vales were characterized after adding the x and z components of the reaction force recorded underneath the hand using proper trigonometric method (Pythagoras’ theorem; Fhorizontal2 = Fx2+Fz2). These outcomes (mean and peak vertical and horizontal forces) were only computed during the lift phase, since this phase represents the most demanding phase of the transfer as previously demonstrated (17). Using the values extracted, 2-factor repeated-measures analysis of variance (ANOVA) [2 supporting surfaces (hands vs feet) × 2 target seat heights (same vs high)] was used to confirm the substantial supporting role of the UEs compared with the LEs when performing transfers. For each participant, note that all values (300 data points) used to generate the mean pattern of the vertical (y) component of the reaction force obtained underneath the leading and trailing hands were combined to compute the data (mean ad maximum) needed to complete this analysis. Another 2-factor repeated-measures ANOVA [2 hand roles (leading vs trailing) × 2 target seat heights (same vs high)] was used to assess the differences between the leading and trailing hands during the same tasks using the outcomes previously described (vertical and horizontal forces). An additional 2-factor repeated-measures ANOVA [3 supporting surfaces (leading hand, trailing hand, feet) × 2 target seat heights (same vs high)] was used to compare the time of occurrence of the peak vertical reaction forces (Fy). For all ANOVAs, main effects were examined to determine the influence of the factors investigated in the absence of interaction. Additional analyses were carried out to determine main independent variable effects on the dependent variables whenever an interaction effect was detected. To do so, one-way ANOVAs (Bonferroni correction applied) as well as paired or independent Student’s t-tests were performed to determine whether differences existed. Lastly, Spearman rank coefficients of correlation were used to establish the association between the mean and maximum values of each component of the reaction force (Fx, Fy, Fz) recorded underneath the hand (leading and trailing) and feet instrumented surfaces, as well as the mean and maximum overall reaction force (all instrumented surfaces combined) values, with respect to the level of SCI expressed on an ordinal scale. Two-tailed tests were selected for all statistical analysis and p-values of 0.05 or less confirmed statistical significance. All statistical analyses were performed using SPSS® software, version 11.5.
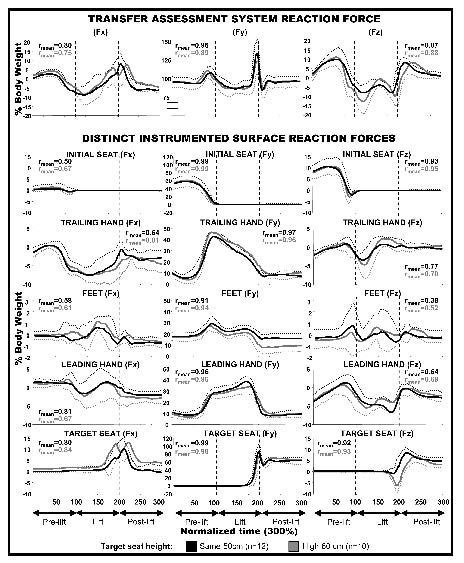
Fig. 3. Time-normalized group mean (standard deviation (SD)) values of the three-dimensional components measured with the transfer assessment system (all force-sensing surfaces combined into one) and of its partition under each distinct instrumented surface (hands (leading and trailing hands), feet and buttocks (initial and target seats)) during the sitting transfers. The mean coefficients of correlation (rmean) are also documented for all patterns illustrated. Note that different scales have been used to better illustrate reaction force (% body weight) given the substantial magnitude in differences.
RESULTS
Participants
The characteristics of the participants are summarized in Table I. All participants were male and had sustained a traumatic SCI on average 9.1 (SD 11.1) years ago. The lesion level varied from T4 to T11 and participants were classified as either American Spinal Injury Association (ASIA) grade A or grade B on the impairment scale (18). Their mean age, stature and body mass index (BMI) were 41.5 (SD 8.4) years, 1.76 (SD 0.09) m and 81.8 (SD 18.5) kg, respectively. As a group, they were slightly overweight with an averaged BMI of 26.4 (SD 5.1) (21). Participants self-reported to perform on average over 20 (SD 7) sitting transfers daily during the week (7 days) prior to the laboratory assessment during a standardized semi-structured interview during which various types of sitting pivot transfers were discussed (close- and open-ended questions). Moreover, they all had the ability to transfer to a seat of the same height (n = 12), whereas only 10 participants succeeded in transferring to the target seat that was 0.1 m higher than the initial one.
Mean time-normalized reaction force patterns
Mean (1 SD) patterns of the x, y and z reaction force components exerted under the hands (leading and trailing UEs), feet and buttocks during the 2 sitting transfers studied are shown in Fig. 3. Typically, the vertical component was always more elevated than the antero-posterior and medio-lateral components for all reaction forces recorded. When specially studying the vertical component, it is easy to note that individuals with SCI usually shift the weight underneath their buttocks (initial seat) toward their hands and feet as their vertical reaction forces quickly increase until seat-off, with additional weight (higher vertical force) being initially shifted to the trailing hand. The trailing hand is then progressively unloaded (decline in vertical force) as an increase in the vertical force is observed under the leading hand as their trunk, abdomen, pelvis and LEs are moved toward the target seat. The lift phase ends with a forceful impact recorded at the target seat. At this time, the buttocks once again support most of the body weight (target seat) and relieve the amount of weight supported by the hands and feet. The antero-posterior and medio-lateral reaction forces represented less than 15% body weight for the majority of participants. Note that all participant’s mean profiles, that were averaged to obtain group mean patterns, were found to be very similar (rmean ≥ 0.89) across participants for the vertical components of the reaction force, whereas mostly moderate to good similarity levels (rmean ≥ 0.39) were found for the 2 horizontal components of the reaction force for both experimental tasks.
Vertical reaction forces during lift phase
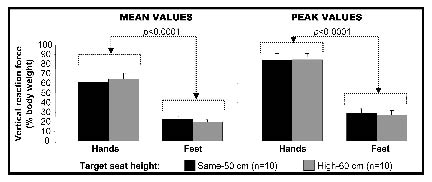
The mean and peak vertical reaction forces exerted under the hands and feet during the lift phase are presented in Fig. 4. Although the mean (same = 22.9%; high = 19.6%) and maximum (same = 29.1%; high = 27.6%) vertical forces recorded under the feet were considerable, the mean (p < 0.0001) and maximum (p < 0.0001) forces were clearly greater under the hands (mean: same = 61.3%; high = 64.4%; maximum: same = 84.1%; high = 84.5%) during the lift phase of the transfers.
Fig. 4. Mean (standard deviation (SD)) and peak (SD) vertical force components measured under the hands and feet during the lift phase of the sitting pivot transfers.
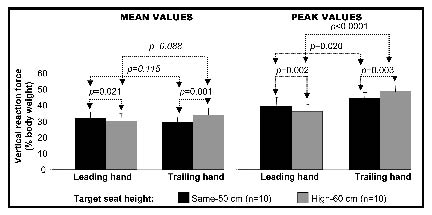
The mean and peak vertical reaction forces recorded separately under the trailing and leading hands are illustrated in Fig. 5. For the mean vertical reaction forces, only target seat height (same vs high) was found to have had a statistically significant effect when looking at each hand separately. For the trailing hand, higher (p = 0.001) mean vertical reaction force was recorded when transferring toward the high target seat (34.1%) compared with the one of the same height (29.4%) and vice-versa for the leading hand (p = 0.021) that reached a greater mean vertical reaction force when transferring to the target seat of the same height (same = 31.9% vs high = 30.3%). Similar mean vertical reaction forces were found between the leading and trailing hands (same = 31.9% vs 29.4%; high = 30.3% vs 34.1%) when transferring toward a target seat of same (p = 0.115) or higher height (p = 0.088) than the initial seat. For the peak vertical reaction forces, both hand roles (leading vs trailing) and target seat heights (same vs high) were found to have had a significant effect. The trailing hand supported a greater peak vertical reaction force (same = 44.5%; high = 48.6%) than the leading hand (same = 39.6%; high = 36%) during the 2 transfer tasks tested (psame height = 0.020 and phigh height < 0.0001). Moreover, the trailing hand supported additional (p = 0.003) vertical reaction force when transferring to the high seat (48.6%) compared with the one of same height (44.5%). As for the leading hand, the lowest (p = 0.002) peak vertical reaction force was recorded when transferring toward the high target seat (same = 39.6%; high = 36%).
Fig. 5. Mean (standard deviation (SD)) and peak (SD) peak vertical force components measured under the leading and trailing hand during the lift phase of the sitting pivot transfers.
Horizontal reaction forces during lift phase
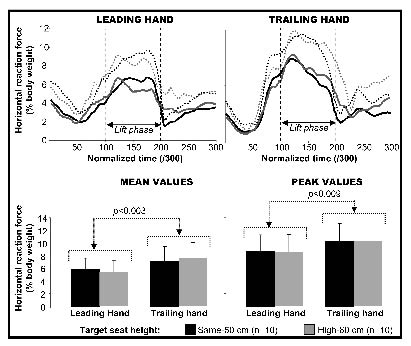
The mean and peak horizontal reaction forces recorded separately under the trailing and leading hands are shown in Fig. 6. The mean (p < 0.003) and maximum (p < 0.009) horizontal forces were significantly greater under the trailing hand (mean: same = 7.1%; high = 7.6%; peak: same = 10.2%; high = 10.4%) in comparison to the leading hand (mean: same = 5.9%; high = 5.4%; peak: same = 8.8%; high = 8.6%) during the lift phase of the transfers, independently of the target seat height, which was found to have no effect.
Fig. 6. Time-normalized group mean (standard deviation (SD)) values of the horizontal reaction force measured underneath the leading and trailing hands during sitting pivot transfers. Mean (SD) and peak (SD) peak horizontal force components measured under the leading and trailing hand during the lift phase of the sitting pivot transfers.
Timing of peak vertical reaction force
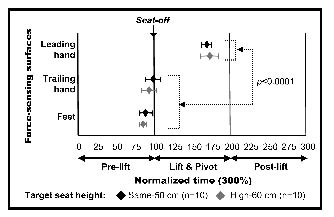
The peak vertical reaction force exerted under the trailing hand (same = 99.8; high = 94.3) and feet (same = 90.1; high = 86.5) occurred earlier than the force recorded under the leading hand (same = 171.2; high = 169.5) when transferring, independent of the target seat height (p < 0.0001), as shown in Fig. 7. The peak vertical reaction force exerted under the trailing hand and feet was observed approximately at seat-off, whereas the force under the leading hand was observed during the second half of the lift phase.
Fig. 7. Mean (standard deviation (SD)) timing of the peak vertical force components measured under the hands (leading and trailing hands) and feet during the sitting pivot transfers.
Effect of SCI levels
No significant association was found between the level of SCI and the mean or peak force components when all instrumented surfaces are combined into one (Fx: r = –0.368 to 0.176; Fy: r = –0.181 to 0.552; Fz: r = –0.406 to 0.176) for the transfer tasks studied. Similar finding also confirmed no significant effect of the level of SCI on the mean or peak force components (Fx, Fy, Fz) distinctively measured under the hands (trailing and leading hands) and feet (r = –0.368 to 0.176). Scatter plot diagrams were also examined to further validate these results.
DISCUSSION
The objective of this study was to quantify three-dimensional reaction forces exerted under the hands, feet and buttocks when individuals with SCI performed sitting transfers toward target seats of same and higher heights than the initial seat. Although a portion of the body weight is supported by the LEs during the transfers, these results confirm that a substantial portion of the body weight is transferred through the UEs. The peak vertical reaction forces reported were always higher and occurred earlier at the trailing hand when compared with the leading hand during sitting transfers, independent of the target seat height. Conversely, similar mean vertical reaction forces were measured between the leading and trailing hands when transferring, independent of the target seat height. As for the horizontal reaction forces, mean and peak values were found to be more elevated under the trailing hand when compared with the leading hand, independent of the target seat height. Note that the consistent reaction force patterns found across participants, especially for its vertical components, further support the findings of this study.
The important weight-bearing role played by UEs among individuals with SCI, especially during the lift phase of transfers, is definitively confirmed in this study. The rapid trunk flexion generally observed when individuals with SCI initiate sitting transfers may partly explain the results found around seat-off time (12). The combination of the high forward flexion velocity of the trunk-head segment, along with the prominent mass of this key segment (head-trunk), produces a momentum that is probably responsible for the initial horizontal force (Fz) developing on the initial seat during the pre-lift phase. This momentum may also facilitate the rapid vertical unloading observed at the initial seat at this time (12). Almost simultaneously, vertical and horizontal reaction forces rise beneath the hands possibly to counteract this flexion angular momentum in order to prevent a forward fall given the trunk’s musculature impairment and facilitate lift-off from the initial seat. Around this transition period (seat-off), asymmetric vertical and horizontal forces were recorded underneath the hands, with the peak values recorded under the trailing hand exceeding those under the leading hand (vertical: trailing ~40% vs leading ~25% of body weight; horizontal: trailing ~8% vs leading ~4% of body weight). The substantial vertical reaction forces recorded under the hands, combined to the horizontal forces, are most likely linked to high mechanical demands placed on the shoulder flexors and adductors and elbow extensors, especially under the trailing hand, to initiate the lift phase, optimize UE joint stability and ensure dynamic postural stability (15). Then the trailing hand rapidly unloads as additional weight is shifted toward the leading hand until the beginning of the impact on the target seat. Contrary to the hypothesis initially formulated, the level of SCI lesion had no significant effect on the mean and peak vertical and horizontal reaction forces measured under the hands and feet. However, careful interpretation of these findings remains warranted given the limited number of participants included in this study and their distribution with respect to their level of SCI. Other factors known to potentially affect reaction forces, or interact with level of SCI lesion, may also need to be considered in future research (e.g. UE strength, LE spasticity, time since SCI).
The results of this study yield partial support for the hypothesis suggesting that transferring to a target seat 0.1 m higher than the initial seat may require added UE efforts. As the target seat height was augmented, only the mean (+4.7%) and peak (+4.1%) vertical reaction force values recorded underneath the trailing hand increased. Surprisingly, the mean (–1.6%) and peak (–3.6%) vertical reaction force values measured underneath the leading hand slightly declined during this period. Raising the height of the target seat height had no effect on the horizontal forces recorded underneath both hands. As for the hypothesis suggesting higher reaction forces underneath the trailing hand compared with the leading hand during sitting transfers, the results of this study strongly support it. The peak vertical and horizontal reaction forces were always higher underneath the trailing hand in comparison to the leading hand when transferring to a target seat of same (vertical = +4.9%; horizontal = +1.4%) or higher height (vertical = +12.6%; horizontal = +1.8%) than the initial seat. Only the mean horizontal reaction forces recorded underneath the trailing hand were more elevated than those underneath the leading hand when transferring to a target seat of same (+1.2%) or higher height (+2.2%) than the initial seat. Though no statistically significant difference was found when examining the mean vertical reaction values, the results remains clinically relevant as additional vertical load was recorded under the trailing hand in comparison to the leading hand when transferring to a target seat of the same (+25%) or higher height (+3.8%) than the initial seat. This last finding may be linked to the limited number of participant included in this study, which may have reduced its statistical power. Note that differences presented above in parentheses reflect absolute differences.
Although only a few studies have investigated UE muscle activity using an electromyographical (EMG) approach during sitting transfers, their results help to elucidate some of the findings of the current study. There is evidence suggesting that the elevated mean and peak vertical and horizontal reaction forces measured under the hands during the lift phase of the transfer may be accompanied by moderate (25–50% EMGmax) to high (> 50% EMGmax) UE muscular demand needed to generate the shoulder and elbow moments during this period (9, 17). However, no significant EMG muscular demand difference has yet been documented between the leading and the trailing UEs during the lift phase of the transfer, despite a tendency for the trailing UE to be exposed to a higher demand compared with the leading UE for the rotator cuff muscles, specifically the infraspinatus (45% vs 37%), supraspinatus (38% vs 12%) and subscapularis (19% vs 8%) muscles (17). The higher mean and peak horizontal forces recorded underneath the trailing hand in the current study, which may be indicative of the rotational (torsion) demands challenging the rotator cuff muscles at the shoulder (gleno-humeral joint), strengthen the results of the EMG study. Conversely, a tendency for the leading UE to generate higher EMG muscular demand than the trailing UE during the lift phase of the SPTs has been proposed for 2 key thoraco-humeral muscles, specifically the pectoralis major (81% vs 49%) and latissimus dorsi (40% vs 25%) (17). When considering the effects of the target seat height, one should also consider that higher EMG activity of the anterior deltoid and pectoralis major of the trailing UE, probably to generate large shoulder flexion moment, was recently found when transferring toward a high target seat compared with one of the same height (22). This may be needed to counteract the highest peak vertical reaction force (Fy) observed under the trailing hand when transferring toward the high target seat and may facilitate the interpretation of the strong tendency observed for the mean vertical reaction force (Fy) (p = 0.088). As for the earlier occurrence of the peak vertical reaction force (Fy) under the trailing hand compared with the leading hand, similar findings have been found when studying peak EMG intensity values in a previous study (22). In fact, this study reported that the peak EMG values for the anterior deltoid and pectoralis major muscles were observed earlier with the trailing UE when compared with the leading UE and occurred at seat-off, independent of the target seat height (22). These 2 muscles possibly have to generate explosive shoulder flexion and adduction moments along with an elbow extension moment to counterbalance the elevated vertical and horizontal forces measured beneath the trailing hand early during the lift phase of the transfer.
The contribution of the LEs is frequently under-estimated in clinical practice given the severe sensory-motor impairments affecting these segments after a SCI. In conformity with the hypothesis, the LEs supported almost 30% of the body weight (Fy) during the sitting transfers investigated despite severe LE sensory-motor impairments. This approximately represents the percentage of body weight allocated to these segments (LE = 16.1% of total mass) based on the parameters proposed by Dempster (23), although this may represent an over-estimation. Such an over-estimation may result from the fact that significant muscle atrophy and decline in bone mineral density are frequently observed in the LEs following SCI (24). Interestingly, it is possible that additional LE joint stiffness, especially at the ankles, may enhance their stability, thereby enabling these segments to support additional weight during transfers. This hypothesis remains to be investigated.
The antero-posterior and medio-lateral components of the reaction forces recorded at the initial and target seats should not be neglected, although they were not scrutinized in this study. The fact that participants pivoted within the laboratory coordinate system when transferring from the initial seat to the target one, added to the orientation of the initial seat and trailing hand instrumented surfaces, make the interpretation of these horizontal force components more complex than those captured when assessing gait or sit-to-stand tasks, which are predominantly realized in the sagittal plane of movement, for instance. Overall, the intensity of the antero-posterior and medio-lateral components of the total reaction forces substantiates that dynamic postural stability is crucial when performing sitting pivot transfers. To this end, the horizontal reaction forces recorded on the target seat at the completion of the lift phase, for example, may be representative of the intensity of the destabilizing force that must be neutralized upon landing to prevent a fall (25), although this hypothesis remains to be verified. The peak vertical component of the total reaction force, which occurs almost simultaneously to the horizontal ones, must also be considered as it may contribute to secure sitting balance upon landing on the target seat (elevated upward linear acceleration). The antero-posterior and medio-lateral components of the total reaction forces may also be indicative of the shear-friction forces sustained underneath the buttocks at the time of the transfer, which, combined with the substantial vertical force, may jeopardize skin integrity under the bony prominences of the buttocks.
No clear consensus has yet been established on the specific role played by each UE during transfers when muscle strength imbalance or secondary UE impairments exist. However, some authors have started to advocate the use of the strongest UE, or of the pain-free one, as the trailing one when performing sitting transfers (3, 10, 17). Promoting the use of the strongest UE, or of the pain-free one, as the trailing one when performing sitting transfers toward a target seat higher than the initial one, is definitively indicated in light of the vertical and horizontal reaction force results found in this study as well as in previous ones (10, 17). Yet, additional biomechanical evidences may contribute to reinforce the recommendation suggesting the use of the strongest UE as the trailing one in clinical practice when transferring between seats of same heights. This suggestion is primarily based on the fact that the mean vertical reaction forces were similar under the hands as observed in this study and on the results of the EMG analysis previously conducted by Perry et al. (17), which revealed no significant difference between the leading and trailing UEs as well as high inter-participant variability during the lift phase of the transfer. However, the highest peak vertical reaction force, added to the highest mean and peak horizontal reaction forces, documented underneath the trailing hand when transferring between seats of the same height support the appropriateness of using the strongest UE, or the pain-free one, as trailing UEs, especially in the presence of a rotator cuff muscle tendinopathy for example. The fact that the dominant UE (right UE), which is typically slightly stronger than the non-dominant UE, always assumed the leading role during transfers in this study may also have had an effect on the relative distribution of the reaction forces between both UEs. This may have altered the relative reaction force distribution between the trailing and leading hands in favour of the leading hand in the current study. Before endorsing the use of the strongest pain-free UE as the trailing one when performing sitting pivot transfers in clinical practice, one must remember that many other parameters aside from the vertical and horizontal reaction forces (e.g. target seat heights, UE strength differences, affected musculoskeletal structures) also need to be considered (3). Future research should attempt to assess the effects of target seat heights, not only on the distribution of the reaction forces, but also on the relative EMG and mechanical demands sustained by the leading and trailing UEs during sitting pivot transfers.
In conclusion, the three-dimensional reaction forces confirm that the UEs contribute to the generation and control of multi-joint movements and play a key role in sophisticated dynamic motor control required when performing sitting transfers. To this end, most of the body weight was found to be supported by the UEs, especially during the lift phase of the sitting transfers, although the LEs supported part of the body weight. Peak vertical reaction forces reported in this study were always higher and occurred earlier underneath the trailing hand when compared with the leading hand during sitting transfers, while similar mean vertical reaction forces were documented between hands, independent of the target seat height. Peak and mean horizontal reaction forces were always higher underneath the trailing UE compared with the leading UE, independent of target seat height. Additional research is suggested before definitively advocating the use of the strongest UE or pain-free UE as the trailing one when performing sitting transfers in clinical practice guidelines for rehabilitation professionals.
ACKNOWLEDGEMENTS
Special thanks are extended to Pierre Desjardins (Eng, MSc), Michel Goyette (Eng), France Piotte (PT, MSc), Daniel Marineau and André Dumoulin for their engineering and technical support. The authors also acknowledge the financial support provided by the Quebec Rehabilitation Research Network (www.repar.ca), Lindsay Rehabilitation Hospital Foundation, and the Canadian Foundation for Innovation. Dany Gagnon holds a PhD scholarship and Sylvie Nadeau holds a Junior 2 Research Scholarship from the Fond de la recherche en santé du Québec (FRSQ). Patrick Dehail holds a postdoctoral scholarship from the REPAR.
REFERENCES
1. Fougeyrollas P, Noreau L, Boschen K. The interaction of environment with individual characteristics and social participation: theoretical perspectives and applications in persons with spinal cord injury. Top Spinal Cord Inj Rehabil 2002; 7: 1–16.
2. Noreau L, Fougeyrollas P, Post M, Asano M. Participation after spinal cord injury: the evolution of conceptualization and measurement. J Neurol Phys Ther 2005; 29: 147–156.
3. Consortium for Spinal Cord Medicine Clinical Practice Guidelines. Preservation of upper limb function following spinal cord injury: a clinical practice guideline for health-care professionals. First edn. Washington, DC: Paralyzed Veteran of America; 2005.
4. Van Drongelen S, Van der Woude LH, Janssen TW, Angenot EL, Chadwick EK, Veeger HEJ. Mechanical load on the upper extremity during wheelchair activities. Arch Phys Med Rehabil 2005; 86: 1214–1220.
5. Van Drongelen S, Van der Woude LH, Janssen TW, Angenot EL, Chadwick EK, Veeger HEJ. Glenohumeral contact forces and muscle forces evaluated in wheelchair-related activities of daily living in able-bodied subjects versus subjects with paraplegia and tetraplegia. Arch Phys Med Rehabil 2005; 86: 1434–1440.
6. Bayley JC, Cochran TP, Sledge CB. The weight-bearing shoulder. The impingement syndrome in paraplegics. J Bone Joint Surg Am 1987; 69: 676–678.
7. Bromley I, editor. Tetraplegia and paraplegia: a guide for physiotherapists. Fifth edn. Edinburgh, UK: Churchill Livingstone; 1998.
8. Pentland WE, Twomey LT. Upper limb function in persons with long term paraplegia and implications for independence: Part II. Paraplegia 1994; 32: 219–224.
9. Finley MA, McQuade KJ, Rodgers MM. Scapular kinematics during transfers in manual wheelchair users with and without shoulder impingement. Clin Biomech 2005; 20: 32–40.
10. Forslund EB, Granstrom A, Levi R, Westgren N, Hirschfeld H. Transfer from table to wheelchair in men and women with spinal cord injury: coordination of body movement and arm forces. Spinal Cord 2006; 45: 41–48.
11. Gagnon D, Nadeau S, Gravel D, Noreau L, Lariviere C, McFadyen B. Movement patterns and muscular demands during posterior transfers toward an elevated surface in individuals with spinal cord injury. Spinal Cord 2005; 43: 74–84.
12. Gagnon D, Nadeau S, Noreau L, Eng J, Gravel D. Trunk and upper extremity kinematics during sitting pivot transfers performed by individuals with spinal cord injury. Clin Biomech 2008; 23: 279–290.
13. Roy G, Nadeau S, Gravel D, Piotte F, Malouin F, McFadyen BJ. Side difference in the hip and knee joint moments during sit-to-stand and stand-to-sit tasks in individuals with hemiparesis. Clin Biomech 2007; 22: 795–804.
14. Roy G, Nadeau S, Gravel D, Malouin F, McFadyen BJ, Piotte F. The effect of foot position and chair height on the asymmetry of vertical forces during sit-to-stand and stand-to-sit tasks in individuals with hemiparesis. Clin Biomech 2006; 21: 585–593.
15. Gagnon D, Nadeau S, Desjardins P, Noreau L. Biomechanical assessment of sitting pivot transfer tasks using a newly-developed instrumented transfer system among long-term wheelchair users. J Biomech 2008; 41: 1104–1110.
16. Gagnon D, Nadeau S, Gravel D, Noreau L, Lariviere C, Gagnon D. Biomechanical analysis of a posterior transfer maneuver on a level surface in individuals with high and low-level spinal cord injuries. Clin Biomech 2003; 18: 319–331.
17. Perry J, Gronley JK, Newsam CJ, Reyes ML, Mulroy SJ. Electromyographic analysis of the shoulder muscles during depression transfers in subjects with low-level paraplegia. Arch Phys Med Rehabil 1996; 77: 350–355.
18. American Spinal Injury Association. Reference Manual for the International Standards for Neurological Classification of Spinal Cord Injury. Chicago: American Spinal Injury Association (ASIA); 2003.
19. Trevithick BA, Ginn KA, Halaki M, Balnave R. Shoulder muscle recruitment patterns during a kayak stroke performed on a paddling ergometer. J Electromyogr Kinesiol 2007; 17: 74–79.
20. Altman DG, editor. Practical statistics for medical research. 1st edn. London: Chapman & Hall/CRC; 1991.
21. World Health Organization. Physical status: the use and interpretation of anthropometry. Report of a WHO Expert Committee. Geneva: World Health Organization; 1995.
22. Gagnon D, Nadeau S, Noreau L, Eng J, Gravel D. Upper extremity muscle activation patterns during sitting pivot transfers performed by individuals with complete spinal cord injury. J Electromyogr Kinesiol 2008; Feb 9 [Epub ahead of print].
23. Winter DA, editor. Biomechanics and Motor Control of Human Movement. Toronto: John Wiley & Sons; 1990.
24. Giangregorio L, McCartney N. Bone loss and muscle atrophy in spinal cord injury: epidemiology, fracture prediction, and rehabilitation strategies. J Spinal Cord Med 2006; 29: 489–500.
25. Duclos C, Desjardins P, Nadeau S, Delisle A, Gravel D, Brouwer B, et al., editors. A model based on the “destabilising force” to assess the dynamic stability during functional tasks. In: Innovations in balance and locomotor rehabilitation: the translation from fundamental science to clinical applications. Satellite preconference of the XVIIIth International Society for Posture and Gait Research Conference; 2007 July 13th, 2007; Montreal, Canada; 2007.