OBJECTIVE: To assess the interaction of foot placement, trunk frontal position, weight-bearing and knee moment asymmetry at seat-off when rising from a chair.
DESIGN: Cross-sectional study.
SUBJECTS: Seventeen subjects with hemiparesis and 15 healthy controls.
METHODS: Trunk position, weight-bearing and knee moment asymmetry were quantified by kinetic and kinematic analysis when the subjects rose from a chair using 3 different foot placements: spontaneous, symmetrical and asymmetrical. Asymmetry was defined by the ratio between sides.
RESULTS: In the healthy controls, the spontaneous and symmetrical foot placements were associated with an almost vertical trunk position and a symmetrical weight-bearing and knee moment. The asymmetrical foot placement resulted in a trunk displacement towards the foot placed behind, with more weight-bearing and higher moment on this side. The opposite was observed in the hemiparetic participants where the spontaneous and symmetrical foot conditions determined a trunk position and an asymmetry bias towards the unaffected side. Placing the affected foot behind the other reduced the asymmetrical behaviour.
CONCLUSION: Changes in weight-bearing are partly associated with the frontal trunk position, and foot placement manipulations can be used to modify weight-bearing distribution. Inference on weight-bearing is possible by observing the trunk position during the sit-to-stand task in persons with hemiparesis.
Key words: rehabilitation, sit-to-stand, kinematic, kinetic, trunk, weight-bearing, asymmetry.
J Rehabil Med 2008; 40: 200–207
Correspondence address: Sylvie Nadeau, École de Réadaptation, Université de Montréal, C. P. 6128, Succursale Centre-ville, Montréal, Québec, Canada H3C 3J7. E-mail: sylvie.nadeau@umontreal.ca
Submitted May 14, 2007; accepted October 17, 2007
INTRODUCTION
The sit-to-stand (STS) task is an activity frequently performed in everyday life (1). The ability to rise from a chair is a prerequisite for independent locomotion and for many other functional activities of daily living (2). Determinants of the STS task have been described in a review by Janssen et al. (3). Transferring from a sitting to a standing position requires considerable effort by the lower limbs in healthy subjects, particularly at the knee and the hip (4, 5). This task can be difficult or impossible for individuals with hemiparesis following a stroke (6–8), and is recognized as a disabling condition.
According to the literature, individuals with hemiparesis present a weight-bearing asymmetry when they rise from a chair spontaneously, placing more weight on the unaffected lower limb than on the affected one (6, 9–12). They modify their motor strategies by making greater use of the knee extensors on the unaffected side (expressed by a greater net moment at the knee) (5). During the STS task, individuals with hemiparesis show lateral trunk movements towards the unaffected side, with a corresponding shift of the body’s centre of gravity (13) in the medio-lateral direction, which is greater than in the antero-posterior direction, unlike in healthy subjects (9). Since the head-arm-trunk (HAT) segment represents a large proportion of the body mass (≈ 70%), it might be hypothesized that the modifications in weight-bearing and moments are caused by a change in the trunk position in space during the STS task. According to this assumption, it is accepted that the trunk position is a good indicator of the global effect of the HAT segment.
The interpretation is more complex when the task is carried out with an asymmetrical foot placement rather than a symmetrical one. When healthy subjects rise from a chair with the asymmetrical foot placed in the antero-posterior direction, the body weight is mainly supported by the lower limb placed behind (14). In this condition, a trunk movement in the frontal plane towards the side of the posterior foot might be accompanied by a corresponding greater solicitation of the knee extensors on this side than in a symmetrical foot condition. However, this might not be the case in individuals with hemiparesis. According to Brunt et al. (14) and Roy et al. (12), the weight-bearing asymmetry for these participants can be reduced when the task is performed with the affected foot placed behind the unaffected foot. This foot placement seems to force the weight-bearing of the affected side and it might be interesting to know if the trunk positions and knee extensor moments also become symmetrical. To summarize, it is expected that the foot position will be associated with an opposite behaviour of the trunk movement in the frontal plane when individuals with hemiparesis are compared with healthy subjects.
So far, no study has systematically analysed the complex interactions between foot placement, trunk position in the frontal plane, weight-bearing and moment asymmetry. The first purpose of this study was to determine the role of foot position in inducing trunk position changes in the frontal plane (side flexion and medio-lateral translation) as well as weight-bearing and knee muscular moment asymmetry at seat-off during the STS task in healthy individuals and in persons with hemiparesis. The second purpose was to demonstrate, in each group of subjects, the association between trunk position, on the one hand, and weight-bearing and knee moment asymmetry on the other, irrespective of the foot position. The reason behind this approach is the possibility that, at the level of the individual subject, asymmetry may be present with symmetrical foot position and vice-versa.
METHODS
Participants
The study was carried out on 17 subjects with hemiparesis, 12 men and 5 women, age range 27–72 years, mean age 49.7 (standard deviation (SD) 11.3) years. Their mean (1 SD) height and weight were respectively 170.1 cm (SD 6.9) and 75.8 kg (SD 13.7). Twelve subjects presented a left-sided hemiparesis. Their mean time post-stroke was 3.2 (SD 2.3) years (range 11 months to 10.1 years). Patients were selected according to the following inclusion criteria: (i) more than 6 months post-stroke; (ii) able to stand up and sit down independently from a standard chair without using arms and hands and to tolerate 2 hours of testing with appropriate rest periods; (iii) to have a residual muscular weakness and motor impairment of the affected lower limb resulting in a score of less than 6 on the Chedoke McMaster Stroke Assessment (15). Individuals with cognitive impairments, cerebellar involvement, musculoskeletal and neurological disorders in addition to their stroke were excluded from this study. This information was gathered with the help of the clinical chart, the participants themselves or their proxy.
Fifteen healthy controls volunteered to participate in this study (7 males and 8 females). All participants except one were right-handed and had no recent history of back pain or disorders of the musculoskeletal system in the lower limbs. Their mean age was 56.1 (SD 10.9) years, age range 33–73 years. Their mean stature and body mass (1 SD) were 168.4 (SD 9.8) cm and 73.9 (SD 16.5) kg, respectively.
The hemiparetic and healthy participants took part in a clinical testing session, followed by a 2-h laboratory session assessment of the STS task. Each individual signed an informed consent in accordance with institutional guidelines before their participation in the project. This study, carried out in the pathokinesiology laboratory at the Research Centre of the Montreal Rehabilitation Institute, was approved by the ethics committee of the institute.
Clinical assessment
To quantify physical impairments and disability, the subjects with hemiparesis were evaluated with valid and reliable clinical evaluation tools by a physical therapist with experience in neurology. With regard to physical impairments, muscular tone at the ankle was evaluated by the Levin & Hui-Chan Spasticity Index (16), while global impairments were estimated by the Chedoke McMaster Stroke Assessment (lower-limb part) (15). To measure their physical disability, patients with hemiparesis were subjected to the Berg balance scale test (17) for balance and the walking speed test at natural and maximal speed over 5 m (18) for locomotor capacities. The walking speed test was also performed by the healthy subjects.
Laboratory assessment of the sit-to-stand task
Instrumentation. An instrumented chair developed in our laboratory, without back or armrests and equipped with force sensors, recorded the forces applied under each thigh (19). The seat level can be easily adjusted to heights ranging from 39 to 77 cm. The chair was fixed to the floor to dissipate any vibrations. Two AMTI (OR6-7-1000) force plates embedded in the floor were used to record the force under each foot. This platform set-up (floor and chair) allowed the orthogonal forces under the thighs and feet and the moments to be recorded throughout the duration of the tasks. The seat and ground reaction forces were collected at 600 Hz. Data were then filtered with a 4th-order Butterworth zero-lag filter with a cut-off frequency of 10 Hz and sampled at 60 Hz to match the kinematic data. During the STS task, the 3-dimensional position of infra-red markers was sampled at 60 Hz and recorded by an Optotrak 3020 system (Northern Digital Inc., Waterloo, Canada).
Segmental kinematic. Three non-collinear markers were placed on each segment of an 8-segment model (feet, legs, thighs, pelvis and trunk) (12). In addition, specific bony landmarks were digitized using a 6-marker probe to further define articular centres and principal axes of segments. Those landmarks were the mid-toe, the heel, the medial ankle, the medial femoral condyle, the anterior superior iliac spines, the iliac crests, the great trochanter and the glenohumeral joint (5). All marker trajectories were later inspected visually to identify missing marker co-ordinates and, when possible, their co-ordinates were interpolated using a linear or cubic spline method. The co-ordinates of the markers were finally smoothed with a 4th-order Butterworth zero-lag filter using a cut-off frequency of 6 Hz.
Anthropometric measurements must be acquired to calculate inertial properties of segments. The participant’s weight and the length and circumference of each segment were measured (5, 20). The circumference of each segment was measured proximally, distally and at the most prominent region between these previous measures. The mass of the foot, shank and thigh segments corresponded to 1.5%, 4.3% and 10.1% of the total body mass, respectively (20). The centre of mass of the foot, shank and thigh segments were located at 50.0%, 56.7% and 56.7% of the segment length relative to the distal axis, respectively (20). Moments of inertia were computed from the length, the diameter and the mass of the segment.
Sit-to-stand tasks. The subjects with hemiparesis and healthy controls sat on the instrumented chair, well centred and with one foot and one thigh on each ground and seat force plate. Keeping both arms crossed on the chest and looking forwards at a target placed at a height of 2 m on the wall 3 m in front of them, they had to stand up, keep the standing position for 4–5 seconds and then sit down. The task was performed at natural speed from the instrumented chair with the seat level adjusted to the length of the leg (distance from the lateral femoral condyle to the ground) using 3 different foot positions: (i) spontaneous (SP): no instructions given on the initial foot position; (ii) symmetrical (S): both feet placed at 15° of dorsiflexion; (iii) asymmetrical with the affected foot placed behind the unaffected foot (AS-A) for the hemiparetic subjects or with the dominant foot placed behind the non-dominant foot (AS-D) for the healthy subjects. For the third condition, the posterior part of the heel of the anterior foot was placed at 50% of the length of the posterior foot, which was dorsiflexed at 15°. The spontaneous condition was always executed first, whereas the other 2 foot positions were randomized. Two trials were performed for each foot placement, for a total of 6 trials. To standardize the position from one trial to another in a given condition, subjects were instructed to keep both heels in contact with the ground and not to move their feet between trials. A mark on the ground was used to ensure that subjects kept a constant foot position. A line marked at 50% of the thigh length (distance from the greater trochanter to the articular centre of the knee) was aligned with the anterior border of the seat to position the participants on the same location on the seat.
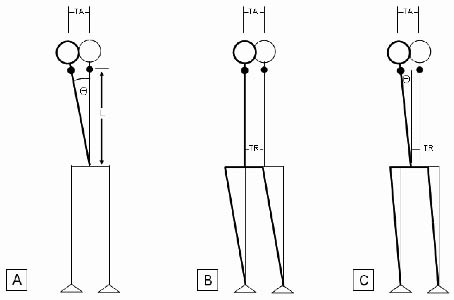
Data analysis and variables. The marker positions were filtered with a 4th-order Butterworth, zero-lag filter, with a cut-off frequency of 6 Hz. Using the analysis package from Mishac Inc. (Mishac Kinetics, Waterloo, Canada), the joint angles in the sagittal plane were calculated at the hip, knee and ankle joints. Trunk positions were quantified in the frontal plane only. Absolute side flexion (°) corresponds to the angle Θ between the trunk longitudinal axis projected in the frontal plane (L) and the vertical axis (Fig. 1A). The longitudinal axis is a line joining the middle of the pelvis segment to the neck centre. Markers attached at the level of the processus spinosus of the seventh cervical vertebra (C7) and the posterior superior iliac spines (PSIS) were used to determine the longitudinal axis of the trunk. Absolute translation (TA) is defined by the lateral displacement (cm) of the neck joint centre relative to the origin of the laboratory system (Fig. 1B), while the relative translation (TR; Fig. 1C) is obtained after correcting for the side flexion according to the formula TR = TA – L sin Θ. The relative translation is related to the side sliding of the pelvis and lower limbs by frontal rotation around each ankle (Fig. 1B).
Fig. 1. The same absolute trunk translation (TA) can be obtained by: (A) a side flexion equivalent to L sin Θ, Θ is the angle between the trunk longitudinal axis projected in the frontal plane (L) and the vertical axis. (B) a relative trunk translation (TR) and (C) a combination of (A) and (B) corresponding to TA = TR + L sin Θ. In this figure, the y-axis of the laboratory was placed to correspond to a sagittal plane dividing the body into right and left segments.
The weight-bearing asymmetry (WBASYM) estimated from the vertical reaction forces (VRFs) between both sides was computed at seat-off as:
WBASYM = VRF non-dominant side (or affected side)
VRF dominant side (or unaffected side)
Perfect symmetry corresponded to equal VRF on each foot (WBASYM = 1).
The net joint moments at the knee were estimated using an inverse dynamic approach (20) performed with Kingait 3 Software (Mishac Kinetics, Waterloo, Canada). Knee moment asymmetry (KMASYM) was also calculated at seat-off and expressed by the ratio:
KMASYM = Knee moment non-dominant side (or affected side)
Knee moment dominant side (or unaffected side)
These 5 parameters (Θ angle, TA, TR, WBASYM and KMASYM) were analysed for a specific event during the STS task, namely seat-off when the participant was just leaving the chair. The time of occurrence of this event was determined by observing the seat vertical forces on the unaffected side or dominant side. These time values were used in a subsequent program to determine the corresponding value for each variable on the affected and unaffected sides.
Two other events were used in reference for calculating the STS execution time: (i) beginning of the STS task: any first perceptible change in the vertical ground reaction forces, which often corresponded to an initial reduction of the forces under the feet; and (ii) end of the STS task: moment when the movement at the hip becomes stabilized or the beginning of stable extension at the hip during the standing position.
Statistical analyses
Statistical analyses were performed using SPSS® software Windows (Version 13). Descriptive statistics (mean (1 SD)) were calculated to quantify the clinical evaluation, the trunk translation and side flexion, the weight-bearing asymmetry and the knee moment asymmetry and for all foot conditions at seat-off. A two-way repeated measures ANOVA (foot position and group of subjects) tested the effect of the foot position on each of the following variables (trunk translation and trunk side flexion, WBASYM, KMASYM) for the hemiparetic and healthy groups at the same time. If complex interactions occurred between the 3 foot conditions and the 2 groups, simpler analyses were performed. The first was a one-way repeated measures ANOVA to verify whether the 3 foot conditions were similar within each group. If the ANOVA resulted in any significant value (p < 0.05), pair-wise comparisons were made to identify the differences using a Bonferroni correction (0.05/3 conditions = 0.0167). The second was an independent t-test (one for each foot position) to determine whether each condition was similar between hemiparetic and healthy groups. The significant value was p < 0.0167 (0.05/3).
Pearson correlation coefficients (r) were used to assess the relationship between: (i) the trunk position (translation and side flexion) and the WBASYM and (ii) the trunk position and the KMASYM. A multiple linear regression analysis was also used to determine whether one or both the trunk translation and lateral flexion were associated with the WBASYM and the KMASYM. A stepwise method with variables entered in the model at a significance level of p ≤ 0.15 and removed from it at p ≥ 0.2 was used.
RESULTS
Clinical assessment
Some characteristics of the subjects with hemiparesis and the healthy controls are presented in Table I. Individuals with hemiparesis presented a mild spasticity at the ankle with a mean score of 6.7 (3.8) (range 3–16/16). They had residual motor impairment of the lower limb with a score on the Chedoke McMaster Stroke Assessment scale ranging from 3/7 to 6/7 for the leg (4.7/7 ± 1.1) and 2/7 to 7/7 for the foot (4/7 (SD 1.5)). The results on the Berg Scale varied from 37/56 to 56/56, indicating a balance from moderate to perfect (51.1 (SD 5.5)). Three subjects with hemiparesis wore an ankle-foot orthosis (AFO) during the STS task. When the 15° of dorsiflexion was limited by the AFO, the closest tolerable angle was used and kept constant across trials.
| Table I. Characteristics of the subjects with hemiparesis and healthy controls (mean (1 SD)) and range) |
| Clinical variables | Subjects with hemiparesis (n = 17) | Healthy subjects (n = 15) |
| Chedoke McMaster Stroke Assessment scale: leg | 4.7/7 (1.1) 3–6/7 | |
| Chedoke McMaster Stroke Assessment scale: foot | 4/7 (1.5) 2–7/7 | |
| Sit-to-stand duration (sec) (spontaneous foot condition) | 2.61 (0.72) (1.78–4.86) | 2.11 (0.39) (1.56–2.85) |
| 5-min walk test: self-selected speed (m/sec) | 0.84 (0.26) (0.27–1.28) | 1.36 (0.19) (1.03–1.63) |
| SD: standard deviation. |
Effects of foot position
Table II shows that the 3 foot conditions during the STS task resulted in a variation of the mean values from one condition to another for each parameter: WBASYM, KMASYM, absolute and relative lateral trunk translation as well as trunk side flexion (Fig. 2).
| Table II. Descriptive variables for subjects with hemiparesis (HS) and healthy controls (HC) (mean (1 SD)) at seat-off during the sit-to-stand task |
| Group | Parameters | Foot placement |
| Spontaneous (SP) | Symmetrical (S) | Asymmetrical* (AS-D or AS-A) |
| HC | WBASYM | 1.00 (0.12) | 0.95 (0.14) | 0.74 (0.21) |
| KMASYM | 0.98 (0.24) | 0.89 (0.21) | 0.82 (0.28) |
| Absolute trunk translation (cm) | 1.8 (2.6) | 2.2 (1.9) | 4.9 (2.5) |
| Relative trunk translation (cm) | 1.2 (2.6) | 1.5 (2.2) | 2.4 (2.0) |
| Trunk side flexion (°) | 2.4 (2.7) | 3.2 (2.7) | 8.2 (3.7) |
| HS | WBASYM | 0.67 (0.26) | 0.66 (0.24) | 0.87 (0.32) |
| KMASYM | 0.46 (0.39) | 0.46 (0.32) | 0.93 (0.58) |
| Absolute trunk translation (cm) | 6.1 (3.7) | 5.6 (4.1) | 2.6 (3.9) |
| Relative trunk translation (cm) | 2.1 (4.2) | 2.6 (4.6) | 2.4 (5.1) |
| Trunk side flexion (°) | 12.1 (6.1) | 11.0 (6.5) | 6.2 (5.8) |
| *for dominant or unaffected foot. WBASYM: weight-bearing asymmetry; KMASYM: knee moment asymmetry; SD: standard deviation. |
First, the two-way repeated measures ANOVA performed on each parameter revealed a significant interaction effect between the foot conditions and groups for the WBASYM (F(2,48) = 27.82, p < 0.001), the KMASYM (F(2,56) = 56.80, p < 0.001), the absolute trunk translation (F(2,56) = 22.38, p < 0.001) and the trunk side flexion (F(2,56) = 28.66, p < 0.001). These interactions indicated that the foot conditions had a different effect on asymmetry and trunk position for the 2 groups. In view of these interactions, the foot condition difference was evaluated with a one-way repeated measures ANOVA for each group separately, while group differences were analysed by t-test.
Trunk position. The absolute lateral trunk translation and the side flexion were influenced by the foot position in healthy ((F(2,28) = 15.85, p < 0.001) and (F(2,28) = 33.70, p < 0.001), respectively) and in hemiparetic individuals ((F(2,28) = 8.66, p = 0.001) and (F(2,28) = 8.81, p = 0.001), respectively). For the healthy subjects, the STS task performed with the AS-D condition showed a greater absolute trunk translation movement than the SP (p = 0.002) and S conditions (p = 0.001) (Fig. 2B). The side flexion angle was also greater in the AS-D conditions than in the SP (p < 0.001) and S conditions (p < 0.001). On the other hand, the results for the subjects with hemiparesis indicated a smaller trunk movement (absolute translation and side flexion) when they stand up with the paretic foot behind (AS-A) compared with the SP (translation: p = 0.003, side flexion: p = 0.002) and S conditions (translation: p = 0.014, side flexion: p = 0.008) (Fig. 2B). The relative trunk translation component revealed no interaction between foot conditions and groups (p = 0.200) nor a main effect of the foot conditions (p = 0.08) and groups (p = 0.58).
Weight-bearing asymmetry. The weight-bearing asymmetry was modified by the foot position for the healthy (F(2,28) = 16.50, p < 0.001) and hemiparetic group (F(2,20) = 17.70, p < 0.001). Healthy subjects presented almost equal loading on both lower limbs in the SP (1.0 (SD 0.12)) and S (0.95 (SD 0.14)) conditions, whereas the asymmetry increased with the asymmetrical (AS-D) foot placement (0.74 (SD 0.21)) (Fig. 2A). Pairwise comparisons identified a significant difference between the SP and AS-D conditions (p = 0.003) and between the symmetrical and AS-D conditions (p = 0.005).
In subjects with hemiparesis, high asymmetry (0.67–0.87) in the vertical reaction forces between the affected and unaffected sides were found in the 3 foot positions, but the difference was less marked in the AS-A condition, resulting in a better distribution of loading and a reduced asymmetrical pattern (Fig. 2A). The statistical analyses revealed significant differences between the SP and AS-A conditions (p = 0.001) and between the S and AS-A (p = 0.004).Knee moment asymmetry. For the KMASYM variable, the results were in the same direction as for the WBASYM, revealing a significant effect of the foot conditions in both groups. In the healthy controls, the ratio of asymmetry of the AS-D condition was significantly higher (p < 0.001) than those from the SP and S conditions, while the reverse was true for the hemiparetic subjects. In this group, KMASYM in the AS-A was significantly lower than in the SP (p = 0.011) and S conditions (p = 0.002).
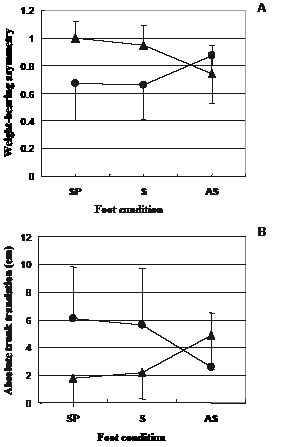
Fig. 2. (A) Weight-bearing asymmetry (WBASYM) and (B) absolute trunk translation for the 3 different foot conditions in subjects with hemiparesis () and healthy controls () at seat-off. SP: spontaneous; S: symmetrical; AS: asymmetrical.
Comparisons between subjects with hemiparesis and healthy controls for each foot condition
The mean values of main variables for each foot condition are presented in Table II. The subjects with hemiparesis presented a significantly higher WBASYM than healthy controls for the spontaneous (paired t-test, p < 0.001) and symmetrical (p < 0.001) foot positions. For these 2 foot conditions, the subjects with hemiparesis also showed a greater KMASYM than the healthy subjects (p < 0.001). Persons with hemiparesis had a greater absolute trunk translation and trunk side flexion to rise from a chair with the spontaneous (p = 0.001 and p < 0.001, respectively) and symmetrical (p = 0.005 and p < 0.001, respectively) foot conditions compared with the control group. However, for the asymmetrical condition, the hemiparetic subjects presented WBASYM, KMASYM, absolute translation and side flexion values that are not significantly different from those of the healthy controls (p > 0.0167). Finally, as indicated above, there is no difference in the relative trunk translation between the subjects with hemiparesis and the healthy controls in any of the foot conditions.
Correlations between asymmetry and trunk position
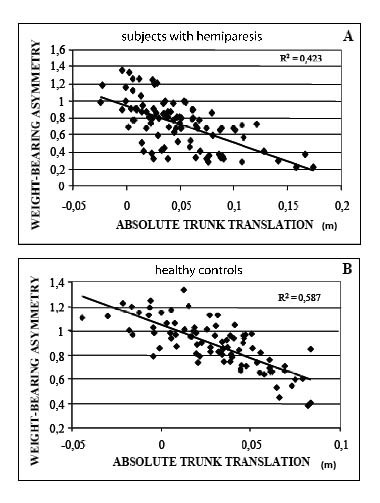
The results in Table II revealed that in both groups the most important trunk movements were observed in foot conditions showing the greatest WBASYM and KMASYM. For both groups, negative associations were found between these parameters, but the values of the coefficients are higher for the WBASYM than for the KMASYM. The associations between absolute trunk translation and the WBASYM were good in both subjects with hemiparesis (r = –0.651) and healthy controls (r = –0.766), whereas they were less so for relative trunk translation in the subjects with hemiparesis (r = –0.422) and healthy controls (r = –0.496). Good relationships were also identified between the WBASYM and the side flexion angle in the healthy controls (r = –0.675), but not in the hemiparetic subjects (r = –0.343). No correlation was found between the trunk position and the KMASYM except for the absolute trunk translation in healthy controls (r = –0.312). The scatter plots showing the associations between WBASYM and absolute trunk translation in healthy and hemiparetic subjects are presented in Fig. 3.
Fig. 3. Scatter plots showing the associations between weight-bearing asymmetry (WBASYM) and absolute trunk translation in (A) subjects with hemiparesis and (B) healthy controls at seat-off.
Multiple regression analysis
Multiple linear regression analysis was used to identify the most important variables associated with the WBASYM and KMASYM in subjects with hemiparesis and healthy controls (Table III). The results in healthy controls revealed that the trunk side flexion was the most important factor determining the WBASYM and KMASYM, accounting for 46% of the variance in the data (R2). When the relative trunk translation was added to the model for the WBASYM, the value increased to 54%. For the subjects with hemiparesis, both the relative trunk translation and the trunk side flexion were predictors of the WBASYM. The relative trunk translation explained 18% of the variance in the data. This value increased to 29% when the trunk side flexion was added to the model. The KMASYM variance was explained marginally (3%) by the trunk side flexion in healthy controls and by no variable in persons with hemiparesis.
| Table III. Results of the multiple regression analyses in subjects with hemiparesis (HS) and healthy controls (HC) |
| Group | Dependent variable | Independent variables in the model | F | R2 | p |
| HC | WBASYM | Θ | 68.643 | 0.456 | < 0.001 |
| Θ + TR | 48.139 | 0.543 | < 0.001 |
| KMASYM | Θ | 2.755 | 0.032 | 0.101 |
| HS | WBASYM | TR | 20.157 | 0.178 | < 0.001 |
| TR + Θ | 19.194 | 0.294 | < 0.001 |
| Θ: trunk side flexion; TR: relative trunk translation; WBASYM: weight-bearing asymmetry; KMASYM: knee moment asymmetry. |
DISCUSSION
The first objective of this study was to assess the interaction between foot placement, trunk positions in the frontal plane (side flexion and medio-lateral translation), weight-bearing and knee muscular moment asymmetry at seat-off when rising from a chair in subjects with hemiparesis and healthy controls. The second objective was to determine the level of association between trunk position and the asymmetry of weight-bearing and knee muscular moment. The effect of foot placement will be discussed first, followed by the analysis of the association between kinematic and kinetic variables.
Effects of foot position
The foot condition influenced the absolute trunk translation and trunk side flexion as well as the weight-bearing and moment asymmetry. With the spontaneous and symmetrical foot placement, healthy controls generally kept the trunk near the neutral position with minimal asymmetry, as revealed by the WBASYM and KMASYM indices near 1. It should be noted that asymmetry may exist, however, for a particular subject, as revealed by the SD of the variables. The generally symmetrical loading was already reported for normal subjects (6, 14, 21). Unlike the healthy controls, the subjects with hemiparesis moved the trunk toward the unaffected side when they rose from a chair spontaneously and symmetrically. These results confirmed those found by Hesse et al. (13), who calculated a lateral displacement of the body’s centre of gravity towards the unaffected side using double integration of force-plate data. More recently, Mazzà, et al. (22) indicated that side flexion toward the unaffected side occurred in subjects with hemiparesis and was correlated with lower-limb impairment. The unequal weight distribution observed in the subjects with hemiparesis confirmed results of previous studies (e.g. 6, 12, 13) and was probably related to the weakness (5, 23) and lack of motor control on the affected side.
When the task was performed with the asymmetrical foot placement, opposite results were observed in the 2 groups. The healthy controls showed a trunk displacement toward the dominant lower extremity, which was placed behind, with higher weight-bearing and moment being observed on this side. This asymmetrical pattern could be explained by the fact that the centre of mass must be displaced progressively in the anterior direction during the execution of the STS task. Thus, the projection of the centre of mass begins on the posterior foot and moves forward between the 2 feet by the end of the STS task. Consequently, at the time of seat-off, more weight is borne by the posterior foot with higher knee muscle involvement. Our observations are in line with the force-plate and electromyographic results of Brunt et al. (14). As supported by the correlation analysis (see discussion below), it appears that the trunk displacement is the factor responsible for the asymmetrical weight-bearing.
In the hemiparetic subjects, the asymmetrical foot placement was paradoxically associated with a more vertical trunk positioning and less asymmetry in weight-bearing and knee moment than in the other foot conditions. Thus, the hemiparetic subjects probably have to deal with 2 opposite elements: (i) the biomechanical obligation to project the centre of mass on the posterior foot (affected lower extremity) like healthy subjects in order to initiate the STS task; and (ii) the natural tendency to put more weight on the unaffected side. The net result is a compromise in terms of trunk positioning, WBASYM and KMASYM relative to the normal subjects. The large SD of the kinematic variables with the asymmetrical foot placement is probably an indicator of this difficult compromise.
The analysis performed on the relative trunk translation component revealed no interaction between foot conditions and groups and also no main effect of the foot conditions. As revealed by the data in Table II, very low values were obtained in all foot conditions. These low values were expected because the lateral shift of the pelvis, necessary for the relative translation (Fig. 1) cannot occur before seat-off, contrary to the side flexion.
The results of the comparison of the 2 groups show that subjects with hemiparesis use different motor strategies from those of healthy controls. Obviously, the former always distribute their weight-bearing towards the unaffected side, even when forced to put weight on the affected side, as in the asymmetrical foot condition. In this last condition, the asymmetry was, on average, less than in healthy controls. However, because of the large inter-subject variation, particularly in the hemiparetic group, statistical analysis failed to demonstrate a significant difference.
Associations between trunk position and asymmetry
Analysis of the effect of the foot placement strongly suggests that the weight-bearing and knee moment asymmetry could be explained in part by the position of the trunk in the frontal plane. In both groups, the greatest trunk position asymmetry was observed in foot conditions with the highest WBASYM and KMASYM ratio. One consequence of this observation should be the presence of correlations between trunk position asymmetry, on the one hand and weight-bearing and knee moment asymmetry on the other hand.
The results confirmed moderate associations between the WBASYM and the absolute trunk translation for both groups, whereas correlations were weaker for the relative trunk translation and side flexion angle. Considering that absolute trunk translation is determined by the relative trunk translation and the trunk side flexion, this result was predictable since subjects could reach displacement of the centre of mass either by a relative translation or a side flexion or by a combination of the 2. Because significant correlations were also found with relative translation and side flexion, a combination of both mechanisms is the most probable strategy. To address this issue, multiple regression analyses were performed to determine the contribution of these components to the WBASYM.
In the healthy subjects, the trunk side flexion accounted for 46% of the variance in the WBASYM and, when the relative trunk translation was added in the model, this value increased to 54%. In the hemiparetic subjects, the opposite was observed. In this group, the first factor selected in the model was the relative trunk translation, explaining 18% of the variance, while the second was the trunk side flexion (the value increased to 29%). The reason why side flexion is so important in determining the asymmetry of weight-bearing in healthy subjects is probably related to the fact that the displacement of the centre of mass occurs before seat-off as an anticipatory motor strategy. At this time, relative translation is impossible because the pelvis is in contact with the chair. The displacement of the trunk toward the non-affected side in subjects with hemiparesis before seat-off was also reported by Hesse et al. (13) and Mazzà et al. (22).
No significant correlation was found between the KMASYM and the trunk position except for the absolute trunk translation in healthy controls with a weak correlation of –0.312. This appears to contradict the finding about the effect of foot placement on KMASYM. This discrepancy should take into consideration the objectives of the statistical procedures used in the analysis. Repeated measures ANOVA on foot conditions is essentially an intra-individual comparison, while the correlation procedure establishes the association between variables and includes both intra- and inter-individual variations across all conditions. In the correlation analysis, all trials were included without considering the foot conditions because the aim was to associate the asymmetry of moment with the asymmetry in trunk position and one can imagine that, in the spontaneous and even in the symmetrical foot conditions, some asymmetry could be present. The lack of correlation indicates that the structured variation across foot conditions is lower than the random variation across subjects and no comparison is possible between subjects. Even if we tried to control the lateral foot placement, the analysis of the lateral foot marker position revealed a mean lateral change of 3 cm between the spontaneous and asymmetrical foot conditions. The width of the base of support on which the subject had to rely when leaving the chair might have influenced the data, particularly the trunk movements in the frontal plane. Moreover, the knee moments are dependent on other factors, such as the position and the orientation of the global force reaction vector under each foot.
This study has shown that foot placement affects WBASYM and KMASYM at seat-off during the STS task. For the hemiparetic subjects, the results indicate that clinicians should place the affected foot behind the non-affected one to constraint the use of the affected side, as already mentioned by Roy et al. (12) and Brunt et al. (14). In the case of symmetrical foot placement, the therapist could also manipulate the WBASYM in subjects with hemiparesis by giving instructions about the trunk movement to be performed. Finally, because WBASYM is partly determined by the trunk position, clinicians might be able to infer the weight-bearing by observing the trunk movements in the frontal plane during the STS task.
ACKNOWLEDGEMENTS
This study was presented in part at the REPAR Congress, Québec (Québec), Canada (May 2005) and at the 14th Biennial Conference of the Canadian Society for Biomechanics, Waterloo (Ontario), Canada (August 2006).
Julie Lecours was supported by a MSc scholarship from the Fonds de la recherche en santé du Québec (FRSQ) and l’Ordre professionnel de la physiothérapie du Québec (OPPQ). Dr Sylvie Nadeau is a junior II scientist supported by the FRSQ. The project was financed by the REPAR and the CHIR. We thank Pierre Desjardins and Michel Goyette for their technical support.
REFERENCES
1. Khemlani MM, Carr JH, Crosbie WJ. Muscle synergies and joint linkages in sit-to-stand under two initial foot positions. Clin Biomech 1999; 14: 236–246.
2. Shepherd RB, Koh HP. Some biomechanical consequences of varying foot placement in sit-to-stand in young women. Scand J Rehabil Med 1996; 28: 79–88.
3. Janssen WG, Bussmann HB, Stam HJ. Determinants of the sit-to-stand movement. A review. Phys Ther 2002; 82: 866–879.
4. Roebroeck ME, Doorenbosch CAM, Harlaar J, Jacobs R, Lankhorst G. Biomechanics and muscular activity during sit-to-stand transfer. Clin Biomech 1994; 9: 235–244.
5. Roy G, Nadeau S, Gravel D, Piotte F, Malouin F, McFadyen BJ. Side difference in the hip and knee joint moments during sit-to-stand and stand-to-sit tasks in individuals with hemiparesis. Clin Biomech 2007; 22: 795–804.
6. Engardt M, Olsson E. Body weight-bearing while rising and sitting down in patients with stroke. Scand J Rehabil Med 1992; 24: 67–74.
7. Kotake T, Dohi N, Kajiwara T, Sumi N, Koyama Y, Miura T. An analysis of sit-to-stand movements. Arch Phys Med Rehabil 1993; 74: 1095–1099.
8. Vander Linden DW, Brunt D, McCulloch MU. Variant and invariant characteristics of the sit-to-stand task in healthy elderly adults. Arch Phys Med Rehabil 1994; 75: 653–660.
9. Cheng PT, Liaw MY, Wong MK, Tang FT, Lee MY, Lin PS. The sit-to-stand movement in stroke patients and its correlation with falling. Arch Phys Med Rehabil 1998; 79: 1043–1046.
10. Chou SW, Wong AM, Leong CP, Hong WS, Tang FT, Lin TH. Postural control during sit-to stand and gait in stroke patients. Am J Phys Med Rehabil 2003; 82: 42–47.
11. Engardt M. Rising and sitting down in stroke patients: auditory feedback and dynamic strength training to enhance symmetrical body weight distribution. Scand J Rehabil Med 1994; Suppl 31: S1–S57.
12. Roy G, Nadeau S, Gravel D, Malouin F, McFadyen BJ, Piotte F. The effect of foot position and chair height on the asymmetry of vertical forces during sit-to-stand and stand-to-sit tasks in individuals with hemiparesis. Clin Biomech 2006; 21: 585–593.
13. Hesse S, Schauer M, Malezic M, Jahnke M, Mauritz KH. Quantitative analysis of rising from a chair in healthy and hemiparetic subjects. Scand J Rehabil Med 1994; 26: 161–166.
14. Brunt D, Greenberg B, Wankadia S, Trimble MA, Shechtman O. The effect of foot placement on sit to stand in healthy young subjects and patients with hemiplegia. Arch Phys Med Rehabil 2002; 83: 924–929.
15. Gowland C, Stratford P, Ward M, Moreland J, Torresin W, Van Hullenaar S, et al. Measuring physical impairment and disability with the Chedoke-Mcmaster stroke assessment. Stroke 1993; 24: 58–63.
16. Levin MF, Hui-Chan CW. Relief of hemiparetic spasticity by tens is associated with improvement in reflex and voluntary motor functions. Electroencephalogr Clin Neurophysiol 1992; 85: 131–142.
17. Berg KO, Wood-Dauphinee SL, Williams JI, Maki B. Measuring balance in the elderly: validation of an instrument. Can J Public Health 1992; 83 Suppl 2: S7–S11.
18. Salbach NM, Mayo NE, Higgins J, Ahmed S, Finch LE, Richards CL. Responsiveness and predictability of gait speed and other disability measures in acute stroke. Arch Phys Med Rehabil 2001; 82: 1204–1212.
19. Desjardins P, Nadeau S, Gravel D, Roy G, editors. A chair with a platform setup to measure the forces under each thigh when seated, rising from a chair and sitting down. Halifax, Nova Scotia: Canadian Society for Biomechanics; August 2004, p. 32.
20. Winter DA, editor. The biomechanics and motor control of human gait: normal, elderly and pathological, 2nd edn. Waterloo: University of Waterloo Press; 1991, p. 75–85.
21. Hirschfeld H, Thorsteinsdottir M, Olsson E. Coordinated ground forces exerted by buttocks and feet are adequately programmed for weight transfer during sit-to-stand. J Neurophysiol 1999; 82: 3021–3029.
22. Mazzà C, Stanhope SJ, Taviani A, Cappozzo A. Biomechanic modeling of sit-to-stand to upright posture for mobility assessment of persons with chronic stroke. Arch Phys Med Rehabil 2006; 87: 635–641.
23. Lomaglio MJ, Eng JJ. Muscle strength and weight-bearing symmetry relate to sit-to-stand performance in individuals with stroke. Gait Posture 2005; 22: 126–131.
24. Crosbie J, Herbert RD, Bridson JT. Intersegmental dynamics of standing from sitting. Clin Biomech 1997; 12: 227–235.