


1Melanoma Skin Unit, Hospital Clinic of Barcelona, IDIBAPS, University of Barcelona, CIBER de enfermedades raras ICIII, Barcelona, Spain and 2Department of Dermatology, University of Modena and Reggio Emilia, Modena, Italy
Non-melanoma skin cancer (NMSC), including basal cell and squamous cell carcinomas, is the most common form of neoplasm. The incidence of NMSC is increasing worldwide. The cure rate is high with early detection and appropriate treatment. Visual examination is the first screening tool used by clinicians, but it is sometimes not sufficient to discriminate benign from malignant lesions. Skin biopsy with histopathology is the gold standard for differential diagnosis; however, this procedure is invasive and occasionally painful. Repeated tissue sampling is not possible in patients with several suspicious lesions and various clinical presentations that are challenging to identify. There are several medical imaging tools for non-invasive in-depth skin examination that can be used to guide clinical diagnosis: dermoscopy, confocal microscopy, cross-polarized light and fluorescence photography, optical coherence tomography and high-frequency ultrasound. These tools are discussed along with their clinical applications. These techniques provide valuable morphological information for better identification, confident diagnosis and treatment monitoring of NMSC.
Key words: basal cell carcinoma; actinic keratosis; squamous cell carcinoma; confocal microscopy; dermoscopy; non-invasive technology.
Accepted May 22, 2017; Epub ahead of print Jul 3, 2017
Acta Derm Venereol 2017; Suppl 218: 22–30.
Corr: Josep Malvehy, Melanoma Unit, Hospital Clinic of Barcelona, ES-08036 Barcelona, Spain. E-mail: jmalvehy@gmail.com
Basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) are the most common forms of skin cancer, accounting for approximately 80% of all non-melanoma skin cancers (NMSC) and 20% of all cutaneous cancers, respectively (1, 2). Actinic keratosis (AK) should be included within the disease spectrum of SCC, since it presents shared histopathological features and has the potential to progress to invasive SCC in up to 1% of cases (3). All AK lesions typically result from sustained exposure to ultraviolet radiation (UV) from the sun. In fair-skinned individuals over 60 years of age and in countries with high levels of sunlight, it is estimated that approximately 28–50% of the population is affected by AK, and its incidence is increasing worldwide (4). Despite the very high prevalence of AK in some countries (5), its importance in public health is often underestimated. History of sun-exposure, sun-damaged skin, associated with a fair skin phototype, and a genetic predisposition are the main factors that can lead to the development of skin cancer. The cure rate for these non-melanoma skin diseases is high, given early detection, accurate diagnosis and appropriate treatment. However, patients often have multiple equivocal lesions, sometimes confluent, covering large areas with various clinical presentations, making it difficult to reach a proper diagnosis and to separate malignant from benign lesions.
Skin cancer screening typically starts with an un-aided visual inspection conducted by a trained physician. In some cases, clinicians face the complicated task of deciding which lesion requires a conventional biopsy with thorough histopathological analysis of the excised specimen, which is the only way to establish a definite diagnosis of a suspicious lesion (5). Several medical imaging technologies are available as adjunctive tools for non-invasive in-depth examination of non-melanoma skin cancers (NMSC) to enable accurate differential diagnosis and optimal treatment. This paper focuses on dermoscopy and confocal microscopy, and other diagnostic complementary tools, such as cross-polarized light and fluorescence photography, optical coherence tomography (OCT) and high-frequency ultrasound (HFU). We introduce the most relevant dermoscopic features to detect keratinizing tumours, briefly describe the technology behind confocal microscopy, and discuss the advantages and limitations of using this procedure in differential diagnosis of NMSC and AK, and in therapy monitoring. The second part of the paper discusses how dermoscopy, cross-polarized light and fluorescence photography, OCT and HFU can also assist clinicians in fully assessing the burden of NMSC. Patients with skin cancer will continue to benefit from ongoing technological advancements in these imaging tools, enabling early diagnosis and provision of therapy monitoring.
Dermoscopy (also called epiluminescence microscopy) is a real-time non-invasive surface skin microscopy procedure with a polarized light source and a high-quality magnifying lens for the visualization of superficial abnormalities in the epidermis, dermoepidermal junction and superficial dermis. The benefit of dermoscopy in improving the diagnosis of melanoma is described in another paper in this supplement (see Thomas & Puig, 6). However, dermoscopy has also proven effective in the diagnosis of other skin conditions, such as AK, which are often difficult to interpret on inspection with the naked eye. Typical dermoscopic features of non-pigmented AK form a composite “strawberry pattern” (Figs 1 and 2) characterized by a pink-to-red erythema pseudo-network consisting of large linear wavy blood vessels surrounding the hair follicles (7). Prominent follicular openings are filled with yellowish keratotic plugs and surrounded by a white halo. Dermoscopic examination of a pigmented AK reveals lesions that are asymmetrical in colour and structure, with blue dots and dilated hair follicles typical of pigmented AK (Fig. 3).
Fig. 1. Strawberry pattern in dermoscopy of an actinic keratosis. Scale bar corresponds to 1 mm.
Fig. 2. Non-pigmented actinic keratosis (AK). (a) AK on the forehead of a patient with skin damage. (b) Dermoscopy reveals the typical strawberry pattern and rosettes (arrows). Scale bar corresponds to 1 mm.
Fig. 3. Clinical and dermoscopic aspect of a pigmented actinic keratosis (PAK). (a) A patient with severe sun damage on the scalp. (b) Dermoscopy reveals that the lesions exhibit asymmetry in colours and structures, with blue dots and dilated hair follicles typically seen in PAK. Each graduation on the scale corresponds to 1 mm.
In a study conducted in 178 patients with AK, Huerta-Brogeras et al. (8) reported a high sensitivity and specificity of dermoscopic diagnosis, with a strong concordance between the dermoscopic results and histo-pathology. However, although commonly observed in AK, the “strawberry pattern” is not specific to this type of lesion. In fact, a dermoscopic examination of an AK in 2009 (9) documented a lichenoid AK and an SCC that developed on an AK in 3 different patients and revealed a different arrangement, named rosette structures, characterized by 4 white points arranged in a 4-leaf clover generally localized inside the follicular openings (Fig. 2). Dermoscopic rosettes have also been described in patients with pigmented incipient melanoma, but remain a rare occurrence in this type of cancer (10).
The exact correlation between the morphological skin features and the dermoscopic images of these formations is poorly understood. Haspeslagh et al. (11) recently performed ex vivo dermoscopy on 6,108 skin biopsies with a variety of lesions, such as BCC, SCC, melanoma, naevus, and reported the presence of rosettes in 63 cases. Dermoscopic examination of transverse sections of these lesions revealed that large rosettes are a simple optical effect resulting from crossed polarization by concentric perifollicular fibrosis and are observed in a wide range of skin conditions and therefore are not specific.
Dermoscopy can also assist in our understanding of the progression of facial AK into intraepidermal carcinoma (IEC) (or in situ SCC) and invasive SCC. Squamous cell carcinoma has specific dermoscopic clues depending on its differentiation and invasiveness. Zalaudek et al. (12) found a strong correlation between the presence of a red pseudonetwork and AK, whereas dotted blood vessels, diffuse yellow opaque scales and microerosions were more prevalent in cases of IEC. The presence of white circles is also a typical feature of well-differentiated SCC (Fig. 4).
Fig. 4. A well-differentiated squamous cell carcinoma on the face of a patient (inset). The dermoscopic image shows white circles (asterisks) corresponding to the atypical keratinized follicles, atypical vessels and central keratin of the tumour. Scale bar corresponds to 1 mm.
Zalaudek et al. (12) also reported that hairpin and linear irregular vessels, targetoid hair follicles, white structureless areas, a central mass of keratin and ulceration were predominantly observed in invasive SCC (Fig. 5). These findings highlight the importance of accurate interpretation of the dermoscopic images for a proper diagnosis when facing equivocal lesions with similarities that are difficult to analyse. Careful analysis of the dermoscopic clues is essential to recognize the characteristics of a red starburst pattern, signs of dynamic process of AK progression into IEC, and to separate well-differentiated (white circles, keratinization) (Fig. 4) from poorly differentiated SCC (blood vessels) (Fig. 5).
Fig. 5. Dermoscopic image of a non-differentiated squamous cell carcinoma with no features associated with keratinization and atypical vessels. Scale bar corresponds to 1 mm.
In non-pigmented Bowen’s disease, a form of intraepidermal in situ SCC, the dermoscopic appearance consists of a scaly surface and clusters of glomerular (or linear coiled) and occasionally dotted vessels frequently dilated in the papillary dermis (Fig. 6). Irregular, linear, polymorphous arborizing vessels are sometimes observed (13). The pigmented form of Bowen’s disease is rare and has a specific dermoscopic pattern characterized by erythematous hyperkeratotic plaque together with a linear arrangement of grey-to-brown dots and coiled vessels and small brown-to-black globules with a patchy distribution and irregular diffuse grey-to-brown pigmentation (14, 15).
Fig. 6. Dermoscopic image of Bowen’s disease with scaling and glomerular vessels arranged in clusters. Scale bar corresponds to 1 mm.
Dermoscopy is also an important tool in the diagnosis of BCC. Dermoscopic characteristics of hypopigmented BCC include arborizing and fine short blood vessels, ulceration, multifocal erosions, white shiny areas and brown-grey dots (16–18) (Fig. 7).
Fig. 7. Dermoscopy of a non-pigmented basal cell carcinoma with arborizing vessels (asterisk). Scale bar corresponds to 1 mm.
Dermoscopy is therefore a valuable tool in the diagnosis of AK, which are often difficult to interpret on inspection with the naked eye, and in the visualization of progression of facial precancerous AK lesions into IEC (or in situ SCC), and invasive SCC, and the diagnosis of BCC.
Confocal microscopy (also called reflectance confocal microscopy) is a well-known technology that has been used in biology since the late 1950s. Over the past 2 decades, the development of confocal microscopy as a clinical tool in dermatology has enabled the in-depth exploration of human skin. The confocal microscope is expensive, which limits the number of users compared with dermoscopy. However, it is steadily gaining popularity in the scientific community due to its advantages as a non-invasive diagnostic tool in skin diseases.
In dermatology, a major advantage of confocal microscopy is that it enables non-invasive painless in vivo visualization of the skin in real time with a cellular level resolution without the need for biopsy. Despite being a powerful tool, the technology used in this equipment is relatively simple. Light emitted by a laser diode at 830 nm (a safe wavelength for patient and operator) is reflected, directed through a small pinhole, and arrives at the detector, where an image is formed of horizontal sections of the different layers of an area of the skin depicting intracellular structures. Melanin and cytoplasmic organelles offer a strong endogenous contrast source for robust reflection. The penetration depth for diagnostic purposes is usually up to 200 µm, which corresponds to the superficial dermis. The emitted light can go deeper, but as depth increases the image resolution is reduced. High-resolution black-and-white images are obtained with a resolution comparable to that of histopathology, which is the gold standard for the diagnosis of cutaneous lesions.
Vivascope 1500® and 3000® (MAVIG GmbH, Munich, Germany) (Fig. 8) are confocal systems widely used in dermatology for cellular skin analyses. The 1500® device captures images through a metallic tissue ring in direct contact with the skin. The ring stabilizes the apparatus in order to generate stable in vivo cellular resolution unstained images in real time, focusing on a single point on the skin surface. This technology produces a stack of consecutive high-resolution confocal images on a single spot starting from the surface and increasing in depth by a predetermined constant step (≥ 1µm). In the mosaic mode with a predetermined depth of penetration, a composite image is formed by consecutive confocal frames and mounted together in order to generate a horizontal section of a lesion and create a map of a specific area up to 8 × 8 mm.
Fig. 8. Confocal microscope Vivascope 1500® (with the kind permission of Giuseppe Solomita from MAVIG GmbH, Munich, Germany).
The Vivascope 1500® confocal microscopy system is particularly indicated to assist in the interpretation of atypical naevi vs. melanoma (19–30), but also hypopigmented vs. amelanotic lesions (31) when the differential diagnosis is difficult. This advanced technological diagnostic method can provide valuable information about the extent of architectural disorder in the epidermis, along with cytological features pertinent to the lesion.
The Vivascope 3000® can be handled and placed directly on the skin, but, in contrast to the 1500® system, it allows visualization only of the point it is focusing on and cannot provide a map or mosaic of a specific skin area. The 3000® system is therefore more appropriate for diagnosis of lentigo maligna and freckles on the face (32–34), BCC (35–42), inflammatory diseases (43), and for cosmetology applications (44–47).
Limitations of confocal microscopy include the depth of laser penetration. In cases of palmoplantar or hyperkeratotic lesions, with crust or ulceration where the skin is too thick, light penetrates only to the superficial stratum spinosum.
Despite these limitations, confocal microscopy is widely used for the diagnosis of melanocytic lesions given its excellent capability to distinguish naevi from melanoma. Confocal microscopy can also be used to diagnose difficult BCC and identify histopathological alterations in keratinizing tumours, thus its application is indicated in diagnosis of skin cancer. Moreover, the systematic use of this technology associated with dermoscopy results in a significant reduction in excision of benign lesions in different settings, as detailed in the next section.
In clinical practice, confocal microscopy is a valuable diagnostic aid in dermoscopically equivocal lesions. It is best indicated for BCC when a confident and precise diagnostic cannot be established by dermoscopy (48). Differential diagnoses of some clinical cases of ulcerated BCC with polymorphic vessels include amelanotic melanoma and SCC, and confocal microscopy is useful to improve the accuracy of diagnosis (48). Confocal microscopy can visualize all the features of a BCC, including tumour islands, palisading cells, peritumoral clefting, and thick collagen deposits around the islands, with a high correspondence with histopathology (Fig. 9). Positive factors for BCC diagnosis are: polarized elongated structures in the superficial layer, linear telangiectasia-like horizontal vessels, compact nests of hyporeflective cells, peripheral palisading, and epidermal shadowing. Negative factors are: atypical honeycomb pattern, non-visible papillae, and cerebriform nests (37).
Fig. 9. Confocal image of a pigmented basal cell carcinoma. Vivablock of the tumour with nest of basaloid cells (asterisk), palisading (white arrows) and clefting (white arrowheads). Scale bar corresponds to 1 mm.
In a paper published in 2014, Longo et al. (40) described how diagnosis of BCC subtypes can be achieved by dermoscopy and confocal microscopy. Superficial BCC were characterized by fine telangiectasia, multiple erosions, leaf-like structures, and cords connected to the epidermis. Nodular BCC mainly displayed classic dermoscopic features and well-outlined large basaloid islands, while infiltrative BCC displayed structureless, shiny red areas, fine telangiectasia, and arborizing vessels on dermoscopy, and dark silhouettes on reflectance confocal microscopy.
Confocal microscopy is also indicated in the diagnosis and surveillance of AK and SCC, as well as to detect and monitor cytological alterations present in the cancerization field. Characteristic skin changes occurring during AK can be seen on confocal images and include architectural disarray, keratinocyte pleomorphism and focal areas of atypical honeycomb pattern (49).
Confocal microscopy can also be used as a tool for
therapeutic monitoring, offering insights into the cellular response to treatments for AK (49, 50) in combination with OCT (51) and superficial BCC (52) when visual inspection alone is not sufficient.
The use of confocal microscopy is also strongly recommended to monitor the response rate to non-invasive photodynamic therapy for NMSC, such as BCC. In some doubtful cases, a skin biopsy is necessary to evaluate the possible persistence of cancerous cells after treatment. In a study published in 2012 (53), cellular imaging of the BCC lesions 7 days after initiation of the therapy demonstrated the presence of dendritic-shaped cells in the epidermis. At long-term follow-up, confocal microscopy revealed complete clearance of the tumour islands, thus demonstrating the efficacy of non-surgical photodynamic therapy for BCC.
Cross-polarized light and fluorescence photography are easy-to-use imaging techniques that can assist dermatologists in detecting and identifying subclinical AK lesions that are often invisible to the naked eye (54, 55). When the skin is illuminated with cross-polarized light, underlying blood vessels, pigmentation and details of the lesion, such as AK and BCC, will appear distinctly on the illumination map when using the appropriate coloured filters (56).
The fluorescence approach uses endogenous fluoro-phore proteins (flavins, collagen, elastin, lipopigments and porphyrins) present in the human skin, each with a unique absorption and emission spectrum. These molecules absorb energy, passing from the ground state to an excited state, and release this energy in the form of fluorescence. Although more sensitive, this imaging technique is also more time-consuming and requires topical application of methyl-aminolaevulinic acid to induce the formation of porphyrin in the skin and visualize the lesion (56). The major limiting factor when employing these non-invasive optical methods is the low-resolution, as the depth to which the light can penetrate the skin cannot capture images at the cellular level. However, these methods can provide important information to guide diagnosis.
The Visia CR (Canfield, Parsippany, USA) facial multimodal imaging system, although still experimental, has the advantage of combining standard, polarized light, UV and fluorescence to produce very high-resolution standardized images (Fig. 10). This system is particularly indicated in patients presenting multiple equivocal AK or keratinizing tumours that are difficult to see with the naked eye and challenging to interpret. Rapid advances in technology might make multimodal dermoscopy a reality in the near future.
Fig. 10. Multispectral images of a patient with actinic keratosis and field cancerization on the scalp (Visia, Canfield, Parsippany, USA). Compared with photography using normal light, multiple lesions are detected with green and mixed lighting.
Optical coherence tomography (OCT) is an emerging non-invasive diagnostic method that offers a real-time in vivo view into the superficial layers of the skin. This rapidly evolving technology has multiple clinical applications and has been commonly used in ophthalmology since 1991. OCT offers detailed morphological and structural images of the epidermis, upper dermis and dermal-epidermal junction. Blood vessels can also be visualized, along with skin appendages, such as hair follicle units, and sebaceous glands (57). Since its introduction in dermatology in 1997, OCT has been widely used in the diagnosis of skin conditions, such as BCC, AK and SCC. Briefly, an infrared light source is used to probe and visualize details of skin structure, with a resolution between 3 and 15 μm and depth of up to 1–2 mm depending on the system. This powerful device can provide high-resolution images of NMSC, inflammatory diseases and parasitic infestations to complement other non-invasive diagnostic imaging tools. Valuable quantitative and qualitative information can be obtained from vertical sections of the skin with different degrees of resolution. As an additional tool to improve diagnosis, Boone et al. (58) have recently developed an algorithm for high-definition OCT, combining horizontal and vertical images for three-dimensional imaging. High-definition OCT can assist the clinician in discriminating AK from normal skin and SCC by detecting hyperkeratotic material and epidermal atypia typical of AK in real-time (Fig. 11). In cases of SCC, evidence of the destruction of the dermal epidermal junction can be seen with OCT, which is a sign that the tumour is progressing and needs to be excised. OCT also has an important clinical value in providing a precise classification of BCC subtypes (superficial, nodular and infiltrative), each with highly specific shape, size and location characteristics. OCT evaluation can help in differentiating an equivocal, very superficial, early BCC from other tumours when the diagnosis is difficult. In addition, this imaging technique is of particular in delineating tumour margins in BCC prior to excision (59), enabling more efficient tumour surgery and an increased success rate.
Fig. 11. High-definition optical coherence tomography image of an actinic keratosis with vertical section (upper image) and horizontal section (lower image). Note the thickening of the stratum corneum (asterisk) and the irregular architecture of the tumour (white arrows); dermoepidermal junction is preserved (white arrowheads). Scale bar corresponds to 1 mm.
High-frequency ultrasound (HFU) is a novel real-time in vivo imaging technique that can differentiate skin layers and deeper structures for the diagnosis and treatment of dermatological conditions, including inflammatory diseases and NMSC, such as BCC.
This technology is based on ultrasonic waves that are transmitted from a probe and travel through the skin before being reflected back to a transducer, based on intrinsic variations in keratin, collagen and water content. This optical tool entails the translation of these sound waves into grey-scale images that can be visualized for interpretation. The higher the frequency of the ultrasonic waves, the higher the resolution. In BCC, HFU permits clear visualization of the tumour margins and assists in evaluating whether the tumour is superficial, nodular or infiltrative. In a retrospective study published in 2010, Wortsman & Wortsman (60) evaluated the diagnostic value of HFU by imaging 4,338 cutaneous lesions along with 130 normal control specimens. They found that the ultrasound diagnosis matched the final diagnosis in 73% of cases, with 97% accuracy and 100% specificity. Although HFU is currently a developing tool with some technical limitations, the authors concluded that it is a promising adjunct imaging modality that could provide physicians with additional valuable information to enable diagnosis. In addition, the presence and number of intralesional hyperechoic spots might help in predicting the risk of recurrence in micronodular, sclerosing variant and morpheaform subtypes of BCC (61). HFU is therefore considered to be a reliable complementary tool for accurate diagnosis of NMSC.
Several other non-invasive optical diagnostic tools and innovative technologies that are already available or are still being developed, such as Raman spectroscopy and multiphoton microscopy, have potential clinical applications in skin cancer diagnosis. These are described in another paper in this supplement (see Tkaczyk, 62).
Ex vivo confocal microscopy with fluorescence can be used in combination with Mohs surgery, which is the most effective technique for precise excision of tumours, such as aggressive BCC and SCC, with minimal damage to the surrounding normal tissue (Fig. 12). Using this procedure, the lesion is removed one layer at a time and the layers are examined immediately with ex vivo fluorescence confocal microscopy (35, 41, 63). Cancer cells and tumour margins can be detected rapidly and easily during surgery without the need for frozen sectioning and processing, which is time-consuming and labour-intensive. Nuclei, fibroblasts, inflammatory cells, hair follicles, accrine glands, fat tissue, sebaceous glands, sweat glands, arteries, and skeletal muscle can be imaged precisely and stained digitally on confocal mosaics to simulate histopathology (64).
Fig. 12. Confocal microscopy of a basal cell carcinoma in ex vivo examination with acridine orange during a Mohs’ surgical procedure. The tumour nests are evident (magnification in red square) using this rapid examination. Scale bar corresponds to 1 mm.
NMSC are increasing worlwide, and yet are curable if identified early, diagnosed properly and treated promptly and appropriately. Powerful imaging non-invasive technologies for in-depth examination of the skin have ben developed and optimized over the past two decades. Dermoscopy, confocal microscopy, OCT and HFU provide real-time images at the cellular and subcellular levels to assist the clinician in making rapid and accurate decisions when confronted with equivocal lesions, without the need for invasive biopsies. Learning curves in all these imaging technologies are different depending on the difficulty to identify lesions. Interpretation of lesions with a basic, easy-to-identify pattern is possible with a training of a few hours in the case of dermoscopy, OCT or confocal microscopy. However, training during a few years is needed to gain expertise for advanced diagnosis of difficult-to-recognize lesions. Emerging technologies, such as multiphoton microscopy and Raman spectroscopy, are state-of-the-art tools from which patients will benefit greatly in the coming years with continuing technological advancements in this field. As they develop and are used in combination as complementary imaging tools, all those techniques will provide detailed, higher sensitivity, information about field cancerization, with increased specificity for higher accuracy of diagnosis and delivery of optimal treatment.
Medical writing services were provided by Marianne Pons and Marielle Romet (Santé Active Edition) and funded by Pierre Fabre Dermocosmetique.
Conflict of interest: JM has participated as a consultant and received research grants from Almirall, Leo Pharma, Pierre-Fabre and ISDIN. GP declares no conflict of interest.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize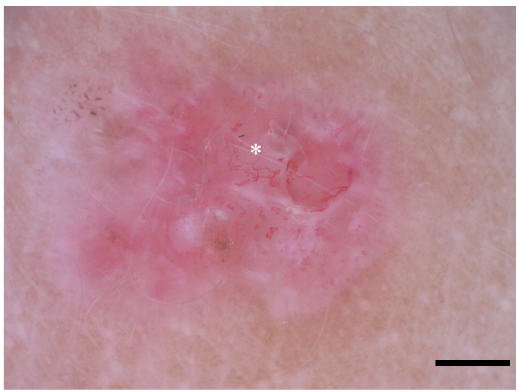 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize