OBJECTIVE: The aim of this study was to evaluate possible differences between local social insurance offices with regard to their selection of clients for vocational rehabilitation.
A further aim was to determine whether social insurance officers from different local insurance offices have uniform attitudes regarding professional practice in their application of the insurance system.
METHODS: A register-based investigation of 815 vocational rehabilitees served by 6 local social insurance offices in a Swedish county. The study was supplemented with a questionnaire to 30 officers about attitudes to social insurance.
RESULTS: The office with the lowest rate of sick-listing periods exceeding one year, and a high frequency of employment training, showed the highest degree of work resumption and the lowest pension rate after vocational rehabilitation. There were wide differences in attitude among the local social insurance officers regarding professional practice in their application of the system.
CONCLUSION: Intra-county differences occur in handling people on sick-leave who undergo vocational rehabilitation. The local social insurance offices with the highest and lowest outcome rates of work resumption and disability pension, respectively, select clients for vocational rehabilitation from different categories of cases. Social insurance officers from different local offices differ in their attitudes towards the social insurance system and its clients.
Key words: disability pension, vocational rehabilitation, work resumption, social insurance, attitudes, chronic pain, psychiatric disorders, sickness absence, outcome.
J Rehabil Med 2008; 40: 178–184
Correspondence address: Åsa Ahlgren, Department of Health Science, Mid Sweden University, SE-851 70 Sundsvall, Sweden. E-mail: asa.ahlgren@miun.se
Submitted March 1, 2007; accepted October 25, 2007
Introduction
In Sweden there are large regional differences with regard to patterns of sick-listing and vocational rehabilitation (VR). There appears to be no single reason for these differences. However, a parliamentary committee report has concluded that the vast local and regional differences indicate deficiencies in the administration of social insurance, and ambiguous application and interpretation of the law (1). Social insurance legislation requires equal access to VR measures regardless of domicile within the country (chapter 22, section 5, Social Insurance Act, 1962: 381) (2). However, VR is not a general civic right, but an opportunity offered to some sick-listed people following prioritization.
Funds in support of VR are allocated to the social insurance offices by the government on an annual basis, earmarked for the “purchase of rehabilitation services”. Since the resources are not in proportion to needs, prioritization is necessary. The internal distribution of tasks in social insurance offices implies that the same group of social insurance officers (SIOs) examines those cases where the aim is work resumption, as well as those cases where the aim is entitlement to disability pension. Accordingly, each officer’s clients present a wide spectrum of possibly relevant health states, levels of functioning, employment situations and other aspects. This raises the question of whether selection to VR is made with regard to the greatest need for VR or to the best chances of work resumption, regardless of the actual need for VR. Where rehabilitation is channelled to those clients with the lowest functional status (i.e. the greatest objective need), the rate of return to work is likely to be low (3).
Although an important part of VR is the SIO’s role in decision-making, few studies focus on the decision-making process between SIOs and their clients, or the interaction between different parties (4, 5). SIO is not considered a profession in its own right. SIOs may have a range of professional backgrounds and an educational level ranging from 9 years compulsory schooling to a university degree. A success factor emphasized in VR is access to a professional mentor from the private, occupational or healthcare arenas. Such personal encounter and treatment has a considerable effect on the outcome of VR (6, 7).
When economic means are limited, selection is necessary. Hence clients who receive VR have been prioritized in relation to others and, together with, for example, duration of sickness absence and demographics; this influences the outcome after VR. Complete analysis is impossible due to the complexity of the VR process and how different factors affect outcome. The present study is confined to testing previous findings (8, 9) against the reasoning that a selection underlies decisions about VR and that there is a link between the criteria for this selection and the outcome of VR. Understanding the significance of selection is important for the interpretation of VR outcomes.
It is reasoned here that SIOs play a part in this selection through their double role: on the one hand they are responsible for measures aiming at work resumption; on the other for investigation of remaining working ability prior to decisions about disability pension grants.
Definitions
Combined measures. The objective of combined measures is to use local co-operation among authorities involved in VR. The aim of combined rehabilitation measures is to create long-lasting solutions as regards employment/work/occupation/livelihood. Measures may consist of, for example, job training or practice, vocational guidance and opportunities for study.
Clients undergoing investigation are considered as rehabilitation clients. Investigation is used to attain a deeper medical, physical and/or psychological assessment of, for example, the pain condition and/or the mobility limitation, in order to facilitate appropriate planning for the client’s future. Considerations include, for example, whether the reduced working ability is seen as short-term or long-term, estimated work ability, whether the reduced ability is general or if the pain relates to certain tasks or work areas. Investigation may further be used to assess the client’s right to various allowances.
Aim of the study
The objective was to study intra-county local differences in the handling of sick-leavers taking part in VR. One element of particular interest was whether any existing differences in outcome could be related to differences in the procedure for selecting clients to VR.
The following specific questions were addressed:
• Do SIOs from different local insurance offices select clients for VR differently?
• Do SIOs from different local insurance offices share attitudes regarding professional practice in their application of the insurance system?
Subjects and Methods
Study design
The study included a register investigation of all 832 rehabilitation cases (RC), i.e. those granted a rehabilitation measure, at any of 6 local public insurance offices in a county in Southern Norrland, Sweden, during 1998 and 1999. All clients in the study were registered as rehabilitation cases regardless of the type of measure. Furthermore, all clients received rehabilitation allowance.
The study considered the type of VR measure and its outcome. Outcomes were followed up through database studies after completion of VR and 24 months thereafter. The variables recorded were: gender, age, employment, duration of sickness, including duration of rehabilitation allowance (days), diagnosis, VR measures, and outcome of VR. The outcome was considered as social insurance status reported on closure of the sickness case (at the end of the sickness period with allowance), and could be: “fully fit”, “granted temporary or permanent disability pension”, “full- or part-time work” or “sick leave”. The diagnosis registered was the diagnosis first stated as the reason for sick-listing.
Between 1998 and 2002, no major amendments of the Act on Public Social Insurance (1962: 381) (2) were made that significantly affect the SIOs’ administration of rehabilitation cases. Accordingly, the time gap between the register study in 1998 and the inquiry in 2002 is not considered to be critical to the conclusions drawn.
Subjects
Of the 832 rehabilitation cases, 14 were excluded due to maternity allowance or parental allowance granted within 24 months after completed VR, and 3 had died. The study was therefore based on the remaining 815 cases. No selection was made with regard to form of employment or duration of sick leave.
The study was approved by the ethics committee of Karolinska Institutet (KI dnrs: 02-258 and 03–373) and by the regional social insurance office.
Questionnaire study
The study also included a questionnaire answered by SIOs working with VR at the 6 offices in autumn 2002. The response frequency was 83%, i.e. 30 of 36 SIOs.
Part 1 of the 2-part questionnaire comprised 11 statements related to attitudes towards sick-listing and the persons involved. Possible answers were “agree”, “disagree” or “neither-nor” and respondents were instructed to tick the statement that best corresponded to their view. The inquiry is based on a series of questions previously used in a Swedish pilot investigation concerning differences in attitudes among SIOs. Parts of that study have been presented as a report from the National Social Insurance Board.
Part 2 consisted of open questions related to the attitudes and professional practice of the SIOs. Some SIOs gave more than one answer to each question, and all answers were presented. The purpose was to display the range of attitudes.
Before the questionnaires were distributed, an introductory note was sent to office managers. After briefing, the SIOs completed the questionnaires on 3 occasions. The first author informed the respondents of the purpose of the questionnaire, took no active part in answering, and collected the forms.
Statistics
SPSS version 12.0, with 5% significance level, was used to indicate statistical significance. For comparing duration of sick leave and age group, the Mann-Whitney U test or the Kruskal-Wallis test was used.
Gender, employment, diagnosis, VR measures and outcome were compared using the ordinary χ2 test or the phi coefficient and Cramer’s V.
For comparing the answers to part 1 of questionnaire, a Kruskal-Wallis test was used; for part 2, frequencies were used
Results
Return-to-work rate and social insurance status
The outcomes immediately after the VR period at the 6 offices (A–F) differed significantly (p = 0.025). The differences were no longer apparent at the 2-year follow-up.
Office B showed the highest degree of work resumption (Table I) immediately after VR (59.2%) as well as at the 2-year follow-up (44.7%). Office B also showed the lowest rate of full-time permanent disability pension grants (10.5%). Office C showed the lowest rate (24%) of work resumption and the highest rate of full-time permanent disability pension grants (28%). For all offices, except C and D, the rate of full-time temporary pension grants declined from the completion of VR to the 2-year follow-up, while full-time permanent disability pension increased for all offices (Table I).
| Table I. Proportions of clients (n=815) at the 6 local social insurance offices A–F working (at work or study), work-ready but unemployed, sick-listed, and/or on disability pension. |
| | A n = 297 | B n = 76 | C n = 25 | D n = 50 | E n = 212 | F n = 155 |
| |
| | AR % | 2 yrs % | AR % | 2 yrs % | AR % | 2 yrs % | AR % | 2 yrs % | AR % | 2 yrs % | AR % | 2 yrs % |
| At work | 37.7 | 25.6 | 59.2 | 44.7 | 24.0 | 28.0 | 48.0 | 40.0 | 43.4 | 35.4 | 39.4 | 32.3 |
| Unemployed | 11.1 | 6.7 | 5.3 | 6.6 | 16.0 | 4.0 | 14.0 | 6.0 | 11.3 | 3.8 | 9.7 | 3.9 |
| Sicklisted | 1.0 | 13.1 | 1.3 | 6.6 | 0.0 | 16.0 | 0.0 | 14.0 | 0.5 | 15.6 | 1.3 | 13.5 |
| TDP part time | 6.7 | 4.0 | 3.9 | 0.0 | 16.0 | 4.0 | 4.0 | 4.0 | 9.0 | 3.8 | 3.2 | 0.6 |
| PDP part time | 16.8 | 17.8 | 9.2 | 15.8 | 12.0 | 8.0 | 12.0 | 10.0 | 9.9 | 11.3 | 12.9 | 12.9 |
| TDP full time | 11.4 | 8.8 | 10.5 | 7.9 | 4.0 | 4.0 | 4.0 | 4.0 | 11.3 | 9.0 | 13.5 | 9.0 |
| PDP full time | 15.2 | 23.9 | 10.5 | 18.4 | 28.0 | 36.0 | 18.0 | 22.0 | 14.6 | 21.2 | 20.0 | 27.7 |
| TDP: temporary disability pension, part-time and full-time; PDP: permanent disability pension, part-time and full-time; AR: after completed vocational rehabilitation; 2 yrs: 2 years later. |
Two groups of employers predominated at the various locations (Table II). In municipalities A, D, E and F, geriatric care and medical care were the most frequent employers and in municipalities B and C the highest proportion of employers were in industry. B was dominated by small and middle-sized companies and C by one major industrial employer. No statistically significant difference between the offices was demonstrated with regard to type of employer or employment.
| Table II. Differences between the six municipalities A-F, where the offices were located with regard to type of employment of the cases. |
| | Municipalities |
| | A n = 297 | B n = 76 | C n = 25 | D n = 50 | E n = 212 | F n = 155 |
| |
| Employer | n | % | n | % | n | % | n | % | n | % | n | % |
| Unemployed | 80 | 26.9 | 10 | 13.2 | 6 | 24.0 | 13 | 26.0 | 52 | 24.5 | 43 | 27.7 |
| Public sector | 112 | 37.7 | 22 | 28.9 | 5 | 20.0 | 17 | 34.0 | 73 | 34.4 | 48 | 31.0 |
| Trade and constraction | 54 | 18.2 | 14 | 18.4 | 4 | 16.0 | 9 | 18.0 | 38 | 17.9 | 37 | 23.9 |
| Industry | 16 | 5.4 | 26 | 34.2 | 6 | 24.0 | 6 | 12.0 | 41 | 19.4 | 21 | 13.5 |
| Other | 35 | 11.8 | 4 | 5.3 | 4 | 16.0 | 5 | 10.0 | 8 | 3.8 | 6 | 3.9 |
All the municipalities except C showed significant gender differences by type of employment. The men worked primarily in industry and the women in elderly care and medical care.
There was no statistically significant difference between the offices regarding clients’ gender, age distribution, employment or diagnosis.
There were statistically significant differences between the offices concerning sick-leave periods and VR measures chosen. Office B showed the second lowest figures (Table III) for sick-listing exceeding 2 years (27.6%) and used employment training (76.3%) and studies (11.8%) to a greater extent than the other offices.
| Table III. Differences between the six local social insurance offices A-F with regard to the cases’ gender, age, employment, sick-leave, diagnosis and VR measures received. Investigation = more detailed investigation. |
| | A n = 297 | B n = 76 | C n = 25 | D n = 50 | E n = 212 | F n = 155 | p |
| | n | % | n | % | n | % | n | % | n | % | n | % |
| Gender | | | | | | | | | | | | | ns |
| Men | 102 | 34.3 | 30 | 39.5 | 11 | 44.0 | 21 | 42.0 | 74 | 34.9 | 57 | 36.8 | |
| Women | 195 | 65.7 | 46 | 60.5 | 14 | 56.0 | 29 | 58.0 | 138 | 65.1 | 98 | 63.2 | |
| Age | | | | | | | | | | | | | ns |
| 16–29 | 18 | 6.1 | 3 | 3.9 | 3 | 12.0 | 3 | 6.0 | 9 | 4.2 | 15 | 9.7 | |
| 30–39 | 62 | 20.9 | 20 | 26.3 | 5 | 20.0 | 10 | 20.0 | 51 | 24.1 | 42 | 27.1 | |
| 40–49 | 100 | 33.7 | 23 | 30.3 | 9 | 36.0 | 16 | 32.0 | 57 | 26.9 | 42 | 27.1 | |
| 50–59 | 105 | 35.4 | 29 | 38.2 | 8 | 32.0 | 14 | 28.0 | 89 | 42.0 | 54 | 34.8 | |
| 60–64 | 12 | 4.0 | 1 | 1.3 | 0 | 0.0 | 7 | 14.0 | 6 | 2.8 | 2 | 1.3 | |
| Employment | | | | | | | | | | | | | ns |
| Employed | 216 | 72.7 | 66 | 86.8 | 19 | 76.0 | 37 | 74.0 | 159 | 75.0 | 112 | 72.3 | |
| Unemployed | 81 | 27.3 | 10 | 13.2 | 6 | 24.0 | 13 | 26.0 | 53 | 25.0 | 43 | 27.7 | |
| Sick-leave period, days | | | | | | | | | | | | | 0.001 |
| 1–90 | 32 | 11.0 | 12 | 15.8 | 3 | 12.5 | 0 | 0.0 | 11 | 5.2 | 9 | 5.8 | |
| 91–180 | 28 | 9.7 | 12 | 15.8 | 1 | 4.2 | 9 | 18.4 | 28 | 13.3 | 12 | 7.8 | |
| 181–365 | 64 | 22.1 | 17 | 22.4 | 3 | 12.5 | 7 | 14.3 | 60 | 28.4 | 25 | 16.2 | |
| 366–730 | 69 | 23.8 | 14 | 18.4 | 4 | 16.7 | 18 | 36.7 | 56 | 26.5 | 41 | 26.6 | |
| >731 | 97 | 33.4 | 21 | 27.6 | 13 | 54.2 | 15 | 30.6 | 56 | 26.5 | 67 | 43.5 | |
| Diagnosis | | | | | | | | | | | | | ns |
| Musculoskeletal | | | | | | | | | | | | | |
| disorders/pain | 165 | 55.9 | 38 | 50.0 | 16 | 64.0 | 29 | 58.0 | 108 | 51.2 | 72 | 46.8 | |
| Reumatoid arthritis | | | | | | | | | | | | | |
| and arthrosis | 28 | 9.5 | 3 | 3.9 | 1 | 4.0 | 2 | 4.0 | 11 | 5.2 | 15 | 9.7 | |
| Psychiatric diseases | | | | | | | | | | | | | |
| and disorders | 42 | 14.2 | 19 | 25.0 | 4 | 16.0 | 11 | 22.0 | 42 | 19.9 | 38 | 24.7 | |
| Cardiovascular diseases | 24 | 8.1 | 6 | 7.9 | 0 | 0.0 | 6 | 12.0 | 17 | 8.1 | 5 | 3.2 | |
| Other | 36 | 12.2 | 10 | 13.2 | 4 | 16.0 | 2 | 4.0 | 33 | 15.6 | 24 | 15.6 | |
| Measures | | | | | | | | | | | | | <0.001 |
| Job training | 122 | 41.1 | 58 | 76.3 | 16 | 64.0 | 28 | 56.0 | 116 | 54.7 | 85 | 54.8 | |
| Studies | 23 | 7.7 | 9 | 11.8 | 1 | 4.0 | 2 | 4.0 | 7 | 3.3 | 13 | 8.4 | |
| Physical exercise | 17 | 5.7 | 0 | 0.0 | 1 | 4.0 | 10 | 20.0 | 6 | 2.8 | 2 | 1.3 | |
| Combined measures | 40 | 13.5 | 2 | 2.6 | 0 | 0.0 | 1 | 2.0 | 51 | 24.1 | 28 | 18.1 | |
| Investigation | 95 | 32.0 | 7 | 9.2 | 7 | 28.0 | 9 | 18.0 | 32 | 15.1 | 27 | 17.4 | |
| VR: vocational rehabilitation; ns: not significant. |
Office C had most sick-listing exceeding 2 years (54.2%) and the second highest proportion of detailed investigation as a VR measure (28%).
Combined measures were rarely used, but when used this was at the larger offices (A, E and F).
Results of questionnaire section regarding SIOs´ attitudes
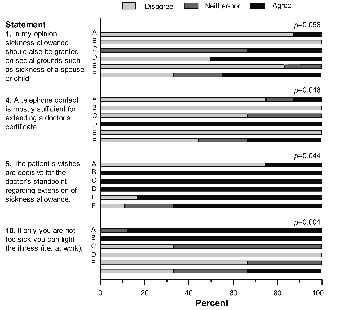
The 11 statements listed below were given. No statistically significant differences were demonstrated for statements 2, 3, 6, 7, 8, 9 and 11. There were, however, statistically significant differences for statements 4, 5 and 10, and a tendency towards significance (p = 0.056) for statement 1. The latter is of particular interest, since it indicates the attitude that there is room for accepting sickness allowance to be granted on social grounds, although this runs counter to its legal restriction to medical grounds only (Fig. 1).
Fig. 1. Distribution of responses among social insurance officers, from 6 local social insurance offices A–F, to the questionnaire about attitudes. Statements 1, 4, 5 and 10.
1. In my opinion sickness allowance should also be granted on social grounds, such as sickness of a spouse or child.
A majority (60%) of the SIOs did not agree that sickness allowance should be granted for social reasons. A comparison between the offices indicated different attitudes in this respect (Fig. 1). Office B responded with “not affirmative”, whereas office C was hesitant or “affirmative”.
2. Doctors should see and examine patients prior to any extension of a grant of sickness allowance.
3. Doctors are more inclined to grant sickness allowance to unemployed people due to the specific problems of this group.
4. Telephone contact is mostly sufficient for extending a doctor’s certificate.
A majority (66.7%) of the SIOs did not think that telephone contact was sufficient for extending a period of sickness allowance. None of the SIOs from offices B or E supported the statement, whereas all from office D did so.
5. The patient’s wishes are decisive for the doctor’s standpoint regarding extension of sickness allowance.
A majority (66.7%) of the SIOs agreed that patients’ wishes were important for physicians’ decisions about prolongation of sickness allowance. Offices B, C and D were “affirmative” to the statement. Many from office A were “not affirmative” (Fig. 1).
6. Social insurance sick-listing rules according to the legislation are generous.
7. Getting a grant for sickness allowance from a doctor is easy.
8. Many sick-listed clients are really capable of working.
9. When jobs are scarce, people tend to be more restrictive with calling in sick.
10. If only you are not too sick you can fight the illness (i.e. at work).
Here the distribution of SIOs varied greatly. A and B were “affirmative” to the statement, D were “not affirmative”, as were most from E. The SIOs from office F were fairly evenly distributed over all 3 categories, “not affirmative”, “neither-nor” and “affirmative”.
11. It is hard for an insurance officer to question the position of a treating physician.
Summary of responses: second part of the questionnaire
Question 1. What criteria indicate that a client should receive VR?
SIOs thought the client’s motivation and whether the doctor’s certificate indicated any need constituted the criteria for VR. The opportunity for the client to be given new or modified work tasks were also considered important.
Question 2. What criteria indicate that a client should not be prioritized for VR?
Responses here included low client motivation, impaired function as a consequence of health condition, and age close to retirement pension.
Question 3. What factor or factors do you consider have the greatest significance for a sick-listed client to return to work?
The client’s own motivation, active support from the employer, and the employer’s desire to have the employee back.
Question 4. What is your objective in purchasing an investigation?
Assessment of work capacity and creating a base for further planning of the case.
Question 5. Please describe the co-operation between employers, employment office and healthcare and medical care units in VR matters.
Half of the SIOs considered that co-operation between the insurance office, employers, healthcare units and employment office varied from good to very poor. The lowest rating concerning co-operation was found regarding the employment office, where fewer than 40% of the SIOs rated co-operation as satisfactory. A cause of this was difficulties in transferring cases assessed capable of work and consequently available to the labour market.
Question 6. Please describe a good employer/enterprise with regard to VR measures.
A supportive employer, open to opportunities, and with strong commitment to employees. SIOs thought it important that the employer keep in contact with the sick-listed person.
Question 7. What do you think should be done to reduce sickness absence?
The SIOs suggested a wide range of measures, indicating what rehabilitation actor they considered responsible. Within their own authority an increase in staff was considered necessary in order to establish contact with the case at an earlier stage. Improved co-operation with other VR actors was also considered important. The SIOs wanted greater responsibility and improved preventive measures among employers and healthcare units. Few SIOs mentioned that rehabilitation plans should be drawn up.
Increased part-time sick-listing could contribute positively, and physicians should learn more about the social insurance system. Some SIOs thought that economic incentives could reduce sick-listing.
Thus, a variety of opinions was presented, mainly about VR actors other than the social insurance offices.
Question 8. Please give examples of changes you think would improve or facilitate your work as an SIO.
First among factors expected to facilitate and improve VR work was reduced workloads for the SIOs. The heavy workload was considered to hamper early contact with clients.
Question 9. Please give your own estimation of the proportion of VR cases ending with disability pension, full- or part-time.
A majority of the SIOs estimated the proportion of disability pension cases to be about 20%, with a range from 10% to 50%. The actual figure was 46.2%.
Question 10. What do you think influences, and who decides, whether a client will get sickness allowance?
Twenty-eight of 30 SIOs were aware that the decision is the responsibility of the social insurance office. Eight thought that the patient’s and the physician’s views influenced the judgement.
Discussion
The general objective of this study was to evaluate whether local social insurance offices differ with respect to how they select clients for VR. The reasoning is that the dual role of SIOs leads to a selection among sick-listed people eligible for VR, and that the selection influences the outcome of VR with respect to work resumption or disability pension.
The questionnaire sought to ascertain whether there is any coherent view among SIOs with regard to issues related to the social insurance system. The reasoning was as follows: the outcome of VR is a result of which clients are selected for VR rather than of what measures have been provided. Hence measures are secondary and adapted to the selection made. The question is thus whether the client has the potential to resume work or needs medical support for a pension examination. Consequently, the outcome of VR reflects the group of clients rather than the measures provided.
The above reasoning is supported by the present result. The local social insurance offices with the highest and lowest outcomes in rates of work resumption and disability pension, respectively, selected clients for VR from different case categories. The differences in characteristics were manifest primarily as duration of sick-listing. The offices whose clients had long sickness absence, including processing time for VR, and which used much detailed investigation as a VR measure, showed higher rates of disability pension grants as the outcome of completed VR. In a previous study, a majority of the rehabilitation clients who had received detailed investigation were unemployed and with the longest periods of sickness absence (10). These factors have turned out to be predictors of disability pension, while clients who have received job training to a great extent are clients with an employment and shorter periods of sick-leave; factors that in turn have been shown to be predictors of work resumption (9, 11, 12).
The SIOs’ responses to the inquiry may also indicate that, for example, clients motivated for work resumption and with an employer positive towards this, have a better chance of getting VR. This in itself implies a sorting of clients when the SIOs are able to affect the selection. According to a National Social Insurance Board report (13), sick-listed people are selected for VR with respect to various factors, such as the choice of available VR services, the client’s motivation and his or her own initiatives.
The importance of early initiation as a factor for successful VR is displayed in this study through the register data as well as through the opinions expressed by the SIOs. Their replies indicate that a possible cause of delay in VR may be lack of resources. The heavy workload of SIOs may create a backlog that makes it difficult to establish the desired early contact with the client. Early contact is also defined by the SIOs themselves as a critical factor in reducing sick-listing. Too heavy a workload in general is known to have various negative effects on the psychological working climate. Previous studies also indicate that VR measures are taken at a late stage of the process (10, 12, 14–20).
It seems natural that job training is the most frequent measure among major employers, since they have a responsibility to determine whether the person can remain in the organization with, perhaps, modified work tasks. Previous studies indicate that employment training or other active work practice is important for returning to work (17, 21, 22). The fact that detailed investigation and combined measures are frequent among unemployed people may be because this group have no existing employer to turn to for job training (10). This group may also require more thorough planning that includes several measures in order to establish a path back to working life.
A parliamentary committee has concluded that: “surveys of rehabilitation needs, e.g. investigations, take up a great and increasing proportion of the resources allocated for the purchase of VR measures.” (14). This is supported by the results of Ahlgren et al. (10), who found that approximately 75% of cases where clients had been investigated resulted in a pension grant. This could be the reason for the poor level of work resumption following investigation, the measure used for obtaining medical statements, when in reality there was never a real potential for return to work.
The greatest difference among the SIOs was found in the attitude towards “minor” ailments and the possibility of working despite these. Differences as to whether a given functional status does or does not imply reduced work capacity could create a risk that decisions regarding allowance may differ depending on which SIO is handling a case. A majority (87%) supported the view that getting sickness allowance granted is easy. This accords with a previous study in which 87% of patients had been granted sickness allowance even where a general practitioner would not recommend sick-listing (23).
Among factors that the SIOs held as important for giving a client priority for VR, the client’s motivation was mentioned by the majority. This is also raised as a success factor in other studies (15, 24). Clients who propose their own measures for VR have a better chance of getting VR (23). Findings in the same studies concerning factors spoiling the chances of getting VR, i.e. low motivation and old age, are also in line with those of the present study.
SIOs give their present work situation as an impediment to effective rehabilitation, particularly where they had a backlog causing delay. Another study (25) discusses the problem that such a low proportion of sick-listed people, only half those on sick-leave exceeding one year, have been in contact with the insurance office to discuss resuming work. The same type of problem appears in a National Social Insurance Board analysis (26), where long-term sick-listed people complained about the long wait for VR measures.
The employer’s attitude to the employee is raised by some SIOs as an essential factor for successful VR and work resumption. This is in line with previous studies that stress the importance of effective communication among those involved and of maintaining communication with workers recovering at home (27, 28). According to Heijbel et al. (29) close to 25% of clients on long-term absence did not feel welcome back to work. More activation of employers in the VR process is also indicated as an important factor by Gard & Söderberg (30).
The response to the question about co-operation was also very varied. One cause of the low opinion of co-operation was the difficulties in forwarding cases where the client has been assessed to be capable of work and consequently should be available on the labour market. This is also in line with previous findings, that lack of common goals and vision among different welfare agencies may impede the VR process (31, 32). If, on the other hand, VR measures were co-ordinated in a multiprofessional VR approach, the chances of returning to work may instead be enhanced (33, 34).
As only the diagnosis first stated as cause of the disability hindering working capacity (and thus the medical reason for sickness allowance) was recorded in the study, changes in diagnosis during sick-listing are not reflected. Thus other concomitant diseases may have existed or appeared. It cannot be excluded that various diagnoses may have affected the SIOs’ choices of VR measures or their selection for VR. Differences in this respect were identified by the municipal social insurance committee, regarding decisions to grant disability pensions to clients with psychiatric diagnoses/disorders; the SIOs saw those cases as most problematic (35). The present study data did not allow these aspects to be analysed.
The significant differences between the offices regarding rehabilitation outcome immediately after completed rehabilitation were not apparent at the 2-year follow-up. One reason for this could be internal changes between outcomes that occur within the respective offices, e.g. due to insufficient VR measures taken, and low stability as a result.
In conclusion, there are intra-county differences in the handling of sick-leavers who take part in VR measures. Differences in the process of selection of clients for VR between SIOs in different local offices lead to differences in work resumption. SIOs from different local insurance offices lacked conformity in attitudes towards the social insurance system and its clients. Although not demonstrated here, this diversity in attitude may be a factor underlying local differences in client selection and in the outcome of VR.
Acknowledgement
This study was supported by the Karolinska Institutet and by Mid Sweden University.
ReferenceS
1. SOU. En handlingsplan för ökad hälsa i arbetslivet. Slutbetänkande av utredningen om den arbetslivsinriktade rehabiliteringen. [An action plan for improved health in work life]. Report No.: SOU 2002:5. Stockholm: Socialdepartementet [Ministry of Health and Social Affairs]; 2002 (in Swedish).
2. SFS. Lag (1962: 381) om allmän försäkring, AFL. [Act on Public Social Insurance]. In: Socialdepartementet [Ministry of Health and Social Affairs]; 1962 (in Swedish).
3. Gerner U. Åter till arbete- hinder och möjligheter. En studie om motivationens betydelse i rehabiliteringsprocessen för långvarigt sjukskrivna. [Return to work – obstacles and prospects. A study of significance of motivation in the rehabilitation process for long-term sick leavers]. Stockholm: licentiate, Institutionen för socialt arbete, Stockholms universitet; 2002 (in Swedish, English summary).
4. Soderberg E, Alexanderson K. Gatekeepers in sickness insurance: a systematic review of the literature on practices of social insurance officers. Health Soc Care Community 2005; 13: 211–223.
5. Klanghed U, Svensson T, Alexandersson K. Positive encounters with rehabilitation professionals reported by persons with experience of sickness absence. Work 2004; 22: 247–254.
6. Ostlund G, Cedersund E, Alexanderson K, Hensing G. “It was really nice to have someone” – lay people with musculoskeletal disorders request supportive relationships in rehabilitation. Scand J Public Health 2001; 29: 285–291.
7. Falkdal AH, Edlund C, Dahlgren L. Experiences within the process of sick leave. Scand J Occup Ther 2006; 13: 170–182.
8. Ahlgren A, Bergroth A, Ekholm J. Work resumption or not after rehabilitation? A descriptive study from six social insurance offices. Int J Rehabil Res 2004; 27: 171–180.
9. Ahlgren A, Bergroth A, Ekholm J, Schüldt K. Work resumption after vocational rehabilitation: a follow-up two years after completed rehabilitation. Work 2007; 28: 343–354.
10. Ahlgren A, Broman L, Bergroth A, Ekholm J. Disability pension despite vocational rehabilitation? A study from six social insurance offices of a county. Work resumption or not after rehabilitation? A descriptive study from six social insurance offices. Int J Rehabil Res 2005; 28: 33–42.
11. Marnetoft S-U, Selander J. Multidisciplinary vocational rehabilitation focusing on work training and case management for unemployed sick-listed people. Int J Rehabil Res 2000; 23: 271–279.
12. Marnetoft SU, Selander J, Bergroth A, Ekholm J. Factors associated with successful vocational rehabilitation in a Swedish rural area. J Rehabil Med 2001; 33: 71–78.
13. RFV. Risk- frisk- faktorer. Sjukskrivning och rehabilitering i Sverige. [Risk – healthy – factors. Sicklisting and rehabilitation in Sweden]. RFV Redovisar, Report No.: 1997: 6. Stockholm: Riksförsäkringsverket [National Social Insurance Board]; 1997 (in Swedish, English summary).
14. SOU. Rehabilitering till arbete- en reform med individen i centrum. Slutbetänkande av utredningen om den arbetslivsinriktade rehabiliteringen. [Rehabilitation back to work- a reform with the individual in the centre]. Report No.: SOU 2000: 78. Stockholm: Socialdepartementet (Ministry of Health and Social Affaires); 2000 (in Swedish).
15. Haldorsen EM, Grasdal AL, Skouen JS, Risa AE, Kronholm K, Ursin H. Is there a right treatment for a particular patient group? Comparison of ordinary treatment, light multidisciplinary treatment, and extensive multidisciplinary treatment for long-term sick-listed employees with musculoskeletal pain. Pain 2002; 95: 49–63.
16. Anagnostes C, Mayer TG, Gatchel RJ. Effect of preinjury wage levels on socioeconomic outcomes of chronic disabled work-related spinal disorder patients. Spine J 2002; 2: 12–13.
17. Bendix AF, Bendix T, Haestrup C. Can it be predicted which patients with chronic low back pain should be offered tertiary rehabilitation in a functional restoration program? A search for demographic, socioeconomic, and physical predictors. Spine 1998; 23: 1775–1783; discussion 1783–1784.
18. Marhold C, Linton SJ, Melin L. A cognitive-behavioral return-to-work program: effects on pain patients with a history of long-term versus short-term sick leave. Pain 2001; 91: 155–163.
19. Marnetoft SU, Selander J, Bergroth A, Ekholm J. The unemployed sick-listed and their vocational rehabilitation. Int J Rehabil Res 1997; 20: 245–253.
20. Selander J, Marnetoft SU, Bergroth A, Ekholm J. The process of vocational rehabilitation for employed and unemployed people on sick-leave: employed people vs unemployed people in Stockholm compared with circumstances in rural Jamtland, Sweden. Scand J Rehabil Med 1998; 30: 55–60.
21. Carling K, Richardson K. The relative efficiency of labor market programs: Swedish experience from the 1990s. Labour Economics 2004; 11: 335.
22. Gerfin M, Lechner M, Steiger H. Does subsidised temporary employment get the unemployed back to work? An econometric analysis of two different schemes. Labour Economics 2005: 12: 807–835.
23. Englund L, Svardsudd K. Sick-listing habits among general practitioners in a Swedish county. Scand J Prim Health Care 2000; 18: 81–86.
24. Baril R, Clarke J, Friesen M, Stock S, Cole D. Management of return-to-work programs for workers with musculoskeletal disorders: a qualitative study in three Canadian provinces. Soc Sci Med 2003; 57: 2101–2114.
25. Eklund M, Lindwall U, Marklund S. Hur fungerar den arbetslivsinriktade rehabiliteringen? In: Marklund S, Bjurvald M, Hogstedt C, Palmer E, Theorell T, editors. Den höga sjukfrånvaron- problem och lösningar. [High numbers of sick-listing − problems and solutions]. Stockholm: Arbetslivsinstitutet; 2005, p. 269–301 (in Swedish, English summary).
26. RFV. Långtidssjukskrivnas uppfattning om rehabiliterande åtgärder och insatser. [Opinions of long term sick-listed about rehabilitation measures and efforts]. RFV Analyserar, Report No.: 2004: 8. Stockholm: Riksförsäkringsverket [National Social Insurance Board]; 2004 (in Swedish, English summary).
27. Friesen MN, Yassi A, Cooper J. Return-to-work: the importance of human interactions and organizational structures. Work 2001; 17: 11–22.
28. Sim J. Improving return-to-work strategies in the United States disability programs, with analysis of program practices in Germany and Sweden. Soc Secur Bull 1999; 62: 41–50.
29. Heijbel B, Josephson M, Jensen I, Vingard E. Employer, insurance, and health system response to long-term sick leave in the public sector: policy implications. J Occup Rehabil 2005; 15: 167–176.
30. Gard G, Söderberg S. How can a work rehabilitation process be improved? – a qualitative study from the perspective of social insurance officers. Disabil Rehabil 2004; 26: 299–305.
31. Edlund C, Dahlgren L. The physician’s role in the vocational rehabilitation process. Disabil Rehabil 2002; 24: 727–733.
32. Lindqvist R, Grape O. Vocational rehabilitation of the socially disadvantaged long-term sick: inter-organizational co-operation between welfare state agencies. Scand J Public Health 1999; 27: 5–10.
33. Jakobsson B, Bergroth A, Schuldt K, Ekholm J. Do systematic multiprofessional rehabilitation group meetings improve efficiency in vocational rehabilitation? Work 2005; 24: 279–290.
34. Van Lierop B, Nijhuis F. Assessment, education and placement: an integrated approach to vocational rehabilitation. Int J Rehabil Res 2000; 23: 261–269.
35. Edlund C. Långtidssjukskrivna och deras medaktörer – en studie om sjukskrivning och rehabilitering. [Long-term sick leavers and their co-actors –a study of sick listing and rehabilitation]. PhD Thesis. Department of Public Health and Clinical Medicine, Umeå, Sweden; 2001 (in Swedish, English summary).