There is a need to develop a contemporary and internationally accepted conceptual description of physical and rehabilitation medicine (PRM). The process of evolving such a definition can now rely on the unifying conceptual model and taxonomy of the International Classification of Functioning, Disability and Health (ICF) and an ICF- based conceptual description of rehabilitation understood as a health strategy. The PRM section of the European Union of Medical Specialists (UEMS) has endorsed the application of the ICF as a unifying conceptual model for PRM and supports the process of moving towards an “ICF-based conceptual description and according definitions of PRM”. With this goal in mind, the authors have developed a first tentative conceptual description in co-operation with the professional practice committee of the UEMS-PRM-section. A respective brief definition describes PRM as the medical specialty that, based on the assessment of functioning and including the diagnosis and treatment of health conditions, performs, applies and co-ordinates biomedical and engineering and a wide range of other interventions with the goal of optimizing functioning of people experiencing or likely to experience disability. Readers of the Journal of Rehabilitation Medicine are invited to contribute to the process of achieving an internationally accepted ICF-based conceptual description of PRM by submitting commentaries to the Editor of this journal.
Key words: rehabilitation medicine, ICF, physical medicine.
J Rehabil Med 2007; 39: 286–292
Correspondence address: Gerold Stucki, Department of Physical Medicine and Rehabilitation, University Hospital Munich, Marchioninistrasse 15, DE-81377 Munich, Germany. E-mail: gerold.stucki@med.uni-muenchen.de
Submitted May 4, 2005; accepted October 13, 2006
INTRODUCTION
A unifying scientific framework is of utmost importance for any professional, academic and scientific discipline. It provides a conceptual link between disparate parts that might appear superficially to lack an intellectual relationship. Thus, it ensures communication and exchange among practitioners and scientists. To be able to rely on a common framework seems to be of even more importance for a professional discipline such as physical and rehabilitation medicine (PRM) that is not defined by a disease or an organ system. Instead, PRM is concerned with limitations of functioning and disability associated with health conditions and with the complex interaction with personal factors and the environment. As a result of this complexity, it is a highly interdisciplinary area, in both research and practice.
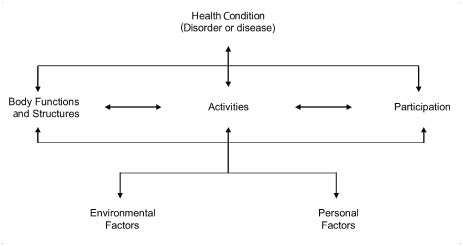
PRM applies rehabilitation as its core strategy (1). The basis for the definition of rehabilitation understood as a health strategy is the World Health Organization’s (WHO) International Classification of Functioning, Disability and Health (ICF) (1, 2) (Fig. 1). According to the ICF, human functioning includes the components body functions and structures, and activities and participation. Human functioning and its complementary notion disability are understood as experiences of people in the context of their personal resources, in relation to health conditions and in interaction with the environment (1, 3). Based on the ICF, rehabilitation can be defined as the health strategy that “aims to enable people with health conditions experiencing or likely to experience disability to achieve optimal functioning in interaction with the environment” (1).
Fig. 1. Interaction between the components of the International Classification of Functioning, Disability and Health (ICF) (2).
This definition of rehabilitation can serve as reference for conceptual descriptions and definitions of professional disciplines such as the medical specialty PRM, the rehabilitation professions, and distinct scientific fields of human functioning and rehabilitation research (4, 5). It may thus be possible to develop a commonly accepted definition of PRM that replaces the widely varying current definitions.
The objective of this paper therefore is to explore how the ICF and an ICF-based conceptual description of rehabilitation understood as a health strategy (1) can serve as basis for the conceptual description and according definitions of the medical specialty PRM. The specific aims are: (i) to develop an ICF-based conceptual description of PRM; and (ii) to provide examples of according comprehensive and brief definitions of PRM.
DEVELOPMENT PROCESS
The conceptual descriptions have been developed by the authors in an iterative discussion process with the professional practice committee of the European Union of Medical Specialists (UEMS)-PRM-section and colleagues acknowledged below. While these colleagues deserve credit for their comments and suggestions, the authors take full responsibility for the text and the ICF-based conceptual description presented here.
The UEMS-PRM-section endorsed the application of the ICF as a unifying conceptual model for PRM on 1 April 2006 in Lausanne, Switzerland. It also decided to promote the application of the ICF as a unifying conceptual model for PRM by supporting the process towards “ICF-based conceptual descriptions and according definitions of the rehabilitation strategy and PRM” within the next 2 years. The conceptual description presented in this paper serves as a starting point for this process. It is important to note that the definitions are tentative and have not been formally approved by the UEMS-PRM-section. They are intended to open the discussion towards an internationally accepted conceptual description and according definitions.
THE ICF AS UNIFYING FRAMEWORK FOR PRM
The ICF can be seen as the new unifying model for PRM (3, 6–10). PRM has been among the first to recognize the potential of the ICF to develop rehabilitation care further, to inform health policy and management better, and to stimulate research with the common goal of optimizing functioning and minimizing disability from both the individual and the public health perspective (3, 6, 7). Accordingly, PRM has also been proactive in the development of practical tools such as the ICF Core Sets to overcome challenges in applying the ICF in clinical practice and research (6, 7, 10–13).
The multi-sectorial perspective of the ICF is in agreement with the position of PRM in society. PRM is clearly rooted in the health sector, since, as a medical specialty, it is committed to improve functioning and health of people with a health condition. However, while PRM focuses on health interventions, it also integrates labor, educational, social, architectural and engineering approaches through co-operation with organizations and professionals across sectors. Beyond medical rehabilitation, PRM specialists may be involved in vocational rehabilitation or community integration.
In this respect, discussion about the name of the specialty is telling. The roots of the professional specialty in medicine and hence within the health sector are made more explicit with the new recently internationally adopted name of the specialty “Physical and Rehabilitation Medicine” (PRM), compared with the previous name “Physical Medicine and Rehabilitation” (PMR). While the term “rehabilitation” refers to a multi- sectorial and multi-professional strategy that may be applied by professional disciplines within the health sector and across sectors (1), the term “rehabilitation medicine” refers to the specific approach of a medical specialty engaging in rehabilitation. The term makes the basis of PRM within medicine and the health sector explicit.
Within medicine and the health sector, the term “rehabilitation medicine” differentiates the medical specialty PRM from other health professions involved in rehabilitation, including those designated rehabilitation professions, e.g. physiotherapy and occupational therapy.
ICF-BASED CONCEPTUAL DESCRIPTION OF PRM
There is no single appropriate ICF-based definition of PRM. Also, depending on the purpose one may, for example, wish to use a comprehensive or a brief definition. In order to facilitate purpose-tailored and consistent definitions of PRM, the development of a conceptual description that can serve as reference seems most useful. Based on the unifying ICF model and taxonomy including, among others, the terms human functioning, disability, environmental and personal factors, capacity and performance, it is possible to develop such a description.
An ICF-based conceptual description can serve as a basis for the development of definitions relying on clearly defined and globally agreed terms. In response to specific needs or audiences, one may tailor an appropriate definition by combining terms from the ICF-based conceptual description. Therefore, varying definitions of PRM can still be consistent with respect to the core concepts. The advantage of a conceptual description serving as reference for definitions is that it is easy to modify and develop further in the envisioned iterative process towards a globally agreed version.
ICF terms in the proposed description shown in Table I are marked in bold. Examples of according comprehensive and brief definitions and comments on selected terms used in the conceptual description of rehabilitation are presented in the following sections. Terms that are consistent with the reference definition of rehabilitation as a health strategy are explained in the respective paper (1).
| Table I. ICF-based conceptual description of the medical specialty physical and rehabilitation medicine (PRM). |
| PRM is the medical specialty, which, based on: • the World Health Organization (WHO)‘s integrative model of human functioning, • rehabilitation as its core health strategy applying and integrating the biomedical and engineering approach to optimize a person‘s capacity, approaches which build on and strengthen the resources of the person, provide a facilitating environment and develop performance in the interaction with the environment, and including the diagnosis and treatment of health conditions, • assesses functioning in relation to health conditions, personal and environmental factors including prognosis; the potential to change the prognosis; identification of long-term goals, intervention program goals, rehabilitation-cycle goals and intervention targets; and the evaluation of disability • performs or applies biomedical and engineering interventions to optimize capacity including physical diagnostics, e.g. electro-neurophysiologic testing, assessment of endurance, force and co-ordination; physical modalities such as mechano-therapy including massage, exercise, strengthening and mobilization techniques, heat and cold, water and balneology, light and climate, electric currents including functional electro-physiologic stimulation; neuropsychological interventions; acupuncture, nerve root blockades and local infiltrations; nutritional and pharmacological interventions; rehabilitation technology including, for example, implants, prostheses and orthoses, aids and devices suitable to: stabilize, improve or restore impaired body functions and structures including e.g. de-conditioning; incontinence; sleep and swallowing disturbance; joint instability; and the minimization of pain, fatigue and other symptoms, prevent impairments, medical complications and risks including, for example, depression, sleep disturbance, skin ulcers, thrombosis, joint contractures and muscle atrophy, osteoporosis and falls, compensate for the absence or loss of body functions and structures including, for example, amputation; vision and hearing impairments • leads and co-ordinates intervention programs to optimize performance in a multi-disciplinary iterative problem-solving process performing, applying and integrating biomedical and engineering interventions; psychological and behavioral; educational and counseling; occupational and vocational; social and supportive; and physical environmental interventions • provides advice to patients and relevant persons in their immediate environment, service providers and payers over the course of a health condition along and across the continuum of care ranging from the acute hospital to rehabilitation facilities and the community and across sectors including health, education, labor and social affairs • manages rehabilitation, health and multi-sectorial services • informs and advises the public and decision-makers about suitable policies and programs in the health sector and across the other sectors which: provide a facilitating larger physical and social environment; ensure access to rehabilitation services as a human right; and empower PRM specialists to provide timely and effective care with the goal • to enable people experiencing or likely to experience disability to achieve and maintain optimal functioning in interaction with the environment |
| ICF terms in the proposed description are marked in bold. |
EXAMPLES OF DEFINITIONS BASED ON THE ICF-BASED DESCRIPTION OF PRM
Comprehensive definition
PRM is the medical specialty that aims to enable people experiencing or likely to experience disability to achieve and maintain optimal functioning in interaction with the environment.
It is based on WHO’s integrative model of human functioning, the rehabilitative health strategy, and includes the diagnosis and treatment of health conditions.
PRM specialists assess functioning, perform or apply biomedical and engineering interventions to optimize capacity, and lead and co-ordinate intervention programs in a multi-disciplinary iterative problem-solving process to optimize performance.
They provide advice to people of all age groups and relevant persons in their immediate environment, service providers and payers along the continuum of care and across sectors in all situations from the acute hospital to the community and along the course of the condition.
PRM specialists manage rehabilitation, health and multi-sectorial services. They inform the public and decision-makers about suitable policies and programs in the health sector and across sectors that provide a facilitating larger physical and social environment, ensure access to rehabilitation services as a human right, and empower PRM specialists to provide timely and effective care.
Brief definition
PRM is the medical specialty that, based on the assessment of functioning and including the diagnosis and treatment of health conditions, performs, applies and co-ordinates biomedical and engineering and a wide range of other interventions with the goal of optimizing functioning of people experiencing or likely to experience disability.
Alternative brief definition
PRM is the medical specialty that aims to optimize functioning of people experiencing or likely to experience disability including the diagnosis and treatment of health conditions.
COMMENTS ON SELECTED TERMS USED IN THE CONCEPTUAL DESCRIPTION OF PRM
“PRM is the medical specialty, which, based on: (i) WHO´s integrative model of human functioning; and (ii) rehabilitation as its core health strategy”
By definition, and as indicated in its name, rehabilitation is the core health strategy of PRM. While there are other medical specialties that may apply rehabilitation as a relevant strategy, PRM is arguably the only specialty which systematically applies the rehabilitation strategy across populations, settings and situations from the acute hospital to the community. Thus “the” and not “a medical specialty” seems justified.
While rehabilitation is the core health strategy of PRM, as any other medical specialty, PRM also integrates the curative, preventive and supportive strategy (1). For example, PRM refers specifically to the curative strategy when “restoring impaired body functions and structures” and the preventive strategy when “preventing impairments, medical complications and risks”. PRM also refers specifically to the preventive strategy when aiming to “maintain optimal functioning”.
“and including the diagnosis and treatment of health conditions”
The diagnosis and treatment of health conditions are the cornerstones of any medical specialty. The inclusion of diagnosis and treatment in the definition is essential for the specialty, for example, to be qualified to “lead and co-ordinate the multi-disciplinary team effort” to improve functioning in relation to health conditions, personal and environmental factors. PRM specialists can cover the broad spectrum of health conditions that, according to the WHO, can result in limitations in functioning. These include diseases, injuries, aging and congenital anomalies. As any other medical specialty, PRM may co-operate with disease or organ specialists in the treatment of these conditions.
“assesses functioning in relation to health conditions, personal and environmental factors”
The unique feature of PRM is the focus on the assessment of human functioning, disability and health. While other medical specialties focus on the diagnosis and treatment of diseases or injuries, PRM specialists particularly focus on functioning.
The diagnosis of human functioning disability is called “assessment”. The assessment of functioning includes the components body functions and structures, activities and participation. A person’s functioning can only be understood in the context of health conditions, personal factors and environmental factors. The assessment, therefore, explicitly includes these components. As mentioned above, the diagnosis and treatment of health conditions is an integral part of the specialty. In addition, PRM specialists are knowledgeable about personal and environmental factors.
The goal of the assessment is to understand or model a person’s experience of disability in relation to impairments and/or in relation to interaction with environmental and personal factors. PRM specialists structure their assessment based on the ICF, for example, using the ICF sheet (14).
The assessment of functioning includes the assessment of prognosis (What is the natural course of functioning?) and the potential for change (Can we change the natural course?), the identification of long-term goals (What is the goal at the end of the current rehabilitation journey, e.g. after an acute episode or over the next year in a chronic condition?), the intervention program goals (What does the multi-disciplinary team want to achieve with its intervention program, e.g. during an early post-acute rehabilitation program or a multidisciplinary pain program?), rehabilitation-cycle goals (What does the multi-disciplinary team want to achieve in its next rehabilitation-cycle over the next days and week(s) during the course of an intervention program of several weeks?) (15), program intervention goals (What does the assigned health professional want to achieve with his or her intervention?).
PRM specialists often also assess legal disability.
“performs or applies biomedical and engineering interventions to optimize capacity”; “including physical modalities …”; “suitable to …”
PRM specialists “perform” or “apply” interventions. The term “apply” indicates that the intervention may be performed under the auspice but not directly by the PRM specialist.
“Intervention” is a most general umbrella term for the actions of a PRM specialist. The term also includes the treatment of the health condition. An intervention may be performed using a specific “intervention technique”. For practical reasons no differentiation of interventions, intervention principles or intervention techniques is made in the conceptual description.
The goal of biomedical and engineering interventions is to optimize a person’s capacity which describes what a person can do in a standardized or “ideal” environment. In order to optimize a person’s capacity, interventions are applied that are suitable to “stabilize, improve or restore impaired body functions and structures; prevent impairments, medical complications and risks; or compensate for the absence or loss of body functions and structures”.
“leads and co-ordinates intervention programs to optimize performance in a multi-disciplinary iterative problem-solving process
Because of their complexity, intervention programs applying the rehabilitation strategy are typically lead and co-ordinated by a PRM specialist and delivered in a multi-disciplinary iterative problem-solving process.
The term “intervention program” differentiates from the word “program” as used in the context of designated proposals including policies, programs and projects on the societal level (16). Interventions (performed by a health professional), intervention programs (delivered by a team) and services (offered by a provider and paid for by a payer) are the actions in the context of health service provision. Projects and programs (by authorities) and policies (by policy-makers) are the actions on the societal level.
To co-ordinate intervention programs, PRM specialists increasingly use the ICF as common language, e.g. within multi-disciplinary teams or inter-disciplinary intervention programs across teams and/or services.
In the “co-ordination” of intervention programs PRM specialists typically rely on a problem-solving iterative approach, as described in the “Rehab-CYCLE” (8, 14, 17, 18). The “Rehab-CYCLE” involves the following 4 steps: “assessment, assignment, intervention and evaluation”, or, in a more proactive taxonomy, “assess, assign, intervene and evaluate”.
The assessment step includes the identification of patients’ problems, the definition or review of the long-term goal (e.g. re-integration into the prior work or living situation), the definition or review of assigned “intervention program goals” (e.g. assigned by a case manager or a PRM specialist leading a prior intervention program), and the definition of the “Rehab-CYCLE goals” set by the team and the “intervention targets” for each professional. Intervention-program goals, Rehab-CYCLE goals and intervention targets are typically matched to ICF categories allowing for easy communication within a team and across services.
The assignment step refers to the assignment of health professionals and the assignment of interventions to the “intervention targets”. Different interventions provided by different professionals may be applied to the same intervention target.
The intervention step refers to the specification of the “intervention techniques”, the definition of “indicator measures” to follow the progress of the intervention, and the definition of “target values” to be achieved within a pre-set time period.
The evaluation step refers to the evaluation of intervention-target achievement with respect to the specified “target values” of the “indicator measures”, the “Rehab-CYCLE” goals, and ultimately the “intervention program goals”. It also includes the decision regarding the need for another “Rehab-CYCLE” based on a re-assessment.
“performing, applying and integrating; biomedical and engineering interventions; psychological and behavioral; educational and counseling; occupational and vocational; social and supportive, and physical environmental interventions”
In the context of intervention programs PRM specialists perform, apply and integrate a wide range of interventions suitable to improve functioning in relation to the approaches of the rehabilitation strategy. The rehabilitation strategy includes biomedical and engineering approaches, approaches that build on and strengthen the resources of the person, approaches that provide a facilitating environment, and that develop performance in interaction with the environment.
PRM specialists are uniquely positioned to integrate biomedical interventions in the broader context of the comprehensive rehabilitation strategy based on the integrative model of functioning, disability and health.
“provides advice to patients and relevant persons in their immediate environment, service providers and payers”
The formulation provides advice to is preferable over the terms “manage” or “case management”. To refer to a person with a health condition experiencing disability as a “case” and to refer to organizing the rehabilitation process as “case management” is not respectful. Guidance may be considered too paternalistic. Advice is a more appropriate, respectful and person-oriented term to denote the process of organizing the rehabilitation in partnership with the person and relevant persons in his or her immediate environment including significant others and employers, service providers and others.
PRM specialists advise people with health conditions about qualified health services and the envisioned effectiveness of alternative intervention programs and request insurers to cover their costs. They may also advise patients about services provided by other sectors including social affairs, labor and education.
Based on the problem-solving iterative approach, PRM specialists negotiate and evaluate “long-term goals”, assign patients to appropriate rehabilitation services and intervention programs and evaluate the attainment of agreed “intervention program goals”.
“in all situations over the course of a health condition; along and across the continuum of care, ranging from the acute hospital to rehabilitation facilities and the community; and across sectors, including health, education, labor and social affairs”
There is currently no general and internationally accepted framework for rehabilitation service and care provision along the continuum of care.
Anywhere in the world, the acute hospital and the community are the 2 “anchor” settings. The term community is also used by the Disability and Rehabilitation (DAR) team at WHO in the context of “Community Based Rehabilitation”.
Based on attempts, e.g. in relation to the development of ICF Core Sets (19) in which the rationale and principles of rehabilitation in the acute hospital and early post-acute rehabilitation have been outlined, it is envisioned to develop a framework for service types and criteria for service provision in situations between the 2 “anchors” from an international perspective.
“informs and advises the public and decision makers about suitable policies and programs in the health sector and across other sectors which …”
PRM specialists are limited in their efforts if the larger environment is not facilitating or if they cannot provide services in a timely fashion. What constitutes a facilitating environment may differ across populations, e.g. with respect to underlying health conditions, age and gender. PRM specialists and their scientific and professional societies are thus informing and advising the public and decision-makers about suitable policies and programs (16).
“and manages rehabilitation, health and multi-sectorial services”
The term “manage” is generally used and appropriate with respect to the organization of a service. PRM specialists manage services along the continuum of care in all situations from the acute hospital to the community.
The term “service” is preferable over the also often-used term “program” to avoid confusion with the term “program” as used on the societal level. A service typically offers “intervention programs” as mentioned above.
While PRM specialists, by definition, manage rehabilitation services, they may also manage health services not specifically denoted as such. Examples include pain clinics, which may run a number of intervention programs including, for example, a 4-week multidisciplinary pain program. Other examples are geriatric services and PRM services provided on general, intensive and intermediate care and specialized wards in the acute hospital.
“to enable people experiencing or likely to experience disability…”
Since these terms are in common with the terms used in the tentative definition of rehabilitation understood as a health strategy they are discussed in the respective paper (1).
CONCLUSION
The conceptual description and the examples of comprehensive and brief definitions presented here are tentative. They are intended to open the discourse and to initiate the process of moving towards an international taxonomy and internationally accepted conceptual description and definitions of PRM. The UEMS-PRM-section supports this process and aims to adopt an “ICF-based conceptual description of PRM” and according brief and comprehensive definitions within the next 2 years. It is also envisioned bringing the conceptual description to the attention of other regional organizations and the International Society of Physical and Rehabilitation Medicine (ISPRM).
In many countries, including the Scandinavian countries, Japan and Australia, the medical specialty PRM is simply called rehabilitation medicine. In others, especially in the Mediterranean region, physical medicine is an important and explicit aspect of the specialty. Aiming for a globally accepted conceptual description, we have included the aspects of physical medicine in the definition but not provided a separate definition.
However, physical medicine is implicitly described in the ICF-based conceptual description of PRM, namely in the part “… performs or applies biomedical and engineering interventions to optimize capacity …”. This description, which focuses on body functions and structures, is closely related to a tentative conceptual description of “biomedical rehabilitation sciences and engineering” (4, 5).
The Journal of Rehabilitation Medicine aims to contribute to the process of achieving an internationally accepted ICF-based conceptual description of PRM by inviting readers to submit commentaries to the Editor. Of particular interest are comments regarding the understanding and definition of physical medicine in the context of the medical specialty PRM. For example, could physical medicine, in line with the ICF, be described as therapeutic interaction between environment and the person? In this context also the meaning of the term “physical” would need to be clarified.
We conclude that the ICF is a suitable unifying model for the conceptual description of PRM based on a respective conceptual description of the rehabilitation strategy (1). A conceptually sound and generally accepted conceptual description is an important basis for research, teaching and clinical service provision, and may hence help to achieve the mission of PRM to contribute to optimal functioning of people experiencing or likely to experience disability.
ACKNOWLEDGMENTS
The authors thank Susanne Stucki; Drs Alarcos Cieza and Jan Reinhardt from Swiss Paraplegic Research; Drs Somnath Chatterji, Bedirhan Üstün and Nenad Kostansjek from the Classification and Terminology (CAT) team at the WHO; and Drs Federico Montero and Chapal Kashnabis from the Disability and Rehabilitation (DAR) team at the WHO for their thoughtful comments.
This paper has been written in co-operation with the UEMS-PRM-section and its professional practice committee (Christoph Gutenbrunner, chair; members Tamas Bender, Mihai Berteanu, Pedro Cantista, Nicholas Christodoulou, Hermina Damjan, Veronika Fialka-Moser, Alessandro Giustini, Gordana Devcerski, Zafer Hascelik, Eero Kyllönen, Timo Pohjolainen, Fernando Parada, Hildegun Snekkevik, Marianthi Tzara, Daniel Uebelhart, Enrique Valera, Jiri Votava, Aivars Vetra, Anthony Ward).
REFERENCES
1. Stucki G, Cieza A, Melvin J. The International Classification of Functioning, Disability and Health: A unifying model for a conceptual description of the rehabilitation strategy. J Rehabil Med 2007; 39: 279–285.
2. World Health Organization. International Classification of Functioning, Disability and Health: ICF. Geneva: World Health Organization; 2001.
3. Stucki G. International Classification of Functioning, Disability and Health (ICF): A promising framework and classification for rehabilitation medicine. Am J Phys Med Rehabil 2005; 84: 733–740.
4. Stucki G, Grimby G. Organizing human functioning and rehabilitation research into distinct scientific fields. Part I: Developing a comprehensive structure from the cell to society. J Rehabil Med 2007; 39: 293–298.
5. Stucki G, Reinhardt JD, Grimby G. Organizing human functioning and rehabilitation research into distinct scientific fields. Part II: Conceptual descriptions and domains for research. J Rehabil Med 2007; 39: 299–307.
6. Stucki G, Grimby G. Foreword. Applying the ICF in medicine. J Rehabil Med 2004; 36 Supp 44: 5–6.
7. Stucki G, Üstün TB, Melvin J. Applying the ICF for the acute hospital and early post-acute rehabilitation facilities. Disabil Rehabil 2005; 27: 349–352.
8. Stucki G, Ewert T, Cieza A. Value and application of the ICF in rehabilitation medicine. Disabil Rehabil 2002; 24: 932–938.
9. Walsh NE. The Walter J. Zeiter lecture. Global initiatives in rehabilitation medicine. Arch Phys Med Rehabil 2004; 85: 1395–1402.
10. Stucki G, Cieza A, Ewert T, Konstanjsek N, Chatterji S, Bedirhan Ustun T. Application on the international classification of functioning, disability and health (ICF) in clinical practice. Disabil Rehabil 2002; 24: 281–282.
11. Üstün B, Chatterji S, Kostanjsek N. Comments from WHO for the Journal of Rehabilitation Medicine special supplement on ICF core sets. J Rehabil Med 2004; 36 Suppl 44: 7–8.
12. Cieza A, Ewert T, Üstün TB, Chatterji S, Kostanjsek N, Stucki G. Development of ICF core sets for patients with chronic conditions. J Rehabil Med 2004; 36 Suppl 44: 9–11.
13. Grill E, Ewert T, Chatterji S, Kostanjsek N, Stucki G. ICF Core Set development for the acute hospital and early post-acute rehabilitation facilities. Disabil Rehabil 2005; 27: 361–366.
14. Steiner WA, Ryser L, Huber E, Uebelhart D, Aeschlimann A, Stucki G. Use of the ICF model as a clinical problem-solving tool in physical therapy and rehabilitation medicine. Phys Ther 2002; 82: 1098–1107.
15. Stucki G, Kröling P. Principles in rehabilitation. In: Hochberg MC, Silman AJ, Smolen JS, Weinblatt ME, Weisman MH, editors. Rheumatology 4th edition. Philadelphia: Mosby; 2007 (in press).
16. Mindell J, Ison E, Joffe M. A glossary for health impact assessment. J Epidemiol Community Health 2003; 57: 647–651.
17. Stucki G, Cieza A. The International Classification of Functioning, Disability and Health (ICF) core sets for rheumatoid arthritis: a way to specify functioning. Ann Rheum Dis 2004; 63 Suppl 2: ii40–ii45.
18. Stucki G, Ewert T. How to assess the impact of arthritis on the individual patient: the WHO ICF. Ann Rheum Dis 2005; 64: 664–668.
19. Stucki G, Stier-Jarmer M, Grill E, Melvin J. Rationale and principles of early rehabilitation care after an acute injury or illness. Disabil Rehabil 2005; 27: 353–359.