


Department of Dermatology, Center for Chronic Pruritus, University Hospital Münster, Von-Esmarch-Str. 58, DE-48149 Munster, Germany. E-mail: sonja.staender@uni-muenster.de
A 47-year-old man presented with generalized pruritus, which had developed 15 years earlier and was continuously present with exacerbations during the day. The itch had begun on the chest and spread to the entire body. An itch intensity score of 7 on a visual analogue scale (VAS, 0–10) was reported during exacerbations. The patient had no known allergies, rhinoconjunctivitis or allergic asthma. Other than an enlarged thyroid, no other health issues were reported and iodine was the only regular medication.
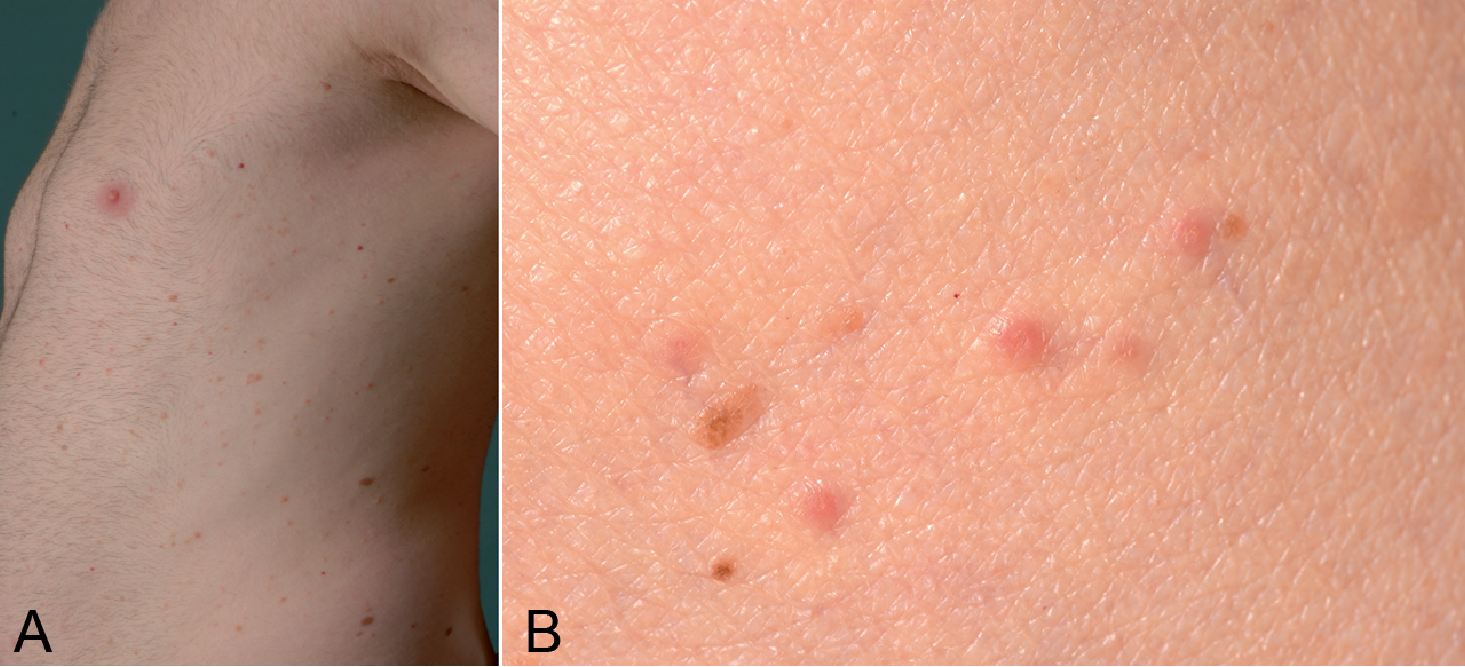
Upon inspection, multiple small isolated skin-coloured papules could be seen, mostly in frontal and lateral aspects of the trunk (Fig. 1).
Fig. 1. (A) Multiple isolated skin-coloured or slightly red itchy flat papules distributed mostly across the frontal and lateral trunk. (B) Close-up of typical lesions seen in the condition shown in A (not the same patient).
Since the onset of the disease 15 years previously the skin condition and the pruritus had been treated intermittently with topical steroids and antihistamine, respectively, with no substantial alleviation of symptoms.
What is your diagnosis?
In 1970, Ralph W. Grover, a dermatologist from New York, USA, reported 6 cases of an itchy papular eruption, which resolved completely in a few weeks (1). Histological examination of the lesion showed acantholytic changes and, as a result, this condition was named “transient acantholytic dermatosis” (TAD).
TAD is characterized by the sudden onset of a monomor-phous papular eruption more commonly affecting older men (2). Inpatients, especially those who are bedridden, are at higher risk of developing this condition (3). Usually the erup-tions can be observed on the trunk, but all body parts may be affected. Differential diagnosis for disseminated papules on the trunk comprises various conditions including, among others, lichen planus, lichenoid drug eruption, histiocytosis, mastocytosis, sarcoidosis or syphilitic rash. Although TAD may be asymptomatic, patients often report severe itching, with heat, sweating and xerosis being common aggravating factors (4, 5). Interestingly, patients report on generalized itching, although only scattered papules are observed. An underlying systemic cause of TAD has not been reported so far; however, haematoproliferative diseases have been linked to TAD and should be taken into account by the attending dermatologist (6). It is disputed whether TAD is a secondary skin condition resulting from intense scratching rather than a primary dermatosis.
Despite its name, TAD may not resolve spontaneously and may persist for many years, as was the case in our patient (5, 7). Interestingly, TAD can be worsened by concomitant inflammatory skin diseases, as well as by skin neoplasms (8).
Focal acantholytic dyskeratosis, as seen in our patient (Fig. 2), are typically found in the histology. Intraepidermal clefting, vesicle formation and a lymphocytic perivascular infiltrate in the dermis may also be observed (2). Five different acantholytic patterns (pemphigus vulgaris-like, Darier-like, spongiotic, pemphigus foliaceus-like and Hailey Hailey-like) have been originally described and may be present in the same individual (2, 9, 10). Additional histological patterns were reported recently, including, for example, a porokeratosis-like pattern, epidermolytic hyperkeratosis, lesions with lentiginous silhouette or dysmaturative foci with keratinocyte atypia (9).
Fig. 2. Focal acantholytic dyskeratosis and perivascular inflammatory infiltrate typical for transient acantholytic dermatosis (TAD).
Therapeutically, treatment of a concomitant skin disease, if present, is essential, since it may trigger TAD. Heat or activities leading to sweating should be avoided, while emollients are useful in preventing xerosis. Topical compounds, such as steroids or calcineurin inhibitors, constitute the first-line treatment regimen. In refractory cases, phototherapy, a systemic retinoid therapy or methotrexate should be considered. Systemic steroids lead often to a rapid improvement; however, relapse is frequent after discontinuation of the therapy (2, 7).


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize